Transcription
Acquired brain injuryThe factsThe practical guide to understanding and responding toacquired brain injury and challenging behavioursFifth edition(2016)
Contents The factsQueensland:PO Box 3356, South Brisbane QLD 4101New South Wales:PO Box 698, Epping NSW 1710Freecall: 1800 673 074F: 07 3137 7452E: info@synapse.org.auW: synapse.org.auThe facts is produced by Synapse.Synapse is dedicated to improving thequality of life of people living with andaffected by acquired brain injury, orpeople whose behaviour challenges ourunderstanding.Visual difficulties:Visit synapse.org.au to view the onlineversion which can be enlarged on screen.Disclaimer:While all care has been taken to ensureinformation is accurate, all informationin this publication is only intended as aguide, and proper medical or professionalsupport and information should be sought.Synapse will not be held responsible forany injuries or damages that arise fromfollowing the information provided. Materialwithin does not necessarily reflect thepolicies of Synapse or the staff and Boardof Management. References to otherorganisations and services do not imply anendorsement or guarantee by Synapse.Synapse acknowledges the fundingreceived to deliver our services.Australian GovernmentDepartment of HealthDepartment of Social ServicesNSW GovernmentFamily & Community ServicesQueensland GovernmentDepartment of CommunitiesISBN 978-0-9581040-2-9SynapseIntroduction04 About acquired brain injury04 Understanding the brain06 Types of injury06 Children and brain injury: an introduction10 StrokeIn the hospital12 Brain injury: treatment and diagnosis16 Brain injury diagnostic tests and scans18 Recovery from a brain injury19 Why predictions of recovery are difficult20 Emotional recoveryRehabilitation and recovery21 What is rehabilitation?22 Rehabilitation tips24 The post-rehabilitation slump25 Steps to independence27 Hope after brain injury28 Family guide to a low cost rehabilitationprogram30 Steps to a healthier brain32 Complimentary therapies33 Pets as therapy
Effects of acquired brain 636466666768707274Information for families and carersImpact of brain injuryPhysical effectsCognitive effectsEmotional and behavioural effectsSocial and relationship changesAttention and concentration after a brain injuryManaging fatigue after a brain injurySleeping disorders after a brain injuryBalance problems and dizziness after a brain injuryCoping with memory problems after a brain injuryProblems with organisingCommunication disorders after a brain injurySensory and perceptual skillsVisual disordersHearing problems after a brain injuryAnosmia – loss of sense of smellHeadaches and other painsEpilepsyChallenging and complex behavioursProblems with angerImpaired self-awareness and brain injurySelf-centrednessImpulsive behaviourSexual changesMental healthStress, anxiety and brain injuryPanic attacksDepression after a brain injurySuicide, depression and brain injuryBrain injury and mental illness (dual diagnosis)Alcohol and other drugs after a brain injury75 The importance of families after brain injury75 The impact of brain injury on families andrelationships76 Family resilience following brain injury77 Coping with grief and ambiguous loss78 The impact of caring for someone with brain injury80 Self-care strategies for carers81 Domestic violenceIn the long term82 Accommodation optionsYoung people in nursing homesReturning to workReturning to studiesAdvocacyWhat to do when they don’t believe you have abrain disorder93 Potential future medical problems848587899194Glossary98About SynapseAustralian network of brain injury associationsQLD SynapseTel1800 673 074Email info@synapse.org.auWeb synapse.org.auVICBrainLink ServicesTel1800 677 579Email admin@brainlink.org.auWeb brainlink.org.auTAS Brain Injury Association of TasmaniaAUS Brain Injury AustraliaTel03 6278 7299 / 1800 242 827Tel02 9808 9390Email enquiries@biat.org.auEmail admin@braininjuryaustralia.org.auWeb biat.org.auWeb braininjuryaustralia.org.auNSW SynapseTel1800 673 074Email info@synapse.org.auWeb synapse.org.auSABrain Injury South AustraliaTel1300 733 049Email info@braininjurysa.org.auWeb braininjurysa.org.auWAHeadwestTel08 9330 6370Email admin@headwest.asn.auWeb headwest.asn.auNTSomervilleTel08 8920 4100Email scs@somerville.org.auWeb somerville.org.auACT Hartley lifecareTel02 6282 4411Email enquiries@hartley.org.auWeb hartley.org.au
IntroductionAbout brain injuryAlmost everything we do, say and think is controlled by our brain, sowhen our brain is injured it has the potential to affect every aspect of life.This resource has been preparedto inform and assist thosewho have experienced a braininjury, their family, and supports – aswell as being a resource for medicalprofessionals.It has been designed to not onlygive an overview of the types andimmediate impacts of brain injury,but also practical information andstrategies on how injury affects broadareas of life.While this resource features a widerange of acquired brain injuries anddegenerative neurological disorders,much of the content is directed atacquired injuries. The strategies andinformation given in this resourcemay be useful in responding to bothacquired injuries and disorders.If you would like to speak tosomeone about this information inthis resource.To find support call,Synapse Options on 1800673 074. Alternatively, visitsynapse.org.au.About acquired brain injury (andneurocognitive disorders)The term brain injury includes anumber of conditions and braindisorders that typically result in a levelof neurocognitive impairment, and aredistinct from intellectual disability.Acquired brain injury (ABI) generallyrefers to injuries sustained after birth,such as through stroke, hypoxicinjury (near drowning, attemptedsuicide, etc.) and traumatic braininjury (TBI) (Motor vehicle accidents,falls, sporting injuries, assault etc.).Injury to the brain also occursthrough degenerative disorders(Alzheimer’s disease, Parkinson’sdisease; multiple sclerosis etc.), braintumours, infections or brain diseases(eeningitis, encephalitis, etc.).Degenerative brain disorders canhave similar physical and cognitiveimpacts to ABI; however, the differentcharacteristics of these conditionsrequire specialist support.Some injuries sustained duringpregnancy, such as Foetal Alcohol4 Synapse Brain Injury Association of Queensland synapse.org.auSpectrum Disorder (FASD), have alsobeen classified as an ABI.Brain injury is common in Australia,with around one in 45 Australians(432,700 people) acquiring abrain disorder (AIHW, 2007).The Queensland Governmentacknowledges that one in 12 areaffected in some way by brain injury.Brain injuries are often called thehidden disability because, althoughpeople can experience significantchanges in how they think, feel andrelate to others, there may be nooutward physical signs of injury.Problems can be easily ignoredor misunderstood by others. Theimpacts of brain injury are alsoexperienced by family and friends,particularly when the injury hasresulted in personality or behaviourchange.Synapse will often refer to theterm ‘brain injury’ as a collectiverepresentation to inclusive of bothacquired injuries and neurologicaldisorders.
Understanding the brainThe long-term effects of a brain injuryor disorder are different for eachperson, and will vary depending onthe type of condition, the natureand location of the injury, and otherfactors. For example, while disorderssuch as Parkinson’s disease andmultiple sclerosis typically impact thebody’s ability to control movement,other brain injuries may have agreater impact on cognition, orpersonality and behaviour may beaffected more. The impacts of braininjury can cause:The brain controls and coordinateseverything we do: movements,feelings, thoughts, breathing andbodily functions.The brain is made up of billionsof nerve cells that communicatethrough electrical and chemicalactivity. It weighs around 1.3 kgand is cushioned within the skull bycerebrospinal fluid that circulatesaround the brain through a series ofcavities called ventricles.The brain makes up only two percent of the body’s weight, but uses20 per cent of the oxygen supply andblood flow. Brain cells are quite fragileand need protection from trauma,pressure, infection, poisoning or lackof oxygen. They begin to die if theydo not receive oxygen after three tofive minutes.The brain is divided into a number ofparts, which have specific functionsand are designed to work together.Physical effects: movement disorders and paralysis dizziness and balance problems epilepsy and seizures eyesight, hearing and speechproblems loss of taste and smell headaches chronic pain fatigue and sleep disorders hormonal changes.Cognitive effects: memory problems difficulty solving problems poor concentration and attention reduced ability to organise andplan lack of initiative and motivation lack of insight and awareness, andpoor judgement.Personality and behaviour change: irritability, anger and easily stressed depression slowed responses and poor socialskills impulsive behaviour and/or a lackof emotional control disinhibition.Secondary effects – the interactionof impacts can result in additionalsecondary changes such as: changes to living arrangements reduced or changed socialnetworks different vocational capabilities altered relationships and familydynamics.Hemispheres and lobes of thebrainThe largest part of the brain is dividedinto two halves, with the left halfcontrolling the right side of the bodyand the right half controlling the leftside of the body.These hemispheres will be moredominant for certain activities.For example, the left hemisphereis mainly involved with speech,language, reading and writing, whilethe right hemisphere is predominantlyfocused on visual perception, andinterpreting nonverbal information.Each hemisphere is divided into fourlobes:Frontal lobes are involved withproblem-solving, planning, makingjudgements, abstract thinking andregulating emotions and impulses.Marked changes in personality andsocial skills can occur from damageto this area.Parietal lobes are involved inmonitoring sensation and bodyposition, understanding time,recognising objects, reading andjudging the position of objects in theenvironment.Occipital lobes receive and interpretvisual information from our sensesincluding colour, size, shape anddistance.The cerebellum is located atthe back and below the mainhemispheres of the brain. It controlsbalance and the muscle coordinationneeded for large body movements.It processes information about howfast, how hard, how far and in whatdirection body parts are moving.The brain stem stem connectsthe brain to the spinal cord andregulates basic activities such aswakefulness, breathing, swallowing,eye movement, body temperatureand heart activity.This brief introduction to the brainreveals not only why the brain is sovulnerable to injury, but also why theeffects of a brain injury can be sovaried. Each part of the brain dealswith different aspects of what wethink, feel and do; so injury to specificareas causes many different effects.The brain can be injured as a result ofmany things; a car accident, stroke,alcohol or drug abuse, tumours,poisoning, infection, disease, neardrowning, haemorrhage, AIDS,and disorders such as Parkinson’sdisease, multiple sclerosis, andAlzheimer’s disease.The good news is that the brain doeshave a limited ability to heal itselfand there are many rehabilitationstrategies to compensate for lostskills and abilities. Read more in therehabilitation and recovery section.Temporal lobes are involved inreceiving and processing sounds,visually recognising objects, andmemory and learning. The temporallobes are also involved in personality,emotions and sexual behaviour.synapse.org.au Brain Injury Association of Queensland The facts 5IntroductionEffects of a brain injury
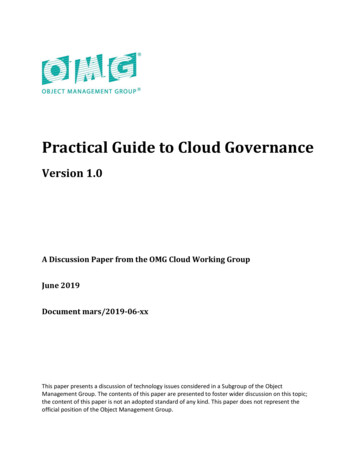
IntroductionTypes ofbrain injuriesand disordersHypoxicLack of oxygene.g. drowning, self-harmConcussionStrokeEpilepsyTraumatic brain injury(TBI)Traumatic brain injury has been defined as ‘an injury to thebrain resulting from an externally applied mechanical forcethat affects the brain and leads to loss of consciousnessor coma’ (Kay and Lezak, 1990).TBI is caused by either a blow to the head or by the headbeing forced to move rapidly forwards or backwards.Brain tissue may be torn, stretched, penetrated, bruised orbecome swollen. Oxygen may not be able to get throughto the brain cells and there may be bleeding.Common causes include motor vehicle accidents, assault,falls, sporting accidents, domestic violence, and babiesbeing shaken. The effects can be temporary or permanent,and range from mild injury, such as being momentarilystunned while playing football, to a very severe injury thatmay cause prolonged loss of consciousness.Apart from the injury to the brain caused by the initialtrauma, there are secondary effects that can arise frombleeding, bruising, lack of oxygen and increased pressurewithin the skull.Hypoxic/anoxic braininjury (lack of oxygen)Brain injury can occur when there is a reduction in(hypoxic) or complete lack of (anoxic) oxygen supply tothe brain. Oxygen is crucial to the brain as it is used tometabolise glucose, which provides energy for all bodycells. Brain cells are sensitive to the effects of restrictedoxygen supply and can die within minutes of oxygenrestriction. The immediate outcome of severe oxygenrestriction is often coma and in very severe cases braindeath.Causes include stroke, near drowning, heart attack,drug overdose, strangulation, severe asthma, accidentsinvolving anaesthesia, and carbon monoxide inhalationand poisoning. Hypoxia can also occur as a secondaryinjury following a TBI (e.g. When there is serious bloodloss resulting in low blood pressure, or as a result of brainswelling that restricts oxygen supply to areas of the brain).Recovery is similar to that of other types of brain injury,but because a hypoxic injury usually results in widespreadinjury to the brain outcomes are likely to be lower thanother brain injuries.6 Synapse Brain Injury Association of Queensland synapse.org.au
IntroductionDegenerativee.g. Alzheimer’s disease, Parkinson’sdisease, multiple sclerosisBrain tumourTraumatic brain injurye.g. motor vehicle accidents, falls, assaultDegenerative conditionsThere are a number degenerative conditions which involvebrain impairment. The more commonly known of theseare multiple sclerosis, Parkinson’s disease and Alzheimer’sdisease.In multiple sclerosis, nerve cells die when the Myelin isremoved. Myelin is a fatty coating that acts in a similarway to the plastic insulation on electrical wiring. Theexact cause is unknown, and there is no cure, althoughtreatments exist that can reduce the symptoms.Parkinson’s disease results from the loss of cells invarious parts of the brain, including an area that createsdopamine. Loss of dopamine causes neurons to firewithout normal control, leaving people less able to director control their movement. The exact cause of Parkinson’sdisease is unknown, and the single biggest risk factoris advancing age. The effects include slowness ofmovement, rigidity, tremors and balance problems.Alzheimer’s disease is the most common type ofdementia, accounting for around 50 per cent to 75 percent of dementia cases worldwide (AIHW, 2012 ). Thecauses are poorly understood, but genes play a majorrole and there is no cure. Plaques and tangles in the brainusually develop later in life and lead to problems withshort-term memory, disorientation, mood swings andbehavioural issues. The average life expectancy is three tonine years after diagnosis.Infection or diseasee.g. meningitis, encephalitisBrain tumoursBrain tumours can restrict blood supply to other cells ormay squash cells through exerting physical pressure uponthem. Infectious substances may cause cell death throughexerting pressure if the brain swells (encephalitis) or thetissue surrounding the brain swells (meningitis), or may killcells through direct infection. Viral infections may result ina widespread injury that can appear as fatigue disorderssuch as chronic fatigue syndrome.More information can be found in our factsheets at synapse.org.auReferences: AIHW (2012) Australian Institute of Health and Welfare 2012.Dementia in Australia. Cat. no. AGE 70. Canberra: AIHW.AIHW (2007). Australian Institute of Health and Welfare. Disability in Australia:Acquired brain injury, Bulletin 55, Canberra: AIHW.Kay, T., and Lezak, M. D. (1990). The nature of head injury. In D. W. Corthell(Ed.), Traumatic brain injury and vocational rehabilitation (pp. 21-65).Menomonie, WI: University of Wisconsin Stout, Research and Training Center.synapse.org.au Brain Injury Association of Queensland The facts 7
IntroductionChildrenand brain injury:an introductionOne of the most important differences between children and adults who acquire abrain injury is that a child’s brain is still developing.After a brain injury, rehabilitation for adults primarilyfocuses on relearning lost skills. However, a childmay be yet to learn many skills, so extra support isneeded to ensure development progresses as normally aspossible.skills have already been developed. However, a child’s ageonly has a limited impact on recovery, and the key factorsare still the severity and type of brain injury, how supportivethe family is, and rehabilitation and support at school.Predicting the degree of recoverySensory and motor skills: a child might either lose somepreviously acquired skills, or have difficulty learning newskills such as holding a pen, drawing, using a keyboard,constructing and manipulating objects, using cutlery,getting dressed, recognising objects and a variety ofother hand-eye coordination activities. Other problemsmay involve mobility, balance and coordination orswallowing and speech difficulties. Professionals suchas physiotherapists, occupational therapists and speechpathologists play an important role in the assessment andrehabilitation of sensory and motor disorders.Predicting how much recovery will occur after a brain injuryis always difficult, regardless of the cause. It becomeseven more so for children as specific problems may onlybecome apparent at certain stages of development. It isimportant to provide plenty of support to prevent the childlagging behind their peers in key areas.It was thought that younger children made a greaterrecovery due to neural plasticity – the ability of thedeveloping brain to reorganise itself. Unfortunately,research suggests this isn’t the case. Children are morevulnerable after a brain injury and will take longer torecover (Catroppa et al., 2008).In general, it appears that the earlier a brain injury occurs,the more impact it will have for the child. Recoveryappears to be an easier process when basic functionalEffects of a brain injuryCognitive abilities: a brain injury may lead to a generaldecline in a number of intellectual abilities. However,similar to adults, a child may be within the normal rangeon measures of intellectual functioning and yet displaysignificant problems in specific areas of attention, memory,language, visuospatial and executive functioning.8 Synapse Brain Injury Association of Queensland synapse.org.au
with caring families and school communities, coupled withpersonal skills that enable young people to develop selfesteem and confidence. It is also helpful to have a stablefamily structure, open lines of communication, a proactiveapproach to solving problems and a good relationship withan adult outside the family – someone who believes in theyoung person.Social, behavioural and emotional issues: a child canexperience difficulties relating to peers and siblings andhave difficulty joining group activities. They can demand alot of attention from parents or teachers, and have difficultyfollowing rules and instructions. Behavioural problemsinclude: depressed or anxious mood, hyperactivity,distractibility, impulsivity, poor judgement, reduced controlof anger and frustration, mood swings, aggression, sleepdisturbance and poor motivation. There are variousrehabilitation strategies to help children manage theiremotions and behaviour. These should be introduced asearly as possible.Challenging behaviours are a normal part of growing up aschildren test their boundaries. While the effects of a braininjury can further complicate this, the appropriate adultresponse to this behaviour is the same: The best basis for helping children is a loving, caringrelationship, so it is important to see children asseparate from their behaviour and use language suchas: ‘I love you, but I don’t like what you’re doing’. Structure and routine become even more importantafter brain injury. Specific rules and structures need tobe set up for particular situations and rehearsed eachtime a similar situation comes up. Children will be encouraged to behave well whenpraised or rewarded. Challenging behaviour should notbe rewarded. Instead, adults can help children to learnfrom experience by talking about what he or she didright or wrong, and how there might be other ways ofresponding. Children will also learn to get along with others andhandle difficulties by watching how adults behave. Most importantly, young people with a brain injury mayneed very concrete, detailed and explicit instructionsand rules about what to do in particular situations.Brain injury and your child’s developmentA brain injury can disrupt normal development in termsof language and speech, learning, memory, behaviour,movement, balance and coordination. Children with a braininjury will often make good progress, even if it is limited tosome extent by the injury. Support and assistance tailoredto each child’s needs will ensure they develop to their fullestability. This is especially true at school where there can bea tendency to underestimate the degree of support neededwithin the education system.Balancing risk & independenceOne of the important things parents do is to help youngpeople learn to manage and judge risk. It is important toencourage independence and allow a manageable elementof risk, but a child’s brain injury can cause problems withanticipating danger, judging risk, or showing self-control.Research shows that important factors in protecting youngpeople from high-risk activities include a strong connectionChallenging behavioursFor more information, view our parents’ guideat synapse.org.auReference: Catroppa, C., Anderson, V. A., Morse, S. A., Haritou, F., andRosenfeld, J. V. (2008). Outcome and Predictors of Functional Recovery 5Years Following Pediatric Traumatic Brain Injury (TBI). Journal of PediatricPsychology, 33(7), 707-718. doi:10.1093/jpepsy/jsn006synapse.org.au Brain Injury Association of Queensland The facts 9IntroductionLanguage and communication: many childrenexperience receptive problems which involve difficultyprocessing different parts of spoken or written information.Comprehension problems occur when a child cannotunderstand what he or she is reading or what anotherperson is saying. Spoken or written language expressionmay be affected in terms of pronunciation, fluency,grammar, intelligibility or the meaning and retrieval of words.
IntroductionStrokeA stroke is an interruption of blood supply to part of the brain. Ifarteries become blocked, bleed or break, then the brain tissue thatwas being nourished deteriorates.When this lack of blood supply occurs to the heartit is called a heart attack. When it occurs in thebrain it is called a stroke.Types of strokeEmbolism is where an object, most commonly a bloodclot, blocks an artery. These clots can occur in other partsof the body then break up and travel to the brain wherethey lodge in the brain’s smaller blood vessels.Thrombosis is where there is a gradual closure of a bloodvessel. In a stroke, this is most commonly fatty lipidscalled plaques building up on the walls of blood vesselsand restricting blood flow. As a result symptoms usuallydevelop slowly but may be rapid in some cases.Haemorrhage is severe bleeding. There are two kindsthat can cause a stroke. An intracerebral haemorrhage iscaused by a ruptured artery leaking blood directly into thebrain. A subarachnoid haemorrhage occurs on the surfaceof the brain and the blood fills the space around the brainand creates pressure.Effects of strokeThe after-effects of a stroke vary widely for each strokevictim as different parts of the brain are responsible forthought processes, comprehension, movement and oursenses. The extent of blood shortage also determines theeffect of the stroke. A stroke may result in paralysis, lossof feeling, communication difficulties, visual problems andmany other issues depending on which part of the brain isaffected.TreatmentSurgery, drugs, acute hospital care and rehabilitation areall accepted stroke treatments depending on the type ofstroke.An example of surgery is a carotid endarterectomyto remove plaque if a neck artery is blocked. Aspirinis a common drug used for thinning the blood. Othermedications aim to dissolve clots that lead to stroke. Newtechniques continue to arise, such as cerebral angioplastywhere balloons, stents and coils are used to dilate smallintracranial arteries.10 Synapse Brain Injury Association of Queensland synapse.org.au
IntroductionRecoveryGenerally speaking, the brain does not regenerate if braintissue dies after an embolism or thrombosis. The individualmay regain some function after the pressure caused by thebleeding (haemorrhage) has decreased.Recovery after a stroke depends ona number of factors including the: type and severity of the stroke part of the brain involved extent and nature of the damage existing medical problems type of treatment andrehabilitation.Recovery usually involves a lot of relearning of activitiessuch as walking and talking. This learning can becomplicated by the fact that many people have troubleconcentrating after a stroke.InfectionsInfections, such as meningitis and encephalitis, can injurethe brain and even lead to death very quickly, so urgentmedical attention is critical.Meningitis is an inflammation of the protectivemembranes that cover the brain and spinal cord, leadingto high fever, headaches, sensitivity to light, confusion,and occasionally seizures. Vaccination of young childrenis strongly recommended as a preventative measure. Themost common causes of meningitis are viruses, bacteria,fungi, and protozoa.Encephalitis is a swelling of the brain caused byviruses or bacteria. This can occur through insectbites, contaminated food, or other existing infectionsand diseases. Symptoms include an unsteady walk,sleepiness, confusion, fever, headache, light sensitivity,seizures, paralysis and impaired cognition.EpilepsyEpilepsy involves recurring brief episodes of abnormalelectrical activity in the brain leading to either uncontrolledconvulsions and unconsciousness, or just a momentaryloss of awareness. The exact cause is unknown, butthe majority of recurring seizures can be prevented bymedications. While epilepsy is a brain disorder itself, it canalso be caused by other disorders such as a TBI or stroke.More information on injury on stroke can befound in our fact sheets at synapse.org.ausynapse.org.au Brain Injury Association of Queensland The facts 11
In the hospitalIn the hospitalIt is important to become familiar with the hospital’s departments, wards and keystaff providing treatment for acquired brain injury.Patients presenting athospital with a brain injuryare typically admitted to theneurosurgical unit under the careof a neurosurgeon. A number ofspecialists may attend patients withmultiple injuries. The specialist incharge can vary depending on theneeds of the patient. For example, incases of bone injury, an orthopaedicsurgeon will be in charge, but thepatient will have access to a range ofspecialists according to their needs.A registered nurse (RN) is alwaysavailable and assigned to patients.Understanding medicalinformationUnderstanding medical terminologycan be difficult, especially duringtimes of stress. It is important forpeople to ask questions in orderto understand what is happening.People may prefer to direct suchquestions to a person with whomthey feel comfortable, such as amember of the nursing staff, a doctoror an allied health professional. Wehave included a glossary of terms atthe back of this resource.It is common for hospitals to holdmeetings with family members andvarious members of staff involved inthe patient’s care. Family memberscan request a meeting throughthe social worker if it has not beenoffered. These meetings providea good opportunity for relativesto direct questions to specificprofessionals. It may be helpful forthose attending a meeting to writedown the most important points orquestions they wish to raise ahead oftime.AdvocacyCoping strategiesFamilies are entitled to ensure thattheir family member’s best interestsare being served. Most hospitalsprovide support for families to obtaininformation and make decisionsabout a patient’s care. The personproviding this support is often a socialworker, who will advocate for thepatient on the family’s behalf.The following ideas are designed tohelp friends and relatives come toterms with the traumatic experienceof having someone sustain a braininjury: acknowledge personal reactions tostressful experiences reduce sources of stress wherepossible accept support: whether it betalking things over or getting helpwith the housework talk with other people about yourfeelings and experiences as thiscan help you process what hashappened be aware that other familymembers may deal with thesituation differentlyInforming the patientThe focus of family members at thistime is typically the wellbeing of theirloved one, and they may be reluctantto convey potentially upsettinginformation to the injured person.Conversations about the pe
Contents The facts In the hospital 12 Brain injury: treatment and diagnosis 16 Brain injury diagnostic tests and scans 18 Recovery from a brain injury 19 Why predictions of recovery are difficult 20 Emotional recovery Rehabilitation and recovery 21 What is rehabilitation? 22 Rehabilitation tips 24 The post-reha