Transcription
10/4/2014Core Measures:What are the goals and what are our roles?Heart Failure (HF) andAcute Myocardial Infarction (AMI)Core MeasuresTiffany Montoya, PharmD, PhCCardiology Pharmacy SpecialistUniversity of New Mexico HospitalDisclosures None1
10/4/2014Objectives Pharmacists Listthe 3 TJC core measures for Heart Failureand describe how pharmacy can provideassistance to meet them. Technicians Describethe importance of meeting coremeasures for heart failure patients.Self-assessment QuestionsTrue or False Heart failure patients need to have documentation in the hospitalrecord that LVSF was evaluated before arrival, duringhospitalization, or is planned for after discharge to meet coremeasures for CMS and TJC.2. True or False In 2015 CMS and TJC will continue to have the same reportedmeasures for HF and AMI3. True or False Left Ventricular Systolic Dysfunction is defined as LVSF 40%4.True or False Reviewing discharge paperwork and prescriptions is one waypharmacy can aid in optimizing core measures for HF and AMI1.2
10/4/2014Core MeasuresCenters for Medicare &Medicaid services (CMS)The Joint Commission(TJC)2003CMS and TJC–resulted in the creation of one common set ofmeasure specifications documentation known as theSpecifications Manual for National Hospital Inpatient QualityMeasures to be used by both organizationsSpecifications Manual forNational Hospital InpatientQuality MeasuresSpecifications Manual forJoint Commission NationalQuality Core MeasuresCore Measures for Heart FailureMeasureCMSTJCHF-1 Discharge instruction Retired Jan 1, 2014Retired Jan 1, 2014HF-2 Evaluation of LeftVentricular SystolicFunction (LVSF)KeepingKeepingHF-3 ACEi or ARB for LeftVentricular SystolicDysfunction (LVSD)Retired Jan 1, 2015Voluntary for 2014Keepinghttp://www.jointcommission.org/core measure sets.aspx3
10/4/2014Heart Failure Core MeasuresHF-1: Discharge instruction Documentation that patients were discharged home w/written instructions or educational material addressing ALLof the following: activity level, diet, discharge medications,follow-up appointment, weight monitoring, and what to do ifsymptoms worsenHF-2: Evaluation of Left VentricularSystolic Function (LVSF) Documentation in the hospital record that LVSF wasevaluated before arrival, during hospitalization, or isplanned for after dischargeHF-3: ACEi or ARB for Left VentricularSystolic Dysfunction (LVSD) Patients w/LVSD (LVEF 40%) are prescribed an ACEi orARB at hospital dischargePharmacy’s RoleIdentify HF patients on admission to the hospitalCreate order sets with updated guideline driven infoand embed in workflowReview Depart Process and Medication Reconciliationon Discharge4
10/4/2014Acute Myocardial Infarction (AMI)Core MeasuresMeasureCMSTJCAMI-1Aspirin at ArrivalVoluntaryKeepingAMI-2Aspirin Prescribed at DischargeRetired Jan 1, 2015 KeepingAMI-3ACEi or ARB for LVSDVoluntaryKeepingAMI-5Beta- Blocker Prescribed atDischargeVoluntaryKeepingAMI-7Median Time to FibrinolysisVoluntaryKeepingAMI-7aFibrinolytic Therapy ReceivedWithin 30min of Hospital ArrivalKeepingREQUIREDKeepingAMI-8Median Time to Primary PCIVoluntaryKeepingAMI-8aPrimary PCI Received Within90 minutes of Hospital ArrivalKeepingREQUIREDKeepingAMI-10Statin Prescribed at DischargeRetired Jan 1, 2015 Keepinghttp://www.jointcommission.org/core measure sets.aspxPharmacy’s RoleIdentify AMI patients on admission to the hospitalCreate order sets with updated guideline driven infoand embed in workflowReview Depart Process and Medication Reconciliationon Discharge5
10/4/2014Self-assessment QuestionsTrue or False Heart failure patients need to have a documentation in thehospital record that LVSF was evaluated before arrival, duringhospitalization, or is planned for after discharge to meet coremeasures for CMS and TJC.2. True or False In 2015 CMS and TJC will continue to have the same requiredreported measures for HF and AMI.3. True or False Left Ventricular Systolic Dysfunction is defined as LVSF 40%.4.True or False Reviewing discharge paperwork and prescriptions is one waypharmacy can aid in optimizing core measures for HF and AMI.1.Core Measures:What are the goals and what are our roles?Venous Thromboembolism (VTE)Core MeasuresAllison E. Burnett, PharmD, PhC, CACPClinical Assistant Professor- UNM College of PharmacyInpatient Anticoagulation ServicesUniversity of New Mexico Hospital6
10/4/2014Disclosures Anticoagulation Forum National Board (non-profit)Objectives Pharmacists Describethe 6 core measures pertaining tovenous thromboembolism (VTE) Technicians List6 anticoagulants that may be used to preventor treat VTE7
10/4/2014Self-assessment Questions1.True or false The VTE core measures include both prophylaxis and treatmentpopulations2.True or false It is possible to achieve core measures without providing optimal,evidence-based care3.True or false VTE-5, discharge instructions, pertains to all anticoagulants4. True or falseThere are numerous ways pharmacists can aid in optimizingmanagement of VTE prophylaxis and treatmentVTE Core MeasuresVTE-1: VTE prophylaxisVTE-2: VTE prophylaxis in ICU patientsVTE-3: Anticoagulant overlap therapyVTE-4: Heparin per protocol & platelet monitoringVTE-5: VTE discharge instructionsVTE-6: Incidence of potentially preventable VTEhttp://www.jointcommission.org/specifications manual for national hospital inpatient quality measures.aspx8
10/4/2014VTE-1 and VTE-2: ProphylaxisICU and non-ICU populations Patients who receive allowable VTE prophylaxis modalitythe day of or the day after hospital admission OR transferto ICU OR have documented reason no prophylaxis was givenProcess measure- improvement is measuredas increase in the rate of prophylaxis Note measuring a hard, clinical outcome (e.g. rate ofthrombosis)Goal: 100% of eligible patientsVTE 1 & 2: Excluded Populations 18 yearsLength of stay (LOS) 2 or 120 daysComfort measures only (CMO)Clinical trialICD code for: Mental illness (not usually prophylaxed)Obstetrics (not usually prophylaxed)Stroke (included in stroke core measures)VTE (included in VTE core measures 3-6)Surgical (SCIP) patients9
10/4/2014“Allowable” Prophylaxis ModalitiesLow-dose unfractionated heparin (UFH)Low molecular weight heparin (LMWH)- e.g. enoxaparinFactor XA inhibitors Fondaparinux (Arixtra ) Rivaroxaban (Xarelto ) Apixaban (Eliquis )Warfarin (Coumadin )Intermittent pneumatic compression devices (IPC)Graduated compression stockings (GCS)Venous foot pumps (VFP)VTE 1 & 2: Challenges and Pitfalls Caution! VTE prophylaxis measures may lead to “benchmarkingmediocrity” Does not require ongoing assessment throughout admission e.g.-patient receives prophylaxis on days 1 and 2, but it is stoppedfor a procedure and never resumed for remaining 5 days ofadmission (would achieve core measure) Suboptimal prophylaxis regimens may still achieve core measure e.g.-a morbidly obese patient with cancer admitted for sepsis is onlyordered for IPCs (would achieve core measure) “Appropriate” VTE prophylactic strategies mustaddress Type, dose and durationAmin A, et al. J Thromb. Thrombolysis. 2010 Apr;29(3):326-39.10
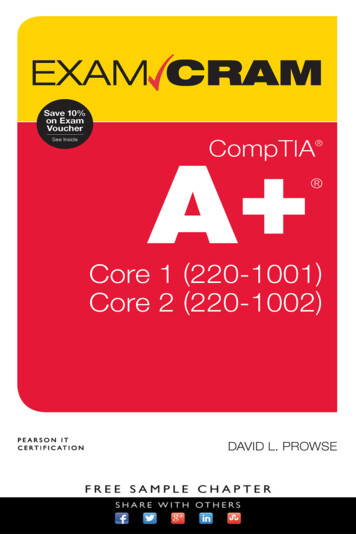
10/4/2014Pharmacy’s RoleEnsure use of standardized VTE prophylaxis protocolContains clinical decision support Makes it easy to do the right thing, hard to do the wrong thing e.g. documenting reason no prophylaxis givenInclude evidence-based prophylactic regimens Ensures appropriate dose of prophylaxisMust employ some type of risk-assessment model (RAM) Identifies patients who do (and do not) warrant prophylaxis Ensures appropriate type of prophylaxis (mechanical vs.pharmacologic)Embed in order sets and workflowPharmacy’s RoleImplementation of ongoing, real-time assessment andreassessment of VTE prophylaxis statusReports or dashboards with current informationClinical pharmacists, interns or technicians shouldmonitor regularlyAids in ensuring appropriate duration of urces/vtguide/index.html11
10/4/2014VTE Prophylaxis DashboardVTE-3: Overlap TherapyPatients with confirmed VTE on warfarin and Receive overlap therapy with parental anticoagulant for 5 daysand until INR 2 OR Have a documented reason overlap therapy was discontinuedbefore 5 days OR Documentation of reason for no overlap therapyExcludes 18 yearsLOS 120 daysCMOClinical trialDischarged to hospice or another hospitalExpiredLeft against medical advice (AMA)Not receiving warfarin therapy (e.g. rivaroxaban, cancer patient)12
10/4/2014VTE-3: Overlap therapyRationale Warfarin has a very slow onset of action Patients with acute VTE must receive rapid-acting parenteralanticoagulation until warfarin is therapeutic Discontinuing overlap therapy before 5 days and INR 2 placespatient at increased risk of recurrent thrombosisProcess measure- improvement is measured as increase inthe % of patients receiving “5 2”Goal: 100% of eligible patients(e.g. those without valid reason for early discontinuation oravoidance of overlap therapyVTE-4:IV Heparin Per Protocol With Platelet MonitoringPatients with confirmed VTE receiving IV UFH ANDplatelet (PLT) count monitored via nomogram or protocolExcludes 18 years, LOS 120 days, CMO, clinical trial Discharged to hospice or another hospital, expired,left AMA Not receiving UFH therapy (e.g. LMWH)13
10/4/2014VTE-4:IV Heparin Per Protocol With Platelet Monitoring Rational Weight-based heparin nomograms/ protocols superior to standarddosing in achieving therapeutic anticoagulation within 24 hours,which reduces risk of recurrent thrombosisStandardized UFH nomograms/protocols reduce the risk of adverseevents, such as bleeding and thrombosisHeparin-induced thrombocytopenia (HIT) occurs in up to 5% ofpatients treated with UFH, and thus PLT count monitoring iswarranted Process measure- improvement is measured as increasein the % of patients receiving UFH and PLT monitoringvia nomogram or protocol Goal: 100% of eligible patientsRaschke RA, Reilly BM, Guidry JR, Fontana JR, Srinivas S Ann Intern Med. 1993;119(9):874Linkins LA, et al. CHEST 2012; Chest 141(2 Suppl):e495S–530S.Pharmacy’s RoleDevelop andimplementUFHnomograms/protocolsObtainapproval fromP&Tcommittee forpharmacy toorder anyneededrelevant labsInvolvepharmacistsinmanagementof VTEpatientsDevelopclinical toolsthat captureinformationpertinent toVTE coremeasures14
10/4/2014Pharmacy’s RoleVTE-5: Discharge InstructionsDocumentation that patient/caregiver was given “copy of WRITTENdischarge instructions or educational materials to take home” thataddress all of the following: Compliance with warfarin and INR checksDietary advice (consistency rather than avoiding vitamin K)Follow-up monitoringPotential adverse reactions and drug interactionsProcess measure- improvement is measured as increase in the % ofpatients with documentation of written discharge instructions forwarfarin being providedGoal: 100% of eligible patients Includes new and experienced patients15
10/4/2014VTE-5: Discharge InstructionsCaution!May lead to “benchmarking mediocrityOnly pertains to warfarinShould strive to include all anticoagulants Newer, less familiar target-specific oral anticoagulants Enoxaparin monotherapy in patients with acute VTE & malignancyVTE-5: Discharge Instructions Pharmacy’s RoleDevelop/identify needed educational toolsProvide patient/caregiver educationTeach RN staff to provide educationAid in development and implementation ofIT tools to capture education activities16
10/4/2014VTE-6: Potentially Preventable VTE Patients diagnosed with an acute VTE that did not receiveappropriate VTE prophylaxis between admission and time to VTEdiagnosis VTE present on admission (POA) excluded Patients with contraindication to VTE prophylaxis excluded Outcome measure Clinical outcome of acute VTE Goal: 0% Requires more in-depth chart review and abstraction Pharmacy may not have a big role in VTE-6Consider multidisciplinary discussion to determine what “wentwrong” and ways to prevent recurrenceReal-time analysis preferable, but may not be feasibleSelf-assessment Questions1.True or false The VTE core measures include both prophylaxis and treatmentpopulations2.True or false It is possible to achieve core measures without providing optimal,evidence-based care3.True or false VTE-5, discharge instructions, pertains to all anticoagulants4. True or falseThere are numerous ways pharmacists can aid in optimizingmanagement of VTE prophylaxis and treatment17
10/4/2014Surgical Care ImprovementProject (SCIP) – What Are theGoals and What Are Our Roles?JAMIE GLASGOW, PHARM.D.MANAGER OF CLINICAL PHARMACY SERVICESLOVELACE MEDICAL CENTER AND HEART HOSPITAL OF NEW MEXICODisclosures None to Report18
10/4/2014Objectives Pharmacists Describethe 8 national inpatient qualitymeasures pertaining to SCIP Technicians List the inpatient quality reporting measurespertaining to SCIP that are time bound.What Is SCIP?19
10/4/2014Short History of SCIPSurgical Site Infection (SSI): Impact Morbidity Most common type of Healthcare Associated Infection (HAI)( 22% of all infections) An estimated 66,100 SSI’s per year are attributed to SCIPprocedures According to the CDC, an estimated 53,700 SSI’s wereassociated with 10 SCIP procedures 2%-5% of patients undergoing inpatient surgery develop a SSI Each SSI is associated with an increased LOS of approximately7-10 days20
10/4/2014SSI: Impact Mortality 3% mortality2-11 times higher risk of death compared with patients without an SSI77% of deaths among patients with SSI are directly attributable to SSIOver 8% of the HAI’s resulting in death in the US were associated withSSIs. Costs Estimated cost per infection ranges from 11,000 - 35,000Estimated total cost in the United States ranges from 3 billion - 10billion annuallyAn estimated 40-60% of these infections arepreventableSCIP Core MeasuresSCIP-Inf-1 Prophylactic Antibiotic Received within 1 Hour (2 hours if receivingVancomycin or Fluoroquinolone) Prior to Surgical IncisionSCIP-Inf-2 Appropriate Prophylactic Antibiotic Selection for SurgicalPatientsSCIP-Inf-3 Prophylactic Antibiotics Stopped within 24 Hours after SurgeryEnd Time (48 hours for cardiac patients)SCIP-Inf-4 Cardiac Surgery Patients with Controlled Postoperative BloodGlucose ( 180mg/dL) in the time- frame of 18 to 24 Hours afterAnesthesia End TimeSCIP-Inf-6 Appropriate Hair Removal (no razors)SCIP-Inf-9 Urinary catheter removed Post-Op Day 1 or 2 with day ofsurgery being Day 0SCIP-Card-2 Patients on Beta-Blocker Therapy Prior to Arrival WhoReceived a Beta-Blocker during the Perioperative PeriodSCIP-VTE-2 Appropriate Venous Thromboembolism Prophylaxis given within 24Hours Prior to Anesthesia Start Time to 24 Hours After AnesthesiaEnd TimeSCIP-Inf-10 Surgery Patients with Perioperative TemperatureManagement has been REMOVED for FY15!21
10/4/2014How does CMS Measure SCIP? The following applies to all SCIP measures: Type of Measure: Process Improvement is Noted As: An increase in rate (%) ofcompliance Goal: 100% of eligible patientsWe Can’t Afford Even One Miss!!We CAN achieve our goal of 100% compliance if we ALL worktogether to make it happen!SCIP - INFECTION MODULESCIP-Inf-1 Prophylactic Antibiotic Received within 1 Hour (2 hours ifreceiving Vancomycin or Fluoroquinolone) Prior to SurgicalIncisionSCIP-Inf-2 Appropriate Prophylactic Antibiotic Selection for SurgicalPatientsSCIP-Inf-3 Prophylactic Antibiotics Stopped within 24 Hours afterSurgery End Time (48 hours for cardiac patients)SCIP-Inf-4SCIP-Inf-6SCIP-Inf-9 Cardiac Surgery Patients with Controlled Postoperative BloodGlucose ( 180mg/dL) in the time- frame of 18 to 24 Hours afterAnesthesia End Time Appropriate Hair Removal (no razors) Urinary catheter removed on Post-Op Day 1 or 2 with day ofsurgery being Day 022
10/4/2014Prophylactic Antibiotics – QUESTIONS? Which cases benefit/are included? When should you start? Which drug should you use? How much should you give? How long should antibiotics be continued?Summary of Surgical Procedures Included in theINPATIENT SCIP Inf MeasuresSurgical ProceduresCoronary Artery Bypass Graft orOther Cardiac Surgery orVascular SurgeryHip Arthroplasty orKnee ArthroplastyColon SurgeryAbdominal HysterectomyorVaginal HysterectomyPrincipal Procedure Code of AbdominalHysterectomy with an Other ProcedureCode of Colon SurgeryorVaginal Hysterectomy with an OtherProcedure Code of Colon SurgeryApproved AntibioticsCefazolin or Vancomycin1If β-lactam allergy:Vancomycin2 or Clindamycin2Cefazolin or Vancomycin1If β-lactam allergy:Vancomycin2 or Clindamycin2Ampicillin/Sulbactam orMetronidazole Cefazolin orMetronidazole CeftriaxoneIf β-lactam allergy:Clindamycin Aminoglycoside orClindamycin Quinolone orMetronidazole Aminoglycoside orMetronidazole QuinoloneCefazolin or Cefuroxime or Ampicillin/SulbactamIf β-lactam allergy:Clindamycin Aminoglycoside orClindamycin Quinolone orMetronidazole Aminoglycoside orMetronidazole Quinolone orVancomycin Aminoglycoside orVancomycin QuinoloneCefazolin or Cefuroxime or Ampicillin/SulbactamIf β-lactam allergy:Clindamycin Aminoglycoside orClindamycin Quinolone orMetronidazole Aminoglycoside orMetronidazole Quinolone orVancomycin Aminoglycoside orVancomycin Quinolone23
10/4/2014SCIP-Inf-1 & 2 Exclusions 18 years of ageLOS 120 daysPrincipal diagnosis suggestive of preoperative infectionHad a hysterectomy AND a cesarean sectionHad other procedures requiring general or spinal anesthesia occurring within 3 days (4 days for cardiac surgery)prior to or after the procedure during a separatesurgical episode but during the same hospital stayDocumented PRE-op infectionEnrolled in a clinical trialProphylactic Antibiotics – QUESTIONS? Which cases benefit/are included? When should you start? Which drug should you use? How much should you give? How long should antibiotics be continued?24
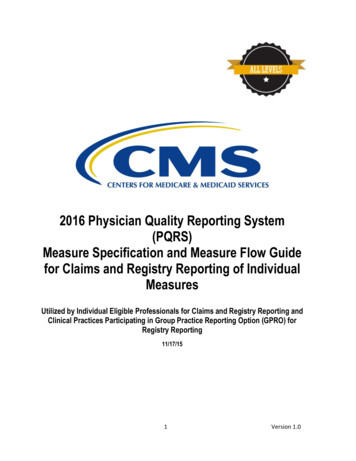
10/4/2014Prophylactic Antibiotics – TIMING415/441Infections (%)14/36931/4121/471/812/18015/6995/10090 -3-2-101234 5Hours From IncisionClassen. NEJM. 1992;328:281.Prophylactic Antibiotics – TIMINGSCIP-Inf-1 Prophylactic antibiotic must be received within onehour prior to surgical incision. This is measured by checking the earliestdocumented start time for the orderedantibiotic and comparing it to the surgicalincision date and time for the procedure. Tomeet the measure the time cannot exceed 60minutes.25
10/4/2014Prophylactic Antibiotics – TIMING There are two exception to this rule: Vancomycin and Fluoroquinolones may be started 2 hoursprior to incision due to longer infusion times. The approved prep for colon surgery includes some oralantibiotics which are taken the evening before surgery.Prophylactic Antibiotics – TIMINGAntibiotics are given for the purpose ofpreventing infection when infection is notpresent but the risk of post-operativeinfection is presentVanco – 118 min preincsion PatientArrives inPre-OpArea120minutespreincisionAncef – 63 min preincsion ABXadministered atthe SAME time asincision SurgicalIncisionTime60 min preincisionMay start administration for all other SCIPappropriate antibioticsMay start administration of Vancomycin or fluoroquinolonesIf you see an orderfor metronidazolealone, ASK the ?If you see an orderfor a quinolonealone, ASK the ?If you see an orderfor aminoglycosidealone, ASK the ?Be mindful ofdelays in surgery!26
10/4/2014Prophylactic Antibiotics – QUESTIONS? Which cases benefit/are included? When should you start? Which drug should you use? How much should you give? How long should antibiotics be continued?Summary of Antimicrobial Recommendations Based onType of Surgery for INPATIENT ProceduresSurgical ProceduresCoronary Artery Bypass Graft orOther Cardiac Surgery orVascular SurgeryHip Arthroplasty orKnee ArthroplastyColon SurgeryAbdominal HysterectomyorVagi
The VTE core measures include both prophylaxis and treatment populations 2. True or false It is possible to achieve core measures without providing optimal, evidence-based care 3. True or false VTE-5, discharge instructions, pertains to all anticoagulants 4. True or false