Transcription
Utah’sRadiology Technology Workforce:A study of radiology technology workforce trends,demand and supply, and capacity to provide servicePrepared byTomoko TamoyamaUtah Medical Education Council
AcknowledgementsUtah’s Radiology Technology Workforce: A study of radiology technology workforcetrends, demand and supply, and capacity to provide service was funded by the UtahMedical Education Council. The data in this report was made available through theprofessional efforts of various state, federal, and private organizations – see ReferencesSection.Special appreciation is given to the following individuals for their expertise andassistance:Marlene Johnson, Technology Program Administrator, University of UtahLarry Kruger, Division Chair of Radiologic Technology Program, Salt Lake CommunityCollegeRobert J. Walker, Ph.D., Weber State University Radiologic Sciences ChairpersonZane H. Williams, Weber State University Health Professions SenatorLisa Wood, Program Director, Radiologic Technology Program, Salt Lake CommunityCollegeFurther acknowledgement and appreciation is given to the staff and consulting membersof the Utah Medical Education Council: Boyd Chappell and Clint Elison.Gar Elison, Executive DirectorTomoko Tamoyama, Research Analyst2
Board Members of the Utah Medical Education CouncilChairDavid J. Bjorkman, M.D., S.M.Dean, School of MedicineUniversity of UtahVice ChairMichael J. Stapley, M.P.A.President and CEODeseret Mutual BenefitsAdministratorsLarry Reimer, M.D.Professor, PathologySchool of MedicineUniversity of UtahJohn Berneike, M.D.Director, Utah Healthcare InstituteResidency Director,St. Marks Family MedicineResidencyGaylen Bunker, M.B.A., C.P.ADirector of Business StudiesWestminster CollegeAileen ClydeEducator & Former Member ofState Board of RegentCitizen AppointeeWilliam L. Hamilton, M.D., M.B.A.Medical Director,Intermountain Health CareUrban Central RegionTeresa TheurerUtah State Board of EducationCitizen AppointeeGregg Young, M.D.Podiatry Residency DirectorVA Medical CenterDebbie SpaffordRisk ManagerAshley Valley Medical CenterCitizen AppointeeFor more information contact:Utah Medical Education Council230 South 500 East, Suite 550Salt Lake City, UT 84102-2062Phone: (801) 526-4550Fax: (801) 526-4551www.utahmec.org3
4
Table of ContentsAcknowledgements . .2Table of Contents .5Preface .6Introduction 7Section I - National workforce trends in radiology technology . 11A.B.C.D.E.F.National SupplyMajor ConstraintsFactors Contributing to the Difficulty in Recruiting Qualified FacultyResults of the Survey for Radiation Therapy environmental ScanSalary TrendsNational Experts’ RecommendationsSection II – Utah’s radiology technology environment 15A. License and CertificationB. Supply Capacity in UtahSection III - Utah’s workforce trends, supply, and demand for radiologytechnology .25A.B.C.D.E.Radiology Practical TechniciansRadiology TechnologistsUtah Salary ComparisonWorkforce DataDemand in UtahSection IV - New challenges in radiology 42A. Need for Radiology Technologists Working in an Advanced ClinicalRoleB. Roles and ResponsibilitiesC. National Training EffortsD. Certification as a Radiologists AssistantE. National DemandSection V - Conclusions and recommendations. . .47A. Conclusions5
B. Recommendations to Reduce the Shortage of Radiology TechnologyWorkforceAppendix A – National Average Annual Salary by Specialty by Year SurveyedAppendix B – Average Annual Salary by Region by Year SurveyedAppendix C – Reasons for Inactive Employment StatusAppendix D – Degrees and Programs Offered at Weber State UniversityAppendix E – Radiologic Sciences Program (Weber State University)Appendix F – Enrollment (Weber State University Dumke College of HealthProfessions)Appendix G – National Data of Radiology Practical Technician VacanciesAppendix H – Forecast of Number of Radiology Technologists of Utah in 2009Appendix I – Forecast of WSU’s Acceptant Used for Appendix HAppendix J – Number of Radiology Technologists Who May Not Renew TheirLicenses by 2009 Used for Appendix HAppendix K – Forecast of SLCC’s Acceptant Used for Appendix HPrefaceThe Utah Medical Education Council (UMEC) has been charged by statute to determineUtah’s health care workforce requirements. The UMEC is to also recommend strategiesto achieve the workforce objectives necessary to assure an adequate mix of well-trainedhealth service providers. This report covers the workforce conditions of the nonphysician radiology healthcare professionals.6
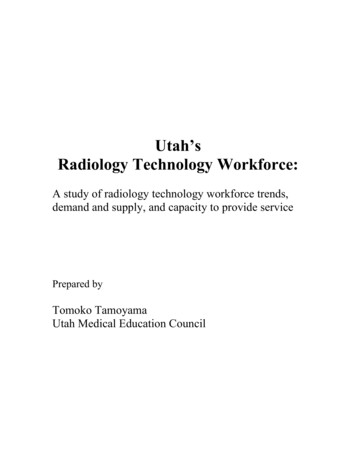
INTRODUCTIONThere are five types of professions in the radiology technology workplace: radiologypractical technicians, radiology technologists, specialized technologists, radiologistassistants, and radiology practitioner assistants.Radiology practical technicians (RPT) are limited to perform x-rays on only the chest,extremities, skull/sinuses, spine, and podiatric (see Chart 1). Formal education is notrequired.Radiology technologists (RT) are allowed to perform more services than radiologypractical technicians (see Chart 1). They hold an Associate of Applied Science degree(A.A.S.) and must pass a national certification examination administered by theAmerican Registry of Radiologic Technologists (ARRT). After passing the ARRTexamination, a registered radiology technologist (R.T.) has the privilege of using “R.T.”after his/her name. The ARRT certification is recognized in all fifty states and in mostforeign countries.Individuals who are interested in specialized areas of radiology technology can work inthose areas. The available areas are:UltrasoundNuclear MedicineMammographyBone DensitometryMagnetic Resonance ImagingCardiovascular-InterventionComputed TomographyQuality managementRadiation TherapyDosimetryBeginning in 2002 a radiologist assistant (RA) certification has been developed. Thiscame about for two reasons: 1) a need to find alternate ways of providing high qualitypatient care by extending the capacity of the physician radiologist, and 2) the need toextend the career path of radiology technology in order to support recruiting and retentionof radiology professionals. The American Registry of Radiologic Technologists (ARRT)certification as a radiologist assistant is on schedule for September 2005 introduction.Weber State University developed a singular program in 1997 that produced similarcertificates, but had some differences with the emerging RA certification. The Weberstudent is called a radiology practitioner assistant (RPA). The RPAs are a physicianextender in radiology and can provide primary patient care in radiology health careservices (see Chart 1). They must hold a current, active registration with the AmericanRegistry of Radiologic Technologists (ARRT), have completed an RPA educationalprogram recognized by the Certification Board for Radiology Practitioner Assistant7
(CBRPA), and be certified by the CBRPA. As the only program for radiologypractitioner assistants, Weber State University leads the country in seeking ways to meetthe growing demand for advanced imaging services.Licensing, Certification, and RegistrationARRT uses “certification” to describe the one-time awarding of a certificate after anindividual satisfies all eligibility requirements including the certification exam.“Registration” is the annual renewal of the certificate’s validity. A registeredtechnologist (R.T.) has satisfied standards for initial certification as well as complied withthe ARRT Standards of Ethics and Continuing Education Requirements.“Licensing” is most commonly used in referring to state laws. The State not ARRT is theauthority that administers the license and grants an individual permission to practiceradiologic technology within that state. Application for and renewal of a state license areseparate from ARRT processes.Although the ARRT examination is a voluntary certification exam, many states use thescores in licensing decisions. Approximately two-thirds of the states have licensing lawscovering the practice of radiologic technology.Thirty-five states utilize ARRT-administered exams for state licensing purposes. Thosestates ebraskaNew JerseyNew MexicoNew YorkOhioOregonPennsylvaniaRhode IslandSouth CarolinaData is from the American Registry of Radiologic shingtonWest VirginiaWyoming
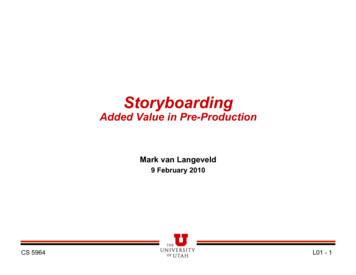
Roles of RAand RPA as aPhysicianAssistantRARPAChart 1. -- Roles of RPT and RTRPTDiagnostic odiatricIntravenous Pyelogram (IVP)Joints (Arthrography)Lower GI Tract (Barium Enema)Upper GI TractPediatric Voiding CystourethrogramArteriogramBarium X-ray (Upper and Lower GI)Computed Tomography (CT or tricFluoroscopyMagnetic Resonance Imaging (MRI)MR AngiographyMR-BodyMR-CardiacFunctional gramNew TherapiesNuclear MedicineGeneralPositron Emission Tomography (PET)PediatricCardiacIntravenous Pyelogram (IVP)Ultrafast CTUltrasoundAbdomenAbdomen scularVenous (Extremities)RTRPT Radiology Practical TechnicianRT Radiology TechnologistRA Radiologist AssistantXXXXXPrepared by the Utah Medical Education Council, March XXXXXXXXXXXXXXXX9RPA Radiology Practitioner Assistant
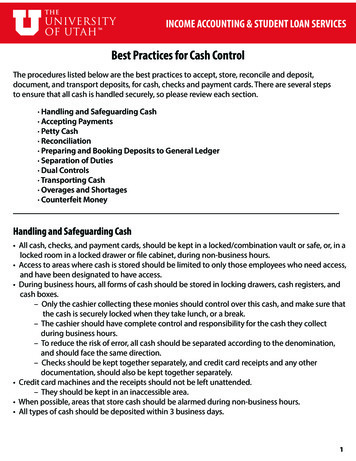
Chart 1. -- Roles of RPT and RT (cont.)RPTRTRoles of RAand RPA as aPhysicianAssistantRAInterventional RadiologyAngiographyCatheter AngiographyCT AngiographyMR AngiographyVenogramsAngioplasty and Vascular StentingEmbolizationCatheter EmbolizationUterine Fibroid EmbolizationGastrostomy TubesIntravascular UltrasoundForeign Body ExtractionNeedle BiopsyUltrasound-Guided Breast BiopsyX-ray Guided Breast BiopsyChemoembolizationCryotheraphyBlood Clot FiltersInjection of Clot-Lysing AgentsCatheters InsertionsCancer TreatmentPercutaneous VertebroplastyThrombolysisVascular Access ProceduresVertebroplastyVenous Access th PlacementsCentral Venous Line PlacementRPARPT Radiology Practical TechnicianRT Radiology TechnologistRA Radiologist AssistantXXXXXXXXXXXXXXXXXXPrepared by the Utah Medical Education Council, March 200410RPA Radiology Practitioner Assistant
I.NATIONAL WORKFORCETRENDS IN RADIOLOGYTECHNOLOGYA. National SupplyThe following are the results of a surveyof directors of educational programs:radiologic technology, nuclear medicine,and radiation therapy programs asreported by the American Society ofRadiologic Technologists (ASRT) in thefall of 2003.There is a growing concern about theshortage of trained healthcareprofessionals to provide the range ofservices required in the provision ofquality and highly technical health care.A radiology technology workforce iscritical in the provision of health caresince it provides diagnostic,interventional, and therapeutic services.Since 1999, hospitals report an 8%increase in the demand for imagingtechnicians and 68% of the hospitalsreport increased difficulty in recruitingthem (Health Forum 2001 & FirstConsulting Group 2001).The ASRT estimates the number ofadditional radiology technologists,nuclear medicine technologists, andradiation therapists that will be workingin 2010 is as follows:Radiology Technologists – 50,866, orabout two-thirds the number BLSforecasts will be required.However, 17.5% of the programdirectors indicated they plannedto increase the enrollment in theirprograms.Nuclear Medicine Technologists –12,000Radiation Therapists – 7,184This section examines the national sceneas a backdrop for comparing Utah’sworkforce requirements for the variouslevels of imaging skills required to meetthe demand for quality healthcareservices.Compared to the demand above, theanticipated supply of additional nuclearmedicine technologists and radiationtherapists will meet estimated demand.However, a shortage of at least 24,134radiology technologists is anticipated in2010.In 2000, the combined national total ofradiology technologists, nuclearmedicine technologists, and radiationtherapists was slightly less than 200,000.The Bureau of Labor Statistics (BLS)forecasted the number of additionalradiology technologists, nuclearmedicine technologists, and radiationtherapists that will be needed by 2010 asfollows:According to the ASRT report, 78.8% ofradiologic technology, 66.7% of nuclearmedicine, and 55.4% of radiationtherapy programs are at full enrollment.A total of 26,683 qualified students wereturned away from these programs in fall2003. The breakout of students deniedadmission was:Radiology Technologists – 75,000Nuclear Medicine Technologists – 8,000Radiation Therapists – 7,00011
Between 1995 and 2000, United Statesand European combined volumesincreased 19% for MRI examinations,10% for catheterization-laboratoryprocedures, 10% for CT studies, 8% forultrasound examinations, and 4% fornuclear medicine procedures.Radiography volumes did not changesignificantly during the same period,according to the American College ofRadiology In 2001, the Health CareFinancing Administration projectedtrends that it had tracked since 1980 toarrive at predictions for 2008. By then,health care costs are expected to accountfor nearly 15% of the gross domesticproduct, compared with 9% in 1980.The distribution of those health caredollars will have shifted as well. Theshare of resources spent on long-termcare will decrease slightly, from 7.1% to7%. Costs for physicians' services willincrease from 18.3% to 19.4% of healthcare spending, but spending for hospitalservices will decrease from 41.5% to31.4%. Spending for administration,construction, and other costs will risefrom 27% to 33%. Drug costs will showthe most rapid growth, from 4.9% to9.9% of spending. These figures implythat radiology departments will still beexpected to do more with less, but willthey be able to function with fewerradiologists? (Applegate and Rumack2003).Radiologic Technology Program –23,550 studentsNuclear Medicine Program – 2,375studentsRadiation Therapy Program – 758studentsData is from the fall 2003 report by the American Society ofRadiologic Technologists.Data is used with the permission by the American Society ofRadiologic Technologists.A National study “Workforce Problemsand Strategies” by Kimberly E.Applegate MD and Carol M. RumackMD determined that:The imbalance between supply anddemand is increasing. Each year, 1,000to 1,100 residents finish their training inradiology and approximately 530radiologists retire or die. The 2% annualincrease in total radiologists is exceededby the 3.5% to 5.0% annual increase indemand for radiology procedures and theannual increase in radiology relativevalue units being expended. Given therapid expansion now being seen inconsumers' use of electronic healthresources available on the Internet ,demand fueled by more widespreadknowledge of imaging may increaseeven beyond the levels currentlypredicted. As consumers become moreinformed about both noninvasivediagnostic technologies and their ownright to make health care decisions,they are more likely to request theseservices (Applegate and Rumack 2003).B. Major Constraints(ranked in order of severity)Further more the same study alsodetermined that demand is increasingWestern Europe and will likely addcompetition for those completingtraining since the supply is not growingas fast as the increase in service levels.It says that:1. Space – Classroom2. Availability of Faculty – Thosewho are academically prepared(Master or Ph.D. degrees)3. Funding4. Equipment5. Number of Clinical Sites12
79% of radiologic science programs areat full enrollment. Of the programs thathave capacity to enroll more students tomeet the projected demand as statedabove, 17.5% indicated in 2002 that theyintended to expand enrollment beginningin the fall of 2003. The data are not yetavailable to determine how muchexpansion has occurred in one year.More expansion is anticipated over thenext two or three years as state revenuesimprove. E. Salary TrendsAccording to Comparative Analysis ofthe 1997 and 2001 RadiologicTechnologist Wage and Salary Surveyby the American Society of RadiologicTechnologists (ASRT), this shortagephenomenon caused the increase ofannual salaries of all specialties ofradiology technologists (ASRT 2001).The annual salaries in 2001 ofspecialized radiology technologists wereincreased more than 11% from theannual salaries of 1997 (see AppendixA). In all regions, the annual salaries ofradiology technologists in 2001 werealso increased more than 13% from theannual salaries of 1997 (see Appendix A& B).C. Factors Contributing to theDifficulty in Recruiting QualifiedFaculty(ranked in order of importance)1. Salary2. Degree Requirements3. Availability of InterestedApplicantsData is from the fall 2003 report by the American Society ofRadiologic Technologists.Data is used with the permission by the American Society ofRadiologic Technologists.The phenomenon of higher salariescaught young people’s interest in theradiologic profession and has resulted inincreased enrollment. This has had apositive impact in Utah. For example,the number of applicants for WeberState’s two-year on-campus RadiologicSciences Program increased 3.6 timesfrom 66 students in 1997 to 240 studentsin 2003 (see Appendix C).D. Results of the Survey for RadiationTherapy Environmental ScanFour key findings result from theEnvironmental Scan of the RadiationTherapists’ Workplace survey conductedby the ASRT and the ASRT Educationand Research Foundation: training appeared to be betterprepared.Baccalaureate programsproduced more skilled graduates(ASRT 2004).Technological advances haveincreased the quality of patientcare even though the complexityof patient care has increased.Facilities are understaffedbecause of the inability to fillbudgeted positions.Therapists who had training andexperience in radiography beforebeginning their radiation therapyF. National Experts’RecommendationsThe Committee agrees with therecommendations made by nationalexperts for addressing the shortage.These recommendations are:13
e.g. workers (full time, age 25and older) with an associatedegree earn about 32,000annually, while workers witha bachelor’s degree earn about 40,000 (Sanchez 2000).Implement radiologist assistant(RA) – Advanced practice thatenhances the self-direction andownership of one’s work andresponsibilities (Racette 2001).Radiologist assistant (RA) isdistinct from the radiologypractitioner assistant (RPA), whois a graduate from a singleprogram at Weber StateUniversity in Utah (RSNA2004).University education to developthe critical-thinking skills,writing skills, case study analysisgroup-decision making anddebate for professional practice(Racette 2001).Exploration of distanceeducational programs forunderserved and rural areas(Racette 2001).Programs to recruit minoritystudents (Racette 2001).Reconsideration of usingunqualified radiology practicaltechnicians who lead only todeclines in quality patient care(Sanchez 2002).Reconsideration of training ofradiology practical technicians(limited radiography technicians)because of poor quality and lackof knowledge of radiologytechnology (Sanchez 2002).Necessity of cross-trainingradiology technologists (Sanchez2002).Increasing reimbursement ratesto make technologist salariesmore attractive (Racette 2001).Embracing the baccalaureatedegree as the minimumprofessional education standardfor the radiology technologist toreceive higher wages.The Committee agrees withthis recommendation for thosewho work outside of privateoffice settings. However, theUtah data indicate a demand fortechnicians in private physicianand chiropractic offices.Therefore, we re
Lisa Wood, Program Director, Radiologic Technology Program, Salt Lake Community College Further acknowledgement and appreciation is given to the staff and consulting members of the Utah Medical Education Council: Boyd Chappell and Clint Elison. . Radiology practical technicians