Transcription
ORIGINAL PAPERNagoya J. Med. Sci. 82. 315–321, 2020doi:10.18999/nagjms.82.2.315Intervention efficacy for eliminating patient misidentificationusing step-by-step problem-solving proceduresto improve patient safetyTatsuya Fukami, Masakazu Uemura, Mineko Terai, Tomomi Umemura, Mika Maeda,Mayumi Ichikawa, Naoko Sawai, Fumimasa Kitano, and Yoshimasa NagaoDepartment of Patient Safety, Nagoya University Hospital, Nagoya, JapanABSTRACTThis study aimed to evaluate the efficacy of interventions to reduce patient misidentification incidentsclassified as level 2 and over (adverse events occurred for patients) with the step-by-step problem-solvingmethod. All incidents related to patient misidentification were selected, and relevant information wascollected from the original electronic incident reports. We then conducted an eight-step problem-solvingprocess with the aim of reducing patient misclassification and improving patient safety. Step 1: the numberof misidentification-related incident reports and the percentage of these reports in the total incident reportsincreased each year. Step 2: the most frequent misidentification type was sample collection tubes, followed by drug administration and hospital meals. Step 3: we set a target of an 20% decrease in patientmisidentification cases classified as level 2 or over compared with the previous year, and established thisas a hospital priority. Step 4: we found that discrepancies in patient identification procedures were the mostimportant causes of misidentification. Step 5: we standardized the patient identification process to achieve an10% reduction in misidentification. Step 6: we disseminated instructional videos to all staff members. Step7: we confirmed there was an 18% reduction in level 2 and over patient misidentification compared withthe previous year. Step 8: we intend to make additional effort to decrease misidentification of patients bya further 10%. Level 2 and over patient misidentification can be reduced by a patient identification policyusing a step-by-step problem-solving procedure. This study aimed to evaluate the efficacy of interventionsto reduce patient misidentification incidents with step-by-step problem-solving method. Continued seamlessefforts to eliminate patient misidentification are mandatory for this activity.Keywords: patient misidentification, patient safety, problem-solving processThis is an Open Access article distributed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 InternationalLicense. To view the details of this license, please visit ).INTRODUCTIONMisidentification of patients is a fundamental patient safety issue. Facilitating the accurateidentification of patients will help minimize the risk of patient harm as a result of misidentification.1-8 Eradicating patient misidentification is also important to improve the quality of healthcare.Received: August 1, 2019; accepted: October 11, 2019Corresponding Author: Tatsuya Fukami, MD, PhDDepartment of Patient Safety, Nagoya University Hospital,65 Tsurumai-cho, Showa-ku, Nagoya 466-8560, Aichi, JapanTel: 81-52-744-2940, Fax: 81-52-744-2781, E-mail: fukami@med.nagoya-u.ac.jp315
316Tatsuya Fukami et alMajor areas where patient misidentification occurs include drug administration, blood transfusions,surgical interventions, and sample collection.9 Hand-over and other communication problemsincrease the risk of misidentification issues, particularly when multiple healthcare providers andspecialists are involved in caring for a patient.10 Patient misidentification occurs for many reasons;therefore, we applied the eight-step Toyota problem-solving method to reduce this issue in ourinstitution. This method is constantly evolving with input from multiple professionals in variousindustries11,12 and is simple and practical to apply, even for complex issues.13 The problem-solvingprocess follows eight steps (Table 1). These practical problem-solving steps include the “Plan,Do, Check and Act” cycle. The planning process incorporates Steps 1 to 5, Step 6 concernsimplementation or “doing,” and Step 7 involves checking the process. Step 8 reflects acting forthe future. This project aimed to reduce patient misidentification, especially incidents classified aslevel 2 and over (adverse events occurred for patients) according to National University HospitalCouncil of Japan recommendations. This study aimed to evaluate the efficacy of interventions toreduce patient misidentification incidents classified as level 2 and over (adverse events occurredfor patients) with step-by-step problem-solving method.MATERIALS AND METHODSOur hospital is a 1,000-bed university hospital with a clinical patient safety and qualitymanagement department that oversees patient safety affairs and is responsible for the incidentreporting system. The department comprises two doctors, three nurses, one pharmacist, onelawyer, and 10 clerical staff. When patient safety incidents and accidents occur in the hospital,they are submitted to general risk and safety managers from various occupations via an electronicreporting system; over 11,000 cases are reported each year. Patient safety incident reporting ismandatory for all staff in our hospital, including contracted workers. We surveyed the incidentreports submitted in the 2016 and 2017 fiscal years, selected all patient misidentification-relatedincidents, and collected information from the corresponding original electronic incident reports.We compared with before and after intervention to validate the effect of countermeasure. Thecollected data included the incident date; ward/department where the incident occurred; healthcareprofession, years of experience, and affiliated department of the reporter and person involvedin the incident; information regarding the patient; incident details; incident classification; andincident severity classification. Incident severity classification is widely used in Japanese hospitalsto evaluate incident severity, and is based on a classification system developed by the NationalUniversity Hospital Council of Japan (Table 2).14 The definition of patient misidentification isTable 1PlanRules of patient identification in the study hospitalStep 1Clarifying the problem and setting the themeStep 2Understanding the current situation and breaking down the problemStep 3Setting the targetStep 4Analyzing root cause factorsStep 5Developing countermeasuresDoStep 6Implementing the countermeasuresCheckStep 7Confirming the effects, and monitoring results and processActionStep 8Standardizing, stabilizing control, and sharing success
317Patient misidentification eliminationTable 2 Incident severity classification system recommendedby the National University Hospital Council of JapanLevelContinuity ofinjurySeverity ofinjuryOutcome/Treatment of injuryLevel 0––Error or trouble with a pharmaceutical or medical devicewas found, but did not affect the patientLevel 1None–There was no harm to the patient (but there was a possibility of some influence)Level 2TransientMildTreatment was not necessary (mild change in vital signs,need for increased patient observation, examination forconfirmation of safety, etc.)Level 3aTransientModerateSimple treatment was required (disinfection, poultice, skinsuture, administration of analgesics, etc.)Level 3bTransientSevereSubstantial treatment was required (significant change invital signs, use of artificial respirator, surgery, prolongationof hospitalization, hospitalization, fracture, etc.)Level 4aPermanentMild tomoderatePermanent disability or subsequent complication remained,but was not accompanied by significant dysfunction or anaesthetic problemLevel 4bPermanentModerate to Permanent disability or subsequent complication remained,severeaccompanied with significant dysfunction or an aestheticproblemLevel 5Death–Death (excluding those due to the natural course of theunderlying disease)mistaking individual patients, including misunderstanding patient information. Misunderstandinga patient’s information also includes cases where patient information is compromised, althoughthey are not mistaken directly (e.g., misprint of paper data or electronic medical record inputerror). Tools commonly used in quality monitoring include proportion charts and Pareto charts.A proportion chart is a control chart used to monitor the proportion of nonconforming units intotal sample; however, it is only suitable for a pass/fail type inspection. A value that indicatesthe highest level of quality acceptable for a product or service. The upper control limit is used inconjunction with the lower control limit to create the range of variability for quality specifications,enabling those within the organization to provide an optimal level of excellence by adhering tothe established guidelines. In a Pareto chart, the values are presented in decreasing order andthe cumulative function is a concave function. A Pareto chart was deemed appropriate for thefirst three steps in the problem-solving process (i.e., clarifying and breaking down the problemand setting to target), as a Pareto chart aims to highlight the most important causing factors.The electronic incident reporting system used by the study hospital is Incident Report Systemversion 1.0 (Safe Master Inc., Fukuoka, Japan). We extracted only necessary incident informationitems for this study, and processed information concerning individuals (e.g., the reporter and targetpatient) anonymously. All analyses were performed using SPSS version 25 (IBM, Armonk,NY, USA). This study was approved by the Institutional Review Board of the study hospital.
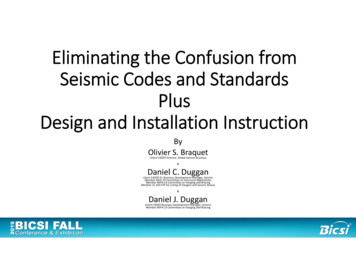
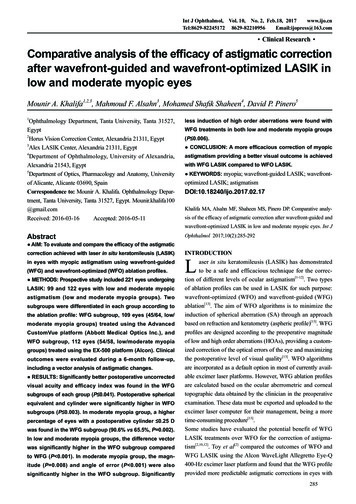
318Tatsuya Fukami et alRESULTSWe performed the Toyota step-by-step problem-solving procedure. In Step 1, we clarified thatpatient misidentification had increased. A review of the total number of patient misidentificationincidents each year from 2000 revealed that the total number of incident reports increased eachyear (Fig 1a), along with the number of misidentification-related incident reports and percentageof the total incident reports (Fig 1b). In Step 2, we assessed the proportion chart, which alsoshowed deterioration (Fig 2), and investigated cases of patient misidentification classified as level2 and over using a Pareto chart. The most frequent kind of misidentification was sample collectiontubes, followed by drug administration and hospital meals (Fig 3a). In Step 3, we decided thetarget was an 20% decrease in cases of level 2 and over patient misidentification compared withthe previous year, and set this goal as a hospital priority. In Step 4, we found that the mostimportant cause of misidentification was discrepancies in patient identification procedures. In Step5, we standardized the patient identification process to achieve the goal of 20% reduction (Table2). While we want to eliminate this type of defect, it may not be reasonable or achievable to setthis as a goal. Most would agree that starting with a 20-50% reduction per improvement periodis a reasonable goal in the beginning. For Step 6, we developed digital image demonstrationvideos of several patient identification situations (blood sampling, hospital meal delivery, bloodtransfusions) to be shown to all staff members. In Step 7, we confirmed the 18% reduction ofpatient misidentification (level 2 and over) compared with the previous year (55 cases in 2016to 45 cases in 2017) (Fig 3b). The proportion chart (Fig 2) also showed a reduction from theseactivities. Finally, in Step 8, we encouraged improved reporting attitudes and set a subsequentgoal of a further decrease 10% in patient misidentification.(a)(b)Fig. 1 The fact of incident reportsFig. 1a: The total number of incident reports in each fiscal year.Fig. 1b: The number of patient misidentification-related incident reports and percentage of total incident reports.
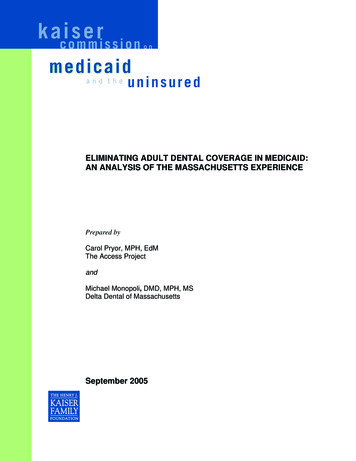
319Patient misidentification eliminationFig. 2Proportion chart of monthly report percentages relating to patient misidentification issues(number of misidentification reports/total number of inpatient-days)Open bar: level 0 or 1 incident; Closed bar: level 2 and over incidents; solid line: rate; UCL: upper controllimits; LCL: lower control limit; CL: control limit in proportion chart.Fig. 3 Pareto chart of level 2 and over patient misidentification incidentsFig. 3a: 2016 (n 55).Fig. 3b: 2017 (n 45).The data are ordered by importance.
320Tatsuya Fukami et alDISCUSSIONIn 2003, the US Joint Commission listed improving patient identification accuracy as the firstof its national patient safety goals, and this continues to be an accreditation requirement.15 Theidentification process used throughout the study hospital requires at least two ways of identifyinga patient, such as the patient’s name, identification number, birth date, or a bar-coded wristband.The process for using two different identifiers for a patient is uniform throughout the hospital.The first rule is that patients are identified using two patient identifiers, excluding the patient’sroom number and location in the hospital. The second rule is that patients are identified beforeperforming diagnostic procedures, providing treatments, and performing other procedures. Finally,rule three is that the hospital ensures the correct identification of patients in special circumstances,such as comatose patients or newborns that are not immediately named.We found that the number of misidentification-related incident reports and the percentage ofthese reports in total incident reports had been increasing each year. However, our problemsolving strategy intervention reduced level 2 and over patient misidentification incidents (whichare incidents that may possibly affect the patient) by about 18%. This countermeasures andinterventions could not help achieving the goal, but these results suggest our countermeasures acertain effect for reducing patient misidentification.The step-by-step problem-solving method is effective in the medical field, despite thecomplex issues involved. Using countermeasures developed and implemented as part of thisprocess (e.g., demonstration videos for dissemination to all staff), we partially overcame patientmisidentification, and reduced sample collection tube and hospital meal errors. These are one ofthe achievements of priority focused approach with Pareto chart. However, sample collection tubeand hospital meal errors were only two of the three major errors identified, with the third beingmisidentification-related drug administration errors. Many different roles are involved in drugadministration, including physicians (orders), pharmacists (inspection, setting, amount, specification), and nurses (delivery and administration of medication to patients). This complexity meantthat we could not develop a simple countermeasure for drug administration issues. However, weintend to focus on reducing patient misidentification in relation to drug administration errors ina follow-up project.Clinical staff must always validate that the verbal identification given by a patient matches theTable 3 Rules of patient identification in the study hospital1. Patient can state their full name (first and last names).Patient’s name information: Healthcare providers promote the patient’s selfintroduction with their full name and date of birth (or hospital identification number)with accurate details (full name, date of birth, and hospital identification number) thatcorrectly identify them and match them to their care.Healthcare provider has the patient’s name information: This must be checkedwith the available health records to ensure all details match. This information includesdisplay of electric medical records for this patient, labels on sample collection tubes,medical prescriptions, label of syringes, meal tags, documents, and others.2. Patient cannot state their name (first and last names).Patient’s name information: Healthcare providers make sure that the patient is wearinga wristband with accurate details (full name, date of birth, and hospital identificationnumber) that correctly identifies them and matches them to their care.Healthcare providers have the patient’s name information: same as for patientsthat can state their full name.
321Patient misidentification eliminationinformation on that patient’s wristband before performing any procedure, examination, treatment, oradministering any prescribed medications. Before any intervention or procedure is performed, it isthe responsibility of the staff member undertaking the intervention/procedure to check the patient’sidentity (Table 3). To support this movements, all clinical and non-clinical staff members receivean induction program from the ward or department manager to ensure they are trained in the appropriate systems. Effective interventions need useful strategies for problem-solving.16 We encouragethe application step-by-step problem-solving procedure for complicated issues in healthcare.Quality improvement is continuous, and seamless effort to eliminate misidentification ofpatients at our hospital will continue.DISCLOSURE STATEMENTNone of the authors has any conflicts of interest to declare in relation to this .16.World Health Organization. World Alliance for Patient Safety: forward programme 2005. 241592443.pdf. Published 2004. Accessed May 11, 2019.World Health Organization. WHO draft guidelines for adverse event reporting and learning systems: frominformation to action. HO-EIP-SPO-QPS-05.3-eng.pdf.Published 2005. Accessed May 11, 2019.Sandhu P, Bandyopadhyay K, Ernst DJ, et al. Effectiveness of laboratory practices to reducing patientmisidentification due to specimen labeling errors at the time of specimen collection in healthcare: systematicreview. J Appl Lab Med. 2017;2:244-258. doi: 10.1373/jalm.2017.023762.Abraham P, Augey L, Duclos A, Michel P, Piriou V. Descriptive analysis of patient misidentification fromincident report system data in a large academic hospital federation [published online ahead of print March8, 2018]. J Patient Saf. doi:10.1097/PTS.0000000000000478.Bittle MJ, Charache P, Wassilchalk DM. Registration-associated patient misidentification in an academicmedical center: causes and corrections. Jt Comm J Qual Patient Saf. 2007; 33(1):25-33.Cohen R, Ning S, Yan MTS, Callum J. Transfusion safety: the nature and outcomes of errors in patientregistration. Transfus Med Rev. 2019;33:78-83. doi: 10.1016/j.tmrv.2018.11.004.Lee NY. Reduction of pre-analytical errors in the clinical laboratory at the University Hospital of Koreathrough quality improvement activities. Clin Biochem. 2019;70:24-29. doi: 10.1016/j.clinbiochem.2019.05.016.Lippi G, Chiozza L, Mattiuzzi C, Plebani M. Patient and sample identification: out of the maze? J MedBiochem. 2017;36:107-112. doi: 10.1515/jomb-2017-0003.Bártlová S, Hajduchová H, Brabcová I, et al. Patient misidentification of nursing care. Neuro EndocrinolLett. 2015;3;17-22.World Health Organization Patient safety curriculum guide. Multi-professional ed. 789241501958 eng.pdf. Published 2011. Accessed May 11, 2019.Dogru M. The application of problem solving method on science teacher trainees on the solution of theenvironmental problems. IJESE. 2008;3:9-18.von Hippel E. “Sticky information” and the locus of problem solving: implications for innovation. MNSC.1994;40;429.Jimmerson C. A3 Problem Solving for Healthcare: A Practical Method for Eliminating Waste. 1st ed. NewYork, NY: Productivity Press; 2007.National University Hospital Council of Japan. Guidelines for the public announcement of medical accidents at national university hospitals [in Japanese]. Rev ed. http://www.univ-hosp.net/guide cat 04 15.pdf. Published June 2012. Accessed May 5, 2019.Goal1. Identify patient cor
In a Pareto chart, the values are presented in decreasing order and the cumulative function is a concave function. A Pareto chart was deemed appropriate for the . All analyses were performed using SPSS version 25 (IBM, Armonk, NY, USA). This study was approved by the Institutional Review