Transcription
Tuning UpYourPatientScheduleThese scheduling tips canhelp you smooth out thepeaks and valleys in yourpatient flow and increaseyour bottom line.M. Kyu Chung, MDPerhaps one of the most importantfactors in the success of a familypractice is patient flow. An officethat can successfully smooth outthe peaks and valleys in its schedule can seemore patients more efficiently, reduce wearand tear on office staff and physicians andmake more money.KEY POINTSILLUSTRATION BY SALLY WERN COMPORT The first step to improving patient scheduling inyour practice is identifying where the peaks andvalleys in your schedule occur. One way to smooth scheduling peaks is by usingthe modified-wave method. The key to modified-wave scheduling is to doublebook patients for the first slot of each hour,leaving the end of the hour open so there’s timeto catch up if the physician begins to run behindschedule.Dr. Chung is chief of theAlthough much recent attention has beenDepartment of Familygiven to open-access scheduling, there areMedicine at the Cooperother, more moderate changes you can makeHealth System in Camden,in your scheduling that can yield significantN.J., and associate professorat the Robert Wood Johnsonresults. You can begin by identifying whereMedical School in Camden.in your schedule peaks and valleys tend toConflicts of interest: noneoccur. Several causes of peaks and valleysreportedand strategies for dealing with them aredescribed in boxes that appear throughoutthis article.To address peaks and valleys in my practice’s schedule, I adopted “modified-wavescheduling,” a simpletechnique where patientsModified-wave scheduling hasare purposely doublebooked at the front endincreased my bottom line byof each hour and the endalmost 15 percent withoutof the hour is left openfor catch-up. I’ve usedincreasing my overhead.this system with muchsuccess for 19 years. Ithas increased my bottom line by almost15 percent without increasing my overhead.Here’s how it works. January 2002 www.aafp.org / fpm FAMILY PRACTICE MANAGEMENT 41Downloaded from the Family Practice Management Web site at www.aafp.org/fpm. Copyright 2002 American Academy of Family Physicians. For the private,noncommercial use of one individual user of the Web site. All other rights reserved. Contact copyrights@aafp.org for copyright questions and/or permission requests.
SPEEDBAR Making moderatechanges to your scheduling can yield significant results. The author adopted themodified-wave methodof scheduling patientappointments andincreased the capacityand efficiency of hispractice. With modified-wavescheduling, patientsare double-booked atthe front end of eachhour and the lastappointment of thehour is left open forcatch-up.Doing the wavemodified-wave technique is by comparing itI first encountered wave scheduling in theto the standard method of scheduling [Seeearly 1980s when I was doing a rotation inthe box on the next page].pediatric cardiology. Patients traveled fromthroughout the region to the clinic where IAdvantagesworked, and they were all told to come atUsing the modified-wave technique helps1 p.m. Once there, they were told they’d beprevent long patient wait times by givingseen on a “first-come, first-served” basis.physicians free time at the end of each hourThis was how originalto catch up if“wave” schedulingthey’ve begun toThe key to the modified-waveworked. Loading therun behind. In mytechnique is to load up the frontpatients at the frontexperience, patientsend of the day optirarely complainend of each hour and leave open when they have tomized the efficiency ofthe staff by guaranteewait from 15 to 25slots in the schedule later on toing there was never aminutes to see thecatch up.lull in patient flow.doctor. It’s whenWhile it was good forthe wait exceedsproductivity, it was unpopular with patients. the 25-minute mark that patients start to getSome had to wait several hours to be seen,upset and satisfaction begins to suffer. Withdespite having arrived on time for theirmodified-wave scheduling, if a physicianappointments.begins to run late, the effect isn’t cumulative:The “modified-wave” method takesThere is time built into the schedule at theadvantage of the principal behind the “wave” end of the hour to catch up.method, but it is more patient friendly. TheAnother plus of modified-wave schedulkey to the modified-wave technique is toing is that because the first appointment ofload up the front end of each hour and leave the hour is double-booked, the physician –open slots in the schedule later on to catchaware that the next patient is either alreadyup. Perhaps the best way to understand thewaiting or is in the process of being put inSEASONAL VARIATIONT Another way toimprove your scheduling is to identify yourpractice’s high and lowseasons and performroutine, comprehensivepatient visits duringyour low season.he geographic area where you practice will have a high and low season uniquely its own. One way to help smoothscheduling peaks is to encourage all patients with chronic diseases to have their comprehensive evaluations performed during your low season. How many times have you encountered a patient with complex, non-urgent problems scheduled into a 15-minute slot on a Monday during flu season? While these types of visits can’t always beavoided, they can be minimized. We’ve found that once we schedule our patients with chronic conditions to come infor routine exams during low season, they stick to that schedule. Another way to move visits of this type to the lessbusy time of year is to adjust the number of refills you prescribe so that patients’ refill requests coincide with yourless busy months.In addition to smoothing out your workload, scheduling comprehensive, non-urgent evaluations during low seasonallows you more time during the visit to discuss health maintenance issues and clean up the patient’s medication list,problem list and the overall chart. There’s also more time to ensure that your documentation and coding support thehigh level of care you provided. And, with a clear and organized chart, acute visits during the busy months can behandled much more efficiently.An unanticipated benefit of scheduling complete evaluations well in advance is that patients arrive expecting alonger visit and don’t seem to mind paying more for it. Early in my practice years, I recall several patients with whomI had spent twice the normal amount of time bitterly complaining that I had charged more than my usual rate. Itdidn’t take me long to learn that when patients make an appointment for a “regular office visit” they expect a“regular office charge.” Scheduling comprehensive visits well in advance seems to increase patients’ satisfaction thatthey’re getting what they (or their insurance plan) pay for. Also, in our practice, where the low season is summer,many patients have already met their deductibles by the time they see us for these more expensive office visits.42 FAMILY PRACTICE MANAGEMENT www.aafp.org / fpm January 2002
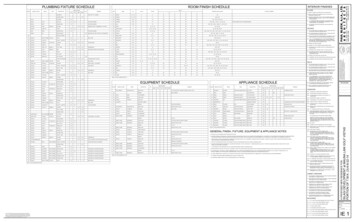
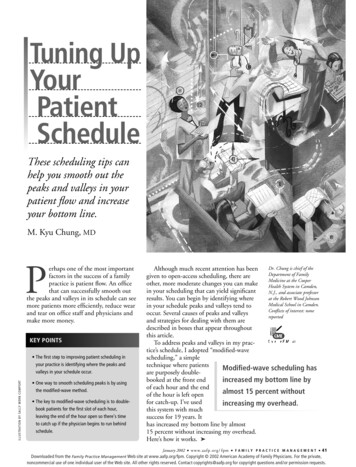
SCHEDULINGSTANDARD SCHEDULING VS. MODIFIED-WAVE SCHEDULINGEach of the following case examples is based on the mix of patient visits a family physician might encounter on an average morning.Standard scheduling methodModified-wave scheduling methodIn this scenario, patient appointments are booked in15-minute increments.Again, patients are scheduled in 15-minute increments, but two patientsare booked for the first time slot of each hour. A “catch-up” period isbuilt into the schedule at 9:45 a.m., 10:45 a.m. and 11:45 a.m. Duringthis time, no appointments are scheduled. In this scenario, more patientshad to wait, but in my experience, patients rarely complain when theyhave to wait up to 25 minutes to see the doctor.Number of patients seen: 10.Number of patients who waited: 4 (2 waited for 25 minutes and 2waited for 15 minutes).Minutes “wasted” by the doctor: 35 minutes (20 minutes waitingfor the next scheduled patients and 15 minutes for the no-show).Number of patients seen: 12.Number of patients who waited: 9 (one waited for 25 minutes and 8waited for 15 minutes or less).Minutes “wasted” by the doctor: 0.TimePatientVisit lengthAnalysisTimePatientVisit length(minutes)9:00 a.m.A78 minutes of physician/staff time wasted9:15B87 minutes :00A7No time wasted9:00B8Patient waited 7 minutes9:15C15Patient did not have to wait9:15D10Patient waited 15 minutes9:30E20Patient waited 10 minutes5 minutes wasted9:4510:45H25Analysis(minutes)15 minutes wastedNo appointment scheduled10:00Fno-show10:00G30Patient did not have towaitPatient waited 15 minutesbut took an additional 10minutes10:15H25Patient waited 15minutes10:30I15Patient waited 25 minutesand is actually seen at10:55 a.m.10:45No appointment scheduled11:00J5Patient waited 10 minutesand is actually seen at11:10 a.m.11:00K15Patient waited 15 minutes11:15L13Patient waited 15 minutes11:30M17Patient waited 13 minutesand is finished at 12:00 p.m.Visit took an additional 15minutes11:00I15Patient waited 25 minutes11:15J5Patient waited 25 minutesbut only took 5 minutes11:30K15Patient waited 15 minutesand is finished at 12:00 p.m.11:45January 2002 No appointment scheduledwww.aafp.org / fpm FAMILY PRACTICE MANAGEMENT 43
SPEEDBAR One benefit of modified-wave scheduling isthat there is time builtinto the schedule forthe physician to catchup if he or she beginsto fall behind. This keeps the doctorfrom falling furtherbehind as the day progresses and preventspatients from spendinga long time in the waiting room. Also, because the firstappointment of thehour is double-booked,the physician is awareof another patientwaiting and tends touse time more wisely.VACATIONSEvery physician has experienced being swamped several daysbefore and several days after a vacation. Reducing the number ofroutine follow-up appointments before and after a vacation can helpprevent this. The key is tapering. Several weeks before your vacation, have your receptionist block out progressively larger and largerportions of your schedule for the several days preceding your vacation. Do the reverse (i.e., block out progressively decreasing portions) for the few days following the vacation. The receptionistshould be instructed not to schedule any routine appointments during those blocked-out periods. Then, perhaps one week prior to thevacation, open up the schedule so that when patients call with semiurgent needs, they can be easily accommodated.with less complex problemswithout having to rush to getback on schedule.Finally, by stacking patients atthe beginning of an hour or session, you ensure that physicianand staff time isn’t wasted if oneof the two patients booked at thetop of the hour is a no-show.Fine-tuning the scheduleTo get even more out of modified-wave scheduling, you cangroup similar types of office visits in a single session. Some practices have surgical-procedureIn a group practice, it is often just as important to block out somedays, complete-physical days orslots on the other physicians’ schedules during the week(s) a physiall-pediatric days. For example,cian is on vacation. Frequently, it is the remaining partner(s) whoconsider setting aside one midgets the brunt of the patient overflow. These appointment slotsweek morning office session forshould be blocked out well in advance and should be reserved forphysicals. If an average physicalsame-day appointments.takes 25 to 30 minutes, twoAfter each vacation, the physician, the office manager and the perphysicals can be scheduled atson scheduling patient appointments can evaluate how well they9 a.m. and one at 9:30 a.m. Thedid in predicting the patient flow. Depending on what they decide,physician sees one of the patientsmore or fewer appointment slots can be blocked before and afterat 9 a.m. while the secondthe next vacation.patient has testing done by theancillary staff. Then, 20 minuteslater, the patients can switch, andan exam room – tends to use time morethe first patient can have testing done whilewisely. And patients who need more attenthe second patient sees the physician. Thistion do not end up getting rushed through.way, both patients with 9 a.m. appointmentsWhy? The modified-wave schedule allowshave the perception that they’ve been seenphysicians to borrow the unscheduled timeimmediately. The entire office gets into afrom the end of the hour or from patientsgroove, and you end up seeing more patients.INTRAWEEK HIGHS AND LOWS Many practices find that Mondays, and sometimes Fridays, are too busy. For example, at one of our practice sites,To avoid rushingthrough a visit involving complex problems,physicians can borrowtime from the end ofthe hour or from lesscomplex visits.the office manager and the receptionist were pulling their hair out trying to handle upset patients who couldn’t be fitinto one physician’s Monday schedule. These patients had waited since Saturday to see their own doctor on Monday,only to find they’d have to wait another day or two. Their anger was understandable. Furthermore, it took extra stafftime to cajole patients into waiting another day or two for an appointment.In this practice, the solution was simple. On Mondays, they allowed only two patients to be scheduled in advance forthe first two morning appointment slots. That way, the doctor would be assured of starting on time. The rest of theschedule was filled as the calls came in on Monday. By the time the first two scheduled morning appointments hadbeen completed, patients who had been added to the schedule that morning were already arriving at the office. Thedifference in patient and staff satisfaction was remarkable. Ill patients were told to come in almost immediately.There were also fewer phone calls to confirm patient appointments and less time spent on the phone on Mondays totriage patients away from an already full schedule.Your practice may not need to block out such a large amount of time on Mondays, but you can use the same principles to help you determine the number of slots you’ll need.44 FAMILY PRACTICE MANAGEMENT www.aafp.org / fpm January 2002
SCHEDULINGThere is one valuable strategy that cancians who are double-booked at the front endmake a huge difference in smoothing patient of the hour and then have no unscheduledflow regardless of the scheduling method you time at the end of the hour to catch up willuse: Review the schedule several days prior to fall markedly behind in no time flat.the appointment day. My medical assistantPitfall 2: Double-booking new patients,and I do this together prior to re-confirmingdifficult patients or patients with complicatappointments. That way, we can fix any odded problems at the front of the hour. Forglitches in the schedule by asking certainexample, if two new patients are scheduledpatients to come earlier or later in the day orat 9 a.m., the schedule can quickly turn intoeven on another day, if necessary.a mess. Don’t book these patients duringWhy do I assign this task to my medicalpeak time periods whenever possible, and tryassistant and not theto ensure that theirreceptionist or schedvisits are mixed withExperience has taught me thatuler? Experience hasothers that are likelytaught me that theto take less time. Ifthe scheduler is often too busyscheduler is often toothe patient asks,to put a lot of thought into howbusy to put a lot ofsimply explain thatthought into how9 a.m. is a high-trafpatients are scheduled.patients are scheduled.fic time in the officeThe medical assistantand does not giveis generally the one who is most accustomedthe doctor sufficient time to spend with theto the work style of the doctor(s) as well as to patient.the idiosyncrasies of the patients, and, consePitfall 3: Implementing modified-wavequently, is better equipped to mix and match scheduling in a large practice (20 physipatients so that each hour is balanced. A final cians) with centralized scheduling. Practicesadjustment to the schedule prior to thewith centralized scheduling can have terribleappointment day can correct the mistakesscheduling problems and have greater diffibefore they become a reality that both theculty implementing this method. The onlystaff and the patients have to deal with.way that I’ve found to make modified-wavescheduling work in a practice with centralPitfalls to avoidized scheduling is to limit a specific schedOver the years, I’ve helped many practicesuler to a specific set of doctors, conductimplement modified-wave scheduling. Ifrequent feedback sessions and commit towould be remiss not to mention havingmodifying the schedule on the fly. I generalencountered a few problems along the way.ly discourage centralized scheduling altoHere are some past mistakes I’ve seen andgether and encourage decentralizedwhat your practice can do to avoid them:scheduling at the primary care office site.Pitfall 1: Filling the catch-up time slotsThis way other issues such as billing matterswith acute visits. Avoid this at all costs. Physi- can be dealt with at the time patients schedule appointments.FPM ARTICLES ON SCHEDULINGThe bottom lineSuccessfully managing patient flow takes“Same-Day Appointments: Exploding the Accessthought and careful planning. It is by farParadigm.” Murray M, Tantau C. September 2000:one of the most challenging aspects of prac45-50. Available at: www.aafp.org/fpm/20000900/tice management. But when done correctly,45same.html.smoothing the peaks and valleys in your“Reducing Delays and Waiting Times With Openschedule using the modified-wave techniqueOffice Scheduling.” Herriott S. April 1999:38-43.will increase the capacity and efficiency ofAvailable at: www.aafp.org/fpm/990400fm/38.html.your practice without increasing your overhead. Add to that staff and physicians who“Is Your Schedule Out of Control?” Shenkel R. Separe less stressed and patients who aren’ttember 1995:66-67.enduring lengthy waits to be seen and you’ve“A Checklist for Scheduling Success.” Matthies F.got a better practice all around.SPEEDBAR To get even more out ofmodified-wave scheduling or any other scheduling technique, groupsimilar types of officevisits in a single session(e.g., “physical day”). The entire office getsinto the groove and isoften able to see morepatients. One valuable strategythat can make a difference in any schedulingtechnique is to reviewthe schedule severaldays prior to appointment day. The author does thiswith his medical assistant, who is mostaccustomed to thework style of the physician(s) and the idiosyncrasies of the patients.January 1995:68-71.Send comments to fpmedit@aafp.org.January 2002 www.aafp.org / fpm FAMILY PRACTICE MANAGEMENT 45
modified-wave method of scheduling patient appointments and increased the capacity and efficiency of his practice. With modified-wave scheduling