Transcription
Redesign Dental for Maximum EfficiencyMark Doherty DMD MPHExecutive DirectorSafety Net Solutions
Mark Doherty, DMD MPHDentaQuest Institute,Executive Director of Safety Net tive Director of Safety Net SolutionsDental Director at the Dorchester HouseFQHC – 30 yearsChief Dental Officer of CommonwealthMobile Oral Health ServicesChief Dental Officer, TauntonOral Health CenterChief Dental Officer, Trident USAMobile Oral Health ServicesTrustee, Board of Directors ,Massachusetts Dental SocietyNational Governor’s Council on OralHealthChair, Online Safety Net Dental ClinicManual, Steering CommitteeMassHealth Dental Joint Committeefor Federal Remediation Agreement,U.S. Federal District Court;MassHealth Remediation Settlement
Knowing What Success Looks like
Safety Net Solutions Centers ofExcellence
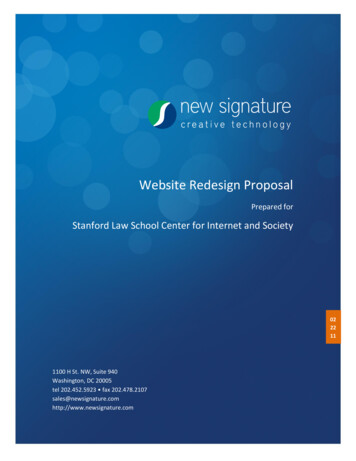
Centers of Excellence ResultsAccessBefore SNSAfter SNSNumber of Visits10,32912,6752,346Unduplicated Patients5,3637,2371,874Number of Procedures24,12239,14815,026Procedures per Visit231.0021%5% pointsBroken Appointment Rate 26%Average of 7 dental programsIncrease/Decrease
Centers of Excellence Results(average per site), cont.FinanceBefore SNSAfter SNSIncrease/DecreaseGross Charges 2,698,844 3,534,817 835,973Net Revenue 1,725,917 2,547,146 821,229Bottom Line- 75,423 319,443 244,020% of sites operating inthe red57%0%
Centers of Excellence Results(average per site), cont.OutcomesBefore SNSAfter SNSIncrease/DecreaseTreatment PlanCompletion Rate16%50%34%# of Sites TrackingCompleted Treatments264Number of Sealants6841,517833
Where Do We Start? with a reality check
Who 1. Teaches us dental business in the Safety Net?2. Gives us the knowledge and guidance we need to run asound dental department?3. Even defines what a sound dental department would be?4. Gives us the tools, policies and operational strategies weneed?5. Defines how many dental visits we should have?
Who 6.Defines the types of dental services we should provide ?7.Describes how to determine a nominal dental fee?8. Teaches us how to create the sliding fee schedule indental?9. Defines how to create a scope of project (SOP) in dentaland then . what our correct scope of service should bewithin that SOP?10. Determines and shares with us what each service weprovide in dental will cost us?
The answer
Five Domains to Understand and Own1Access2Finance3Outcomes4Quality5Governance
MEDICALDENTALAre Different!Different Care Plan and Different Business Plan
MedicalDental80% of clinic volume20% of clinic volume80% of visits similar80% of visits varied80% of visits shorter80% of visits longer80% of billing similar80% of billing varied80% of visits diagnostic80% of visits treatment80% of RVU similar80 % of RVU different100% of governance isdesigned around medical0% of governance is designedaround dentalEMR siloEDR siloFamiliar with medical modelNot familiar with dental modelConfident leadershipLack of confidence
Top Priorities for Dental1.2.3.4.5.6.7.8.9.10.Understanding What Success Should Look Like in DentalCompiling data that is: Accurate, Meaningful and TimelyComputing and understanding your actual “Capacity”Setting clear Goals, Roles, Responsibilities and TimelinesUtilizing the dental schedule strategicallyHaving the right policy for “Everything”Owning management of No-Shows and EmergenciesCreating a “Culture of Accountability”Executing a CQI and QA SystemWhat your own Executive Leadership should look and feellike to best enable and support Dental
Administrator’s Top Priorities for Dental1.2.3.4.5.6.7.8.9.10.11.Defining Your CapacityKnowing What Everybody Else is DoingSetting Productivity Goals in AccessSetting Productivity Goals in FinanceSetting Productivity Goals in OutcomesGetting your Quality House in OrderGetting your Governance House in OrderRunning Dental as a Cost CenterMeasuring and Sharing ALL ResultsSetting Limits of TolerabilityCommunicating Regularly and Meaningfully with Dental
Capacity Quality
Prior to Setting Access GoalsDefine Your Capacity
Defining Capacity/Visits We are limited by our structure Chairs-Rooms-Ops., Dentists,RDHs, DAs, Staff, Hours of OpOur structure determines our capacity not our heartsWe only have 20% of the capacity of MedicineWe cannot be everything to every patient of the CHCEquitable, quality, care mandates that we work withinour capacity We need to decide WHO gets the care When we understand and define capacity we thencreate our business plan
Other Considerations ImpactingCapacity/Visits Our patient population Serve primarily adults, children or a mix? Provider skill levels Students/externs Recent graduates Advanced dentists Staffing Model General Dentists, RDHs, Pediatric Dentists, etc.
The Business PlanThere is Productivity in Access-Finance-OutcomesGOVERNANCEQUALITYRemember: We Get What We MeasureAnd . We Get the Results We TolerateWe now establish productivity goals for theprogram as a unit and for each individualRemembering: Clarity around Goals, Roles,Responsibilities and Timelines establishes howwe will hold the program and each individualAccountable
ClarityAnd by the way:THIS IS HOW WE ARE EVALUATEDOur Program Goals areMy Goals areMy Role isMy Responsibilities areYour Goals, Roles, and Responsibilities areWe need to get this done by
Access Benchmarks1300-16002500-3200encounters/year/FTE hygienistencounters/year/FTE dentist1.7 patients/hour2700 encountersor 13.6 patients/day/dentist/year with 1100 patient base/DMD2.5 ADA coded1 patients/50 min.services/treatment visit9 patients/day/hygienist
Access Benchmarks, cont.15%No-Show rate#New Patients #CompletedTreatments 6%Emergency Rate33% Comp TX. Planis Fair2.5Visit/Year/Patient
Financial Benchmarks 450,000- 500,000Gross Charges/FTEDentist 250,000- 350,000Gross Charges/FTEHygienist 191 Cost/Visit
Benchmark Dental Budget BreakdownTotal Budget: 100% Dental Practice Overhead: 70-85%(77%) See breakdown below* Allocation for Administrative Costs: 5-10% Costs for CEO, CFO, COO, etc. Health Center Support Allocation: 10-20%(23%) Costs for Human Resources, Security, Medical Records, IT, etc.Breakdown of the 70-85% Dental Practice Overhead: Payroll (salary, taxes, & fringe benefits): 68%Building, Utilities, telephone: 9%Dental Supplies: 7%Lab fees: 5%Depreciation: 4% Office Supplies: 2%Repairs: 2%Marketing/Promotion: 1%Recruitment: 1%Continuing Education: 1%
What is Everybody Else Doing?2016 UDS National Data Averages2,614 visits/year/FTE DDS for a panel of 1100 patients2,200 visits/year/FTE RDH2.55 visits/year/unduplicated dental patientrEach dentist treated a panel of1100 patientsUnduplicated dental patients make up 21.9% of all healthcenter unduplicated patients. 2.5 services by ADA code per patient/visit Number of new patients should be similar to the number ofcompleted treatments Cost/dental visit 191.00 Source: https://bphc.hrsa.gov/uds/datacenter.aspx?q tall&year 2016&state
Not Just Visits!AccessAccess is everything associated with the visit:VisitMeasuresAccessOutcomesServices: Type – diagnostic, preventive, therapeutic, specialtyHow many services by ADA code?Charges for the servicesRevenue received for the chargesHealth Outcomes as a result of the servicesQuality of the services and of the customer serviceCompliance with y-Patient CentricHealth OutcomesOral Health OutcomesFinancial OutcomesHRSA Goal OutcomesTreatment Plan Completion OutcomesFocus Population Care Outcomes
Scope of Service BenchmarksService TypeDiagnosticProcedure CodesD0100-D0999% of 2000-D2999D3000-D699933%20%2-6%Oral SurgeryEmergencyD7000-D7999D0140, D91105-10%2-6%(endo/perio/prostho)(excluding D0140)
Scope of Service ExampleCHC Oral Surgery13%5-10%Emergencies14% 6%WHY?
Success in Finance, Outcomes & QualityFinanceVisionFinancial PlanCreation of a high-quality, affordable, oral health programthat documents the improvement of the oral health statusof the patients we treat while being financially responsibleWhat the dental practice needs to accomplishto be financially sustainable, maximize patient access andprovide meaningful quality outcomesIf I had only one report!REMEMBER: Knowing who you are and being able toThe Profitand Lossdefine that with data; defining who you want to be and whatsuccess looks like for you; creating a simple and clear plan toachieve that success and then communicating that plan to theteam and thus creating a culture of accountability is the roadto accomplishing financial success
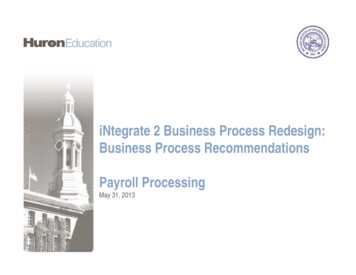
Variance ReportMonth - To - DateJUNEActualActualVarianceBudgetYear - To - DateJUNEBudgetVarianceRevenues:Gross 7,993)Insurance 64,1961,413,315(50,881)Grant RevenueCapitation paymentsInterest/Other IncomeTotal Revenues-Expenses:SALARIES & BENEFITSCOMMISSIONSRENT, BUILDING EXPENSE, OFFICE 7OPERATIONAL 110,500(3,884)PRINTING & ADVERTISINGPOSTAGE & SUPPLIES-17,22418,4171,193INITIATIVES------COMPANY 10,357193,336(205)7,049Total 718)Change in Net 6,960)PROFESSIONAL SERVICES & CONSULTINGMISCELLANEOUSDEPRECIATION34
Common Factors Impacting Finance Not having goals! Not having a Profit and Loss statement Productivity Busters: Empty chairs missedopportunities Reimbursement environment: Low encounter rate orlow fee for service Issues in the billing & collections process (High AR) Fee schedules & SFDS/Nominal fee: Fees below marketrate, nominal fee too low Patient/Payer Mix: high number of uninsured adultpatients
Outcomes HRSA Sealant Measure Compliance for FQHCsChildren seen 0-5 years oldPregnant women seen and treatedChildren seen getting a preventive service# Fluoride Varnish applicationsDiabetic patients with HbA1C 7 seenPatients seen who have not been seen for 12 monthsPatients seen getting a Risk AssessmentPatients with moderate or high risk who lower risk at recare#Sealants providedCompletion of phase 1 treatment 15/12/Demystifying-HRSA-SEALANT-PRESENTATION FINAL.pdf
Phase 1 Treatment Completion What is Phase 1 Treatment? It is also known as “Elimination of dentaldisease” This includes: Oral cancer prevention and earlydiagnosis; prevention education and services;emergency treatment; diagnostic services andtreatment planning; restorative treatment; basicperiodontal therapy (non surgical) and basic oralsurgery that includes simple extractions
Tracking Phase 1 Treatment Completion Create a dummy code in your EDR that will signify that phase 1treatment is complete Phase 1 treatment is complete when the patient has no activedental disease in their mouth; or when that disease is beingactively managed. Note: If the patient receives a prophy, exam, fluoride, andradiographs and has no active disease, the front desk can andshould code for all treatment and the tx complete dummy codeon the same day of service. This patient’s Phase 1 treatment hasbeen completed. Note: If the patient chooses to discontinue Phase 1 therapy,then the treatment would be considered complete. This must beclearly documented in the patient’s chart when the treatmentcompletion dummy code is entered. Educate all dental providers/staff on the proper use of this code Consistent, accurate use of this code is imperative.
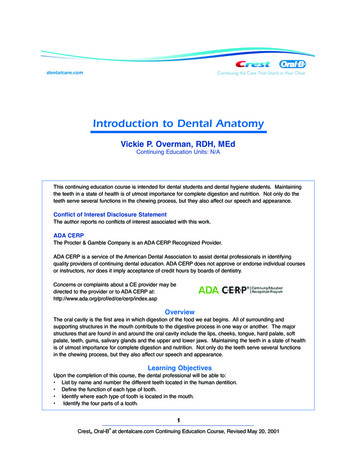
Finding Your Treatment CompletionRate Divide the total number of completed treatment plans (tracked bya dummy code) by the sum of all periodic exams (D0120), oralexams for children under age 3 (D0145), and comprehensiveexams (D0150) for a given time period. (Within 12 months) Thispercentage is your Phase 1 Treatment Completion e 1TreatmentCompletionRatePercentage of phase 1 treatmentplans that are completed within agiven time period. Phase 1treatment all proceduresneeded to help the patientachieve dental disease-free oralhealth.Number of all completedtreatment plans (This #needs to be tracked by adummy code that isentered when all neededphase 1 treatment for thepatient is completed.)Total of all D0120,D0145, and D0150visits. (These are visitswhen the patientreceives a treatmentplan)
Tracking Phase 1 Treatment Completion Setting a Goal: Step 1: Establish your baseline Step 2: Create an initial goal (33% to start) Seek to raise the treatment completion rate by 5%or better in each succeeding 12 month period Step 3: Assess your program to understand thebarriers and work on solutions Step 4: Set your ultimate goal: 75% completion rate
Quality Quality Management System Quality Assurance Policy and Tool Continuous Quality Improvement Policy Dental Quality Compliance Officer Dental Representation on FQHC CQI team Credentialing Policy Privileging Policy/Competencies Policy and Procedure Manual Patient Satisfaction Survey (At least 1X year)
Patient Satisfaction Surveys Can use a paper form – Survey3.pdf Must have a valid # surveys per provider Must report the results to the staff (StaffMeeting) Must act on results: document actions
Guidelines ADA Radiographguidelineshttp://www.ada.org/ /media/ADA/Member%20Center/FIles/Dental Radiographic Examinations 2012.ashx ADA Clinical Practice by-topic American Association of Endodontists:http://www.aae.org/colleagues/ American Academy of Pediatric ion.aspx?orgid 874 Agency for Healthcare Research and Quality (135 dentalguidelines) http://www.guidelines.gov/search/search.aspx?term dentistry ADA code of ethics and conduct e-of-professional-conduct
Issues Most Important to Patients Friendliness of ALL staffTimely appointmentsWait times in the waiting roomProvider listeningProvider addressing their concernsAppearance of the officeNo pain!Understanding the bill!!!Good communication
Governance Compliance with Federal, State and Local Regulations andwith the State Practice Act Quality Compliance Officer Policy and Procedure Manual Credentialing Policies and CEU Compliance Privileging Policy/Competencies Annual Safety/infection Control/Hazardous Waste Training Preparation for a OSV/ Regulatory Site Visit After Hours Coverage Policy Extended Service Hours Malpractice and Liability Policies and Coverage/Gap Ins.? FTCA Deeming/Annual Redeeming/Compliance
Credentialing and Privileging HRSA Pin 2002-22 Requires Credentialing and Privileging ofproviders including dentists. Credentialing is the process of establishing and ensuring that aprovider is qualified to practice in your center. Your health center should own and control the credentialingprocess Privileging is establishing the right of a provider to performspecific procedures The Dental Director should own and control the privileging process Defines, for the incoming dentist, what procedures are allowed atthe clinic and for that dentist Required for FTCA insurance and many other malpractice insurers
Operational Site Visit DentalCompliance IssuesAccessible Hours of Operation/Locations:Health center provides services at times and locations thatassure accessibility and meet the needs of the population tobe served. (Section 330(k)(3)(A) of the PHS Act)After-Hours Coverage: Health center providesprofessional coverage during hours when the center isclosed. (Section 330(k)(3)(A) of the PHS Act)
Operational Site Visit DentalCompliance Issues, Cont.Budget: Health center has developed a budget that reflectsthe costs of operations, expenses, and revenues (including theFederal grant) necessary to accomplish the service deliveryplan, including the number of patients to be served. (Section330(k)(3)(D), Section 330(k)(3)(I)(i), and 45 CFR Part 74.25)Scope of Project: Health center maintains its funded scopeof project (sites, services, service area, target population, andproviders), including any increases based on recent grantawards. (45 CFR Part 74.25)
Operational Site Visit DentalCompliance Issues, Cont.Sliding Fee Discounts: Health center has a system in place todetermine eligibility for patient discounts adjusted on the basis of the patient’sability to pay. This system must provide a full discount to individuals and families with annualincomes at or below 100% of the Federal poverty guidelines (only nominal feesmay be charged) and for those with incomes between 100% and 200% ofpoverty, fees must be charged in accordance with a sliding discount policy basedon family size and income.* No discounts may be provided to patients with incomes over 200% of theFederal poverty guidelines.* No patient will be denied health care services by the health center due to anindividual’s inability to pay for such services, assuring that any fees or paymentsrequired by the center for such services will be reduced or waived. (Section330(k)(3)(G) of the PHS Act, 42 CFR Part 51c.303(f)), and 42 CFR Part51c.303(u))
What is Churning?
Checklist to Dental Redesign Define What Success Should Look Like inDental Gather Data that is accurate, timely andmeaningful Compute and Understand your actual Capacity Set Clear Goals, Roles and Timelines for boththe Dental Team as a whole and Individuals in :Access, Finance and Outcomes Have a policy for “Everything”!!!! Set fees at the usual and customary of themarket rate in your service area
Checklist to Dental Redesign Execute a Quality Management Systemincluding CQI and QA in Dental and in the CHC Create a Dental Culture of Accountability Actively Manage: Broken Appointments/LastMinute Cancellations; Self Pay Patients; FrontDesk; Payer Mix ; Customer Service; Billing;Emergencies; Priority Populations; Scope ofService Use the Dental Schedule Strategically! Know what your own Leadership should lookand feel like to best enable/support Dental
SNS Technical Assistance Resources Dental Policy & ProcedureManual Template Sample Clinical Protocols Sample Dental JobDescriptions Sample Broken AppointmentPolicies Scripting for CHC Dental Staff Profit & Loss Budget VarianceTool Financial and ProductivityGoals Tool Payer Mix Projection Tool Dental Program PerformanceTracking Tool Productivity BenchmarkGuide Sample Scheduling Policy Sample Emergency Policy Sample Quality AssurancePolicy And much, much ntaquestinstitute.org/learn/safety-net-solutions
NNOHA Technical Assistance Programs Website: www.nnoha.orgDental Clinic Operations Manual/PublicationsWebinarsPromising PracticesAnnual ConferenceNational Oral Health learning InstituteListservSpeaker’s BureauConsultation/Referral
SNS Online Practice Management Series -practicemanagement-series) Developing Billing Excellence Fee Schedules, Sliding Fee Scales, & Management of the Self-PayPatient Safety Net Dental Program Finance and Productivity: Your Missionand Your Mar
Massachusetts Dental Society. National Governor’s Council on Oral Health. Chair, Online Safety Net Dental Clinic Manual, Steering Committee MassHealth Dental Joint Committee for Federal Remediation Agreement, U.S. Federal District