Transcription
Hospital Inpatient QualityReporting Program:Part 1 of 4: A Detailed Review of the Final CMS FY 2014 IPPS Rule-1-
Welcome and IntroductionsVicky Mahn DiNicola RN, MS, CPHQVP Research and Market InsightsMidas XeroxFollow me at https://twitter.com/MidasXerox to keep up withRegulatory Changes Impacting Quality Reporting Requirements!Questions regarding this briefing may be submitted directly to mein a private email simply by clicking on the comment bubble in thetool bar at the bottom right of your presentation screen, or youmay contact me directly by sending me an email tovicky.mahn@xerox.com-2-
Hospital Inpatient Quality Reporting ProgramIPPS 2014 Final RuleInpatientHospital ramHospital ValueBasedPurchasingProgram-3-
Review ofFinal IPPSRule forFY 2014CMS-1599-FCMS-1455-FPosted toFederal RegistryAugust 19, 2013-18956.pdf-4-
Timelines for Updated TechnicalSpecifications Manual for InpatientHospital Quality Reporting ProgramManualVersionApplicable DischargeDatesScheduledRelease4.34.41/1-/014 – 9/30/201410/1/2014 – 6/30/20157/1/20134/1/2014Note: Addendum to Specifications Manual for Hospital InpatientQuality Measures 4.3a applicable with 1/2014 dischargesto be posted late September 2013-5-
Comparing the old with the new-6-
17 Measures Removed from HIQR Program inPrevious Rulings for FY 2015 Payment DeterminationCMS will continue calculations for the “claims based” measures through December 31, 2014 dischargesHospital Acquired ConditionsAHRQ Patient Safety MeasuresForeign Object Retained After SurgeryPSI 06: Iatrogenic PneumothoraxAir EmbolismPSI 11: Post operative Respiratory FailureBlood IncompatibilityPSI 12 Post operative PE or DVTPressure Ulcer Stages III & IVPSI 14 Post op wound dehiscenceFalls and TraumaPSI 15 Accidental puncture or lacerationVascular Catheter-Associated InfectionAHRQ Inpatient Quality IndicatorsCatheter-Associated Urinary Tract InfectionIQI 11 AAA mortality rate (with or without volume)IQI 19 Hip fracture mortality rateManifestations of Poor Glycemic ControlIQI 91 Mortality composite for selected conditionsSurgical Care ImprovementSCIP Inf-VTE-1 Surgery patients withrecommended VTE prophylaxis ordered-7-
Removal of 7 Measures for FY 2016 HIQR Programfor FY 2016 Payment DeterminationAcute Myocardial Infarction AMI-2 Aspirin prescribed at discharge ** AMI-10 Statin prescribed at discharge**Pneumonia PN-3b: Blood Culture Performed in ED prior to FirstAntibiotic Received in Hospital **Heart Failure HF-1 Discharge Instructions ** HF-3 ACEI or ARB for LVSD **Surgical Care Improvement SCIP-Inf-10 Surgery patients with perioperativetemperature management **Structural Measure Systematic Clinical Database Registry for Stroke Care** Note that these measures may still be reported “voluntarily”beginning with 1/1/14 discharges-8-
Five Measures in SuspensionCMS reserves the right toreactive these with a 3month notice prior toresuming data collectionif and when they haveevidence thatperformance isdeclining . IMM-1: Immunization for Pneumonia (beginning with FY 2016 payment determination) AMI-1 Aspirin at Arrival AMI-3 ACEI/ARB for LVSD AMI-5 Beta-blockers at discharge SCIP Inf-6 Appropriate Hair RemovalMeasures remain in suspension(data collection ended 1-1-12)from previous rules beginning withFY 2014 Payment Determination-9-
Summary of 29 Chart Abstracted Measures to be collectedJanuary 1st to December 31st 2014 for FY 2016 PaymentNo new chart abstracted measures required (SCIP Inf-4 modifications)Hospital Inpatient Quality ReportingHospital Inpatient Quality ReportingAcute MI AMI-7a Fibrinolytic agent 30 minutes of arrival AMI-8a Timing of PCI InterventionVTE VTE-1 VTE Prophylaxis VTE-2 ICU VTE Prophylaxis VTE-3 VTE anticoagulation overlap therapy VTE-4 Unfractionated heparin monitored by protocol VTE-5 VTE discharge instructions VTE-6 Incidence of potentially preventable VTEHeart Failure HF-2 Evaluation of LVSFPneumonia PN-6 Appropriate initial antibiotic selectionSurgical Care Improvement Project (SCIP) SCIP Inf-1 Antibiotic 1 hour prior to incision SCIP Inf-2 Prophylactic antibiotic selection SCIP Inf-3 Antibiotics discontinued 24 hrs postop SCIP Inf-4 Cardiac surgery controlled glucose SCIP Inf-9 Postop urinary cath removed day 1 or 2 SCIP-Card-2 Surgery patients on beta-blocker priorto surgery receive during periop period SCIP-VTE-2 Appropriate VTE prophylaxis within 24hours pre/post surgeryGlobal Immunization Measures IMM-2 Immunization for InfluenzaStroke STK-1 VTE Prophylaxis STK-2 Antithrombotic therapy STK-3 Anticoagulation for Afib/flutter STK-4 Thrombolytic therapy STK-5 Antithrombotic therapy hospital day 2 STK-6 Discharged on Statin STK-8 Stroke education STK-10 Assessed for RehabEmergency Department Throughput ED-1 Median time from arrival to departure ED-2 Median time from admit decision to departurePerinatal Care PC-01 Elective delivery prior 39 completed weeks gestationAll Measures above to be validated for Discharges CY Q3 and Q4 2013 andQ1 and Q2 2014 for FY 2016 Payment Determination- 10 -
SCIP-Inf-4 Measure RefinementsBeginning January 1, 2014 Changing SCIP-Inf-4 Controlled 6amGlucose for Cardiac Surgery Patients to“controlled glucose 18-24 hours postcardiac surgery” Must demonstrate that a corrective actionwas taken for patients with a glucose 180 mg/dl) in order to pass the measure HOWEVER the technical specificationsfor the measure appear to be laggingbehind the final rule, as they do not yetindicate what corrective action a hospitalmust take; the allowable values onlyreflect blood glucose levels, timing andexclusion criteriaMidas clients will receiveupdated software inNovember- 11 -
12 Chart Abstracted HIQR Measures tobe Validated for FY 2016 and BeyondHospital Inpatient Quality ReportingAcute MI AMI-7a Fibrinolytic agent 30 minutes of arrival AMI-8a Timing of PCI InterventionHeart Failure HF-2 Evaluation of LVSF CY Q3 and Q4 2013CY Q1 and Q2 2014 3 charts per quarterPneumonia PN-6 Appropriate initial antibiotic selectionSurgical Care Improvement Project (SCIP) SCIP Inf-1 Antibiotic 1 hour prior to incision SCIP Inf-2 Prophylactic antibiotic selection SCIP Inf-3 Antibiotics discontinued 24 hrs postop SCIP Inf-4 Cardiac surgery controlled glucose SCIP Inf-9 Postop urinary cath removed day 1 or 2 SCIP-Card-2 Surgery patients on beta-blocker prior tosurgery receive during periop period SCIP-VTE-2 Appropriate VTE prophylaxis within 24hours pre/post surgeryGlobal Immunization Measures IMM-2 Immunization for Influenza Acute MI Heart Failure Pneumonia SCIP Influenza Immunization (for patientsNOT also in above populations) Up to 12 additional charts forinfluenza immunization if patientsfrom AMI, HF, PN and SCIP qualify No validation required for VTE,Stroke, ED or Perinatal- 12 -
Options for Electronic Reporting inCY 2014 Lieu of Chart AbstractionHospital Inpatient Quality ReportingHospital Inpatient Quality ReportingAcute MI AMI-7a Fibrinolytic agent 30 minutes of arrival AMI-8a Timing of PCI InterventionVTE VTE-1 VTE Prophylaxis VTE-2 ICU VTE Prophylaxis VTE-3 VTE anticoagulation overlap therapy VTE-4 Unfractionated heparin monitored by protocol VTE-5 VTE discharge instructions VTE-6 Incidence of potentially preventable VTEHeart Failure HF-2 Evaluation of LVSFPneumonia PN-6 Appropriate initial antibiotic selectionSurgical Care Improvement Project (SCIP) SCIP Inf-1 Antibiotic 1 hour prior to incision SCIP Inf-2 Prophylactic antibiotic selection SCIP Inf-3 Antibiotics discontinued 24 hrs postop SCIP Inf-4 Cardiac surgery controlled glucose SCIP Inf-9 Postop urinary cath removed day 1 or 2 SCIP- Card-2 Surgery patients on beta-blocker priorto surgery receive during periop period SCIP-VTE-2 Appropriate VTE prophylaxis within 24hours pre/post surgeryGlobal Immunization Measures IMM-2 Immunization for InfluenzaStroke STK-1 VTE Prophylaxis (STK-1 not included) STK-2 Antithrombotic therapy STK-3 Anticoagulation for Afib/flutter STK-4 Thrombolytic therapy STK-5 Antithrombotic therapy hospital day 2 STK-6 Discharged on Statin STK-8 Stroke education STK-10 Assessed for RehabEmergency Department Throughput ED-1 Median time from arrival to departure ED-2 Median time from admit decision to departurePerinatal Care PC-01 Elective delivery prior 39 completed weeks gestation- 13 -
Option to Submit CQM eMeasures instead of paper-based “coremeasures” FY 2016 Payment Determination Submit at least one quarter of data for one or moreof the four eMeasure Sets defined by MeaningfulUse Specifications for Stroke (not including STK1), VTE, ED and Perinatal Care instead of or inaddition to paper-based “core measures” forthese same topics Must continue submission of all other paper-basedtopics for all quarters to meet HIQR requirements No data validation and no public reporting for theinitial year CMS estimates a savings of 800 hours per year indata abstraction for hospitals electing this option- 14 -
Timelines forElectronic SubmissionSubmission for Both EMR and HIQRReporting PeriodsSubmissionDeadlineFor eligible hospitals in 1styear of MU Attestation –CY Q1 2014July 1, 2014For eligible hospitals thatare beyond their first yearof MU program, CY Q1,Q2 or Q3 2014.Submission of Q4 2014data is NOT an option forthe HIQR programNov 30, 2014Hospitals that are voluntarily submittingeMeasure data are highly encouraged tosubmit the same data via chart-abstraction- 15 -
Overview of EHR Incentive ProgramBeginning 2014Stage 1 (In First Year) Electronically report or attest on 16 clinicalquality measures (CQMs) out of 29 CQMsSelected CQMs must cover at least 3 ofthe 6 National Quality Strategy domainsMust submit either CY Q4 2013 or CY Q12014 by July 1st 2014 for EHR incentivepayment BUT must submit CY Q1 2014Stroke, VTE, ED and PC data by July 1st2014 to meet requirements for BOTHEHR and HIQR reporting programsStage 2 (Not In First Year) AND 13 required core objectives5 objectives chosen from a list of 10 menuset objectivesElectronically report 16 out of 29 CQMsSelected CQMs must cover at least 3 ofthe 6 National Quality Strategy domainsMay submit electronic data for any CYquarter in 2014 for EHR incentivepayment BUT must submit CY Q1, 2 or 3data by November 30, 2014 to meetrequirements for BOTH EHR and HIQRreporting programsQuarter 4 data submission too late forHIQR program!AND 16 required core objectives3 objectives chosen from a list of 6 menuset objectives- 16 -
Option to Continue All Paper Submissions forHospital Inpatient Quality Reporting ct-Dec2014Stroke(8 measures)HIQR ProgramVTE(6 measures)ED(2 measures)Perinatal(1 measure)ChartAbstractedSubmissionDeadlinesAug 15th2014Nov 15th2014Feb 15th2015May 15th2015- 17 -
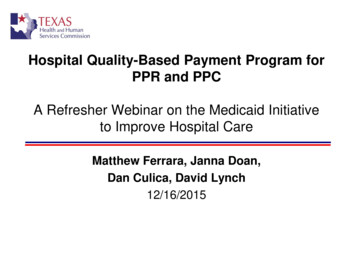
Hospitals in the First Year of Meaningful Use May SubmitElectronic Submissions for Meaningful Use but Q4 2013 datawill NOT meet HIQR RequirementsHospitals in First Year of Meaningful ept2014Oct-Dec2014Stroke(7 measures) **VTE(6 measures)EDSubmit electronically to QNETby July 1, 2014HIQR Program(2 measures)MU EHR ProgramPerinatal(1 AN/A** No electronic submission of STK-1 for CY 2014- 18 -
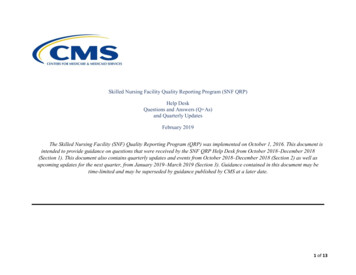
Hospitals in the First Year of Meaningful Use MaySubmit Electronic Submissions for Q1 2014 to MeetBoth Program RequirementsHospitals in First Year of Meaningful Sept2014Oct-Dec2014Stroke(7 measures) **VTESubmitelectronically toQNETby July 1, 2014(6 measures)ED(2 measures)HIQR ProgramMU EHR ProgramPerinatal(1 AN/AN/A** No electronic submission of STK-1 for CY 2014- 19 -
Hospitals in the First Year of Meaningful Use MaySubmit Electronic Submissions for Meaningful Usebut Data Too Late for HIQR RequirementsHospitals in First Year of Meaningful Sept2014Oct-Dec2014Stroke(7 measures) **VTESubmitelectronically toQNETby July 1, 2014(6 measures)ED(2 measures)HIQR ProgramMU EHR ProgramPerinatal(1 AN/AN/A** No electronic submission of STK-1 for CY 2014- 20 -
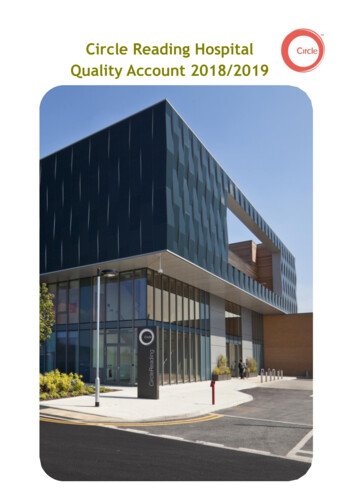
Submission of Electronic Data for Some Topics andPaper Submissions for All Other TopicsHospitals in either First Year or Beyond Year One of Meaningful ec2014HIQR ProgramStroke(7 measures) **Submit electronically to QNETby July 1, 2014VTEMU EHR Program(6 measures) ED(2 measures)Perinatal(1 measure) ChartAbstractedSubmissionDeadlinesAug 15th2014Nov 15th2014Feb 15th2015May 15th2015Sixteen clinical quality measuresin three domains must besubmitted to satisfy the clinicalquality measure reportingcomponent of the Medicare EHRIncentive ProgramThree additional measures mustbe submitted to satisfy the clinicalquality measure requirement inthis example** No electronic submission of STK-1 for CY 2014- 21 -
Submit Electronic Submission for Some Topics andContinue Paper Submissions for All Other TopicsHospitals Beyond Year One of Meaningful ec2014HIQR ProgramStroke(7 measures) **Submit electronicallyto QNET byNovember 30, 2014VTE(6 measures)MU EHR Program ED(2 measures)Perinatal(1 measure)ChartAbstractedSubmissionDeadlinesAug 15th2014Nov 15th2014Feb 15th2015May 15th2015 Sixteen clinical qualitymeasures in three domainsmust be submitted to satisfythe clinical quality measurereporting component of theMedicare EHR IncentiveProgramThree additional measuresmust be submitted to satisfythe clinical quality measurerequirement in this example** No electronic submission of STK-1 for CY 2014- 22 -
Submit Partial Electronic and Continue PaperSubmissions for All Other TopicsHospitals in either First Year or Beyond Year One of Meaningful ec2014HIQR Program Stroke(7 measures) **Submit electronically to QNETby July 1, 2014VTE(6 measures)MU EHR Program ED(2 measures)Perinatal(1 measure)SubmissionDeadlinesAug 15th2014Nov 15th2014Feb 15th2015** No electronic submission of STK-1 for CY 2014May 15th2015Must submit a full yearof data for chartabstracted topics Sixteen clinical qualitymeasures in three domainsmust be submitted to satisfythe clinical quality measurereporting component of theMedicare EHR IncentiveProgramThree additional measuresmust be submitted to satisfythe clinical quality measurerequirement in this example- 23 -
Hospitals Beyond the First Year of Meaningful UseMay Submit All Electronic Submissions LaterHospitals Beyond the First Year of Meaningful ec2014StrokeHIQR Program(7 measures)Submitelectronicallyto QNETby November30, 2014VTE(6 measures)EDOROR(2 measures)Perinatal(1 measure)PaperSubmissionDeadlinesN/AN/AN/AN/AMU EHR ProgramNote that if a hospital submitsmore than one quarter of dataelectronically, only the firstquarter submitted will beconsidered- 24 -
Submission of Data in Q4 2014 too late for FY 2015Hospitals in either first year or beyond the first year of Meaningful ec2014Stroke(7 measures) **VTESubmissiondates to bedeterminedTOO LATE(6 measures)ED(2 measures)MU EHR ProgramPerinatal(1 measure)PaperSubmissionDeadlinesHIQR ProgramN/AN/AN/AN/A- 25 -
Submit BOTH Electronic Data AND Abstracted DataWhen Possible to Support Testing and Validation ofCQM Measure Specifications by CMSHospitals in either First Year or Beyond Year One of Meaningful ec2014HIQR ProgramStrokeMU EHR Program(7 measures) **Submit electronically to QNETby July 1, 2014VTE(6 measures)ED(2 measures)Perinatal(1 measure)SubmissionDeadlinesAug 15th2014N/AN/AN/A** No electronic submission of STK-1 for CY 2014- 26 -
Live ClientsYou must be a Midas Live client for us to submit eMeasure data for you Stage 1: Hospitals that want touse their data for BOTH HIQRand MU Stage 1, should reportdata electronically, rather thanthrough attestation. If you useattestation, it does not fulfill theHIQR requirements. Thedeadline for submission forTWO BIRDS WITH ONESTONE is July 1, 2014. Stage 2: Hospitals that wantto use their data for BOTHHIQR and MU Stage 2, willsubmit 1 or more quarters ofdata (CY Q1, Q2 or Q3discharges) by November 30,2014 (as opposed to the Q32014 HIQR paper baseddeadline of February 15,2015)For clients that have other vendors for MU Clinical Quality Measures but use Midas CPMS or DataVision for paper core measures you will have to let us know if you do notwish us to submit your paper based measures for Stroke, VTE, ED and Perinatal Care.- 27 -
Future eMeasures Being Considered Expect to see a proposal in FY2015 rule to make electronicreporting of selected qualitymeasures mandatory for HIQR Rumors that CMS will proposethat CQM eMeasures to be usedfor VBP by 2017 Five new electronic measuresproposed for “future” years Severe sepsis and septic shockmanagement bundle Cesarean Section Exclusive breast milk feeding Healthy term newborn Hearing screening prior to hospitaldischargeNot yet approved in any final rule- 28 -
Healthcare Associated Infections MeasuresHospital Quality Reporting Program for FY 2016Healthcare Associated InfectionsCentral Line Associated Bloodstream Infection ICU Medical (beginning 1-1-2015) Surgical (beginning 1-1-2015)Catheter- Associated Urinary Tract Infection ICU Medical (beginning 1-1-2015) Surgical (beginning 1-1-2015)Surgical Site Infection (combined total of 10 or more per CY) SSI following Colon Surgery SSI following Abdominal HysterectomyMRSA BacteremiaClostridium difficile (C. difficile)Healthcare Personnel Influenza Vaccinations(Provided October 1st through March 31st)(Date of collection on or before May 15th)No new measuresadded except for additionalstratification groups in CLABSI andCAUTI starting in 2015 and new datefor reporting Healthcare PersonnelInfluenza Vaccination- 29 -
FY 2016 Changes with Validation Templates forCLABSI, CAUTI, MRSA and CDI Validation to evaluate and score eachcase only for the infection for which itwas sampled (note a case could havemore than one of same infection) Beginning with Validation Templatessubmitted May 1, 2014 forward,hospitals may NOT modify the format ofthe validation templates Excluding patients with a LOS 120days from validationCMS is testing a secure file transferproduct called Axway so hospitals canmore easily upload larger files thru aweb-based portal or direct from a clientusing secure file transfer protocol (FTP) Collection for FY 2016 paymentdetermination will only be 3 quarters(CY Q4 2013, and Q1 and Q2 2014) Annual validation sample includes 400randomly selected hospitals Plus up to 200 hospitals sampledbased on targeting criteria 12 cases per quarter will be sampled 2 SSI 5 MRSA or 5 CLABSI 5 CDI or 5 CAUTIFY 2017 payment determination will bebased on 4 quarters (CY Q3 and Q42014 and Q1 and Q2 2015) thereforeonly 9 cases will be sampled perquarter- 30 -
Changes to Quarterly HAI Validation for FY2016 PD starting with October 2013 Events Half the hospitals(300) report on: SSI (2 records for FY 2016, 1 Half the hospitals(300) report on: for FY 2017 and beyond)for FY 2017 and beyond) MRSA (5 records for FY C.Difficle (5 records for FY2016, 3 for FY 2017 and beyond)CLABSI (5 records for FY2016, 3 for FY 2017 and beyond)2016, 3 for FY 2017 and beyond) SSI (2 records for FY 2016, 1 CAUTI (5 records for FY2016, 3 for FY 2017 and beyond)- 31 -
Validation Templates - continuedMRSA and CDICLABSI and CAUTI Sampled hospitals must provideCMS with a list of all MRSApositive blood cultures and CDIpositive stool specimens (bothhospital and community onset) Only hospital onset cases will bepublica
(7 measures) ** VTE (6 measures) ED (2 measures) Perinatal (1 measure) Chart Abstracted Submission Deadlines N/A N/A N/A N/A - 18 - Submit electronically to QNET by July 1, 2014 ** No electronic submission of STK