Transcription
ePoster #54PCCA2Efficacy and Safety of Futibatinib in IntrahepaticCholangiocarcinoma Harboring FGFR2Fusions/Rearrangements: Subgroup Analyses ofa Phase 2 Study (FOENIX-CCA2)John A. Bridgewater,1 Funda Meric-Bernstam,2 Antoine Hollebecque,3 Juan W. Valle,4,5 Chigusa Morizane,6Thomas B. Karasic,7 Thomas A. Abrams,8 Junji Furuse,9 Robin Kate Kelley,10 Philippe Cassier,11 Heinz-Josef Klümpen,12Nataliya Volodymnyrivna Uboha,13 Amit Mahipal,14 Edith Mitchell,15 Eugene R. Ahn,16 Heung-Moon Chang,17Kunihiro Masuda,18 Yaohua He,19 Karim A. Benhadji,19 Lipika Goyal201UCLCancer Institute, London, UK; 2University of Texas MD Anderson Cancer Center, Houston, TX, USA; 3Drug Development, Institut Gustave Roussy, Villejuif, France;of Manchester, Manchester, UK; 5The Christie NHS Foundation Trust, Manchester, UK; 6National Cancer Center Hospital, Tokyo, Japan; 7Hospital of the University ofPennsylvania, Philadelphia, PA, USA; 8Dana-Farber Cancer Institute, Boston, MA, USA; 9Kyorin University, Faculty of Medicine, Tokyo, Japan; 10University of California, SanFrancisco, CA, USA; 11Centre Léon-Bérard, Lyon, France; 12Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, the Netherlands; 13University ofWisconsin, Carbone Comprehensive Cancer Center, Madison, WI, USA; 14Mayo Clinic, Rochester, MN, USA; 15Sidney Kimmel Cancer Center at Jefferson, Philadelphia, PA,USA; 16Cancer Treatment Centers of America Chicago, Zion, IL, USA; 17Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea; 18Tohoku UniversityGraduate School of Medicine, Seiryo-machi, Aoba-ku, Sendai, Miyagi, Japan; 19Taiho Oncology, Inc., Princeton, NJ, USA; 20Massachusetts General Hospital, Boston,Massachusetts, USA4UniversityClinicalTrials.gov Identifier: NCT02052778
CCA2Background Patients with advanced intrahepatic cholangiocarcinoma (iCCA) have a poor prognosis, with a modest medianoverall survival (OS) of 1 year with standard first-line gemcitabine–cisplatin chemotherapy1,2 and 6.2 months withsecond-line FOLFOX (fluorouracil, leucovorin, and oxaliplatin) therapy3 FGFR fusions occur in 13–14% of patients with iCCA,4–6 and patients with FGFR aberrations may experienceimproved outcomes when treated with a fibroblast growth factor receptor (FGFR) inhibitor7– Small-molecule FGFR inhibitors are being investigated across tumor types harboring FGFR alterations8 The reversible FGFR inhibitor pemigatinib was recently approved for the treatment of advanced/metastatic CCA witha confirmed FGFR2 fusion/rearrangement9 Futibatinib is a novel, highly selective, potent, and covalently binding irreversible small-molecule inhibitor of all4 FGFR isoforms10,11 that has demonstrated tolerability and antitumor activity in a phase 1 study12,13 The robust activity of futibatinib against FGFR2 kinase-domain mutations resistant to reversible ATP-competitiveinhibitors was demonstrated in both preclinical studies14 and early clinical reports of patients previously treated withFGFR inhibitors15 FOENIX-CCA2 (NCT02052778) is a phase 2 study of futibatinib in patients with iCCA and FGFR2fusions/rearrangements who experienced treatment failure after first-line chemotherapy; this report includes datafrom the planned interim analysis of patients with 6 months of follow-upClinicalTrials.gov Identifier: NCT020527782
CCA2FOENIX-CCA2 Study Design FOENIX-CCA2 is an ongoing global open-label phase 2 study that enrolled patients with unresectable locally advanced or metastaticiCCA harboring an FGFR2 fusion or rearrangement Patients received oral futibatinib 20 mg once daily over continuous 21-day cycles until disease progression or intoleranceAE, adverse event; ECOG PS, Eastern Cooperative Oncology Group performance status; FGFR, fibroblast growth factor receptor; iCCA, intrahepatic cholangiocarcinoma; ICR, independent central radiology review;RECIST v1.1, Response Evaluation Criteria for Solid Tumors version 1.1.Database lock: March 30, 2020aAcross 36 international sites, 703 patients were prescreened and assessed for eligibility.bLocal testing was performed with next-generation sequencing, fluorescence in situ hybridization, or an alternative assay of tumor tissue/circulating tumor DNA and was centrally confirmed by Foundation One(Cambridge, MA, USA) or by a local laboratory.cTreatment was discontinued if treatment-emergent AEs did not resolve after 2 dose modifications or if the next cycle of treatment was delayed 21 days.dA planned interim analysis was performed when 70% of all treated patients had 6 months’ follow-up.ClinicalTrials.gov Identifier: NCT020527783
CCA2Patient Baseline Demographics A total of 103 patients were enrolled across 36 international sites from April 16, 2018, to November 29, 2019 In this planned interim analysis (database lock March 30, 2020), data were reported for 67 patients (65%) with 6 months’ follow-up(median follow-up was 11.4 months) Twenty-five patients (37%) remained on treatment; 36 patients (54%) discontinued because of clinical or radiological diseaseprogression, and 4 patients (6%) discontinued because of adverse events (AEs); no patients died while on treatmentECOG PS, Eastern Cooperative Oncology Group performance status; FGFR, fibroblast growth factor receptor.aRearrangements were categorized as fusions by central review only if the fusion gene partner was known or was predicted to be in-frame with FGFR.bOf 37 unique fusion partners identified, those occurring in 1 patient were BICC1 (n 15); KIAA1217 and WAC (each n 3); and SHROOM3 and SMARCC1 (each n 2).ClinicalTrials.gov Identifier: NCT020527784
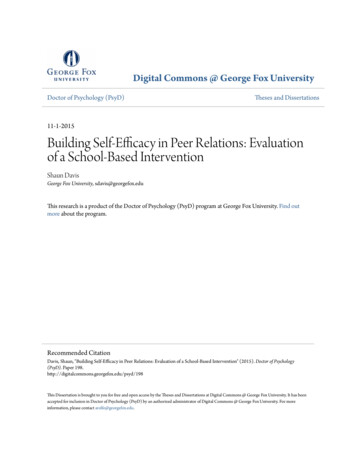
CCA2Change From Baseline in Target Lesions Objective response rate (ORR) was 37.3% Shrinkage of target lesions from baseline occurred in 28 of 30 patients who had a best response of stable diseaseCI, confidence interval; RECIST v1.1, Response Evaluation Criteria for Solid Tumors version 1.1.Dashed horizontal lines represent the 30% reduction in lesion size defined as a partial response and the 20% increase in lesion size defined as progressive disease per RECIST v1.1.aOne patient was not evaluable.ClinicalTrials.gov Identifier: NCT020527785
CCA2Duration of Futibatinib Treatment by Best Response Median duration of response was 8.3 months Duration of response was 6 months in 14 patients (21%), and 9 patients (13%) had an ongoing response of 6 months at data cutoffCI, confidence interval; NE, not evaluable.Shrinkage of target lesions from baseline occurred in 28 of 30 patients who had a best response of stable disease.Duration of response was 6 months in 14 patients (21%); 9 patients (13%) had an ongoing response of 6 months at data cutoff.ClinicalTrials.gov Identifier: NCT020527786
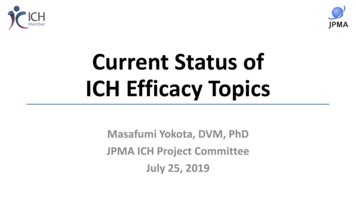
CCA2Progression-Free Survivala Median progression-free survival (PFS) was 7.2 months, and the PFS rate at 6 months was 61% (95% CI, 47.5–72.0) Median OS was not reached, and the 6-month OS rate was 86% (95% CI, 74.7–92.4)CI, confidence interval; OS, overall survival; PFS, progression-free survival.aPFS was calculated from the date of the first dose of the study drug to the date of first objective evidence of disease progression or date of death due to any cause, whichever occurs first; patients who did not havedisease progression, die, or begin a subsequent therapy without progression were censored on the date of their last tumor assessment.bOS was immature, and median OS was not reached.ClinicalTrials.gov Identifier: NCT020527787
CCA2Tumor Response in Patients With a Co-occurringGenetic Alteration of Interest Objective responses were also observed in patients with tumors harboring co-occurring genetic alterations One patient with a co-occurring TP53 mutation achieved a complete responseCR, complete response; ORR, objective response rate; PD, progressive disease; PR, partial response; SD, stable disease.Patients with more than one comutation are listed for each co-occurring alteration.aIncludes mutations in PIK3CA (n 3), PI3KC2G (n 2), PIK3C2B (n 1), and PIK3R1 (n 1).ClinicalTrials.gov Identifier: NCT020527788
CCA2Objective Response by Baseline Patient Characteristic Objective responses were observed across all patient subgroups ORRs were 33.3% in patients with a BICC1 fusion and 38.1% in patients with all other fusionsCI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group performance status; FGFR, fibroblast growth factor receptor; ORR, objective response rate.Objective response and ORR by subgroup are based on patient baseline demographics.aORRs were 33.3% in patients with a BICC1 fusion and 38.1% in patients with all other fusions.ClinicalTrials.gov Identifier: NCT020527789
CCA2Treatment-Related AEs in 15% of Patients Serious treatment-related AEs (TRAEs) were reported in 7 patients (10%); migraine was the only serious TRAE reported in 1 patient (n 2)A dosing modification occurred in 44 patients (66%) because of a TRAEOne patient discontinued because of TRAEs (stomatitis, oral dysesthesia, and pharyngeal inflammation)AE, adverse event; CTCAE, Common Terminology Criteria for Adverse Events; MedDRA, Medical Dictionary for Regulatory Activities.aNo grade 4 or 5 TRAEs were reported. bThe highest grade event was used for patients with 2 AEs in the same system organ class (or with the same preferred term) with different CTCAE grades.cHyperphosphatemia was graded according to protocol-defined serum phosphate levels.ClinicalTrials.gov Identifier: NCT0205277810
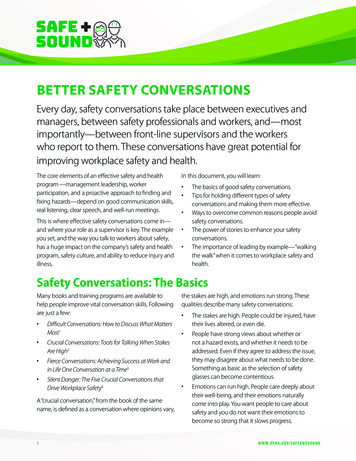
CCA2Probability of Response vs Change inSerum Phosphate From Baseline A preliminary analysis of the correlation between increased blood phosphorus and response to futibatinib showedthat patients with an objective response had a change in serum phosphate of at least 0.5 mmol/LThe maximum change in serum phosphate concentration from baseline was determined from baseline through cycle 13.ClinicalTrials.gov Identifier: NCT0205277811
CCA2AEs of Special Interest AEs of special interest are those identified based on prior studies with futibatinib and include hyperphosphatemiaand nail and eye toxicitiesAE, adverse event.aNail toxicities occurring in 1 patient were nail disorder (n 11), onycholysis (n 10), nail discoloration (n 7), paronychia (n 5), and onychalgia (n 2).bOther eye disorders reported in 1 patient were dry eye (n 16), blurred vision (n 6), increased lacrimation (n 5), trichomegaly (n 4), blepharitis (n 3), cataract (n 2), eye pain (n 2), impaired vision (n 2), andtrichiasis (n 2).cOther skin toxicities reported in 1 patient were alopecia (n 20), dry skin (n 18), pruritus (n 7), and skin fissure (n 2).ClinicalTrials.gov Identifier: NCT0205277812
CCA2Management of AEs of Special Interest Dosing modifications occurred in 28 patients (42%) because of an AE of special interest Median time to onset of any grade hyperphosphatemia was 5.0 days (range, 3.0–103.0), and grade 3hyperphosphatemia resolved in a median of 6.0 days (range, 2.0–26.0)– No patients discontinued treatment because of hyperphosphatemia Hyperphosphatemia was managed with medication in 88% of patients, including the phosphate-binding agentssevelamer (66%), acetazolamide (28%), and lanthanum carbonate (24%) Concomitant medications were used to treat eye and nail toxicities in 37 (55%) and 28 (42%) patients, respectivelyAE, adverse event.aConsists of blurred vision, chorioretinopathy, detached retinal pigment epithelium, dry eye, eye pain, foreign body sensation, increased lacrimation, and subretinal fluid.bGroup term that includes hyperphosphatemia and increased blood phosphorus.cConsists of nail discoloration, onychalgia, onycholysis, and paronychia.ClinicalTrials.gov Identifier: NCT0205277813
CCA2Conclusions An ORR of 37.3% was observed in this interim analysis of 67 patients with 6 months offollow-up– Responses were durable, lasting a median of 8.3 months, and 37% of patients remain on treatment Objective responses were observed across patient subgroups, regardless of demographic,baseline characteristic, or number of prior treatment regimens– Patients with co-occurring genetic alterations in TP53, IDH1, and PI3K-related genes had objectiveresponses The safety profile observed was consistent for this drug class, and AEs were managed wellwith dose modifications and concomitant medications– All cases of grade 3 hyperphosphatemia resolved, and no patients discontinued because of this AE These data indicate efficacy and tolerability of futibatinib in patients with iCCA harboringFGFR2 fusions/rearrangements after failure of systemic chemotherapy A phase 3 study of futibatinib versus gemcitabine–cisplatin in the first-line setting(NCT04093362) is underwayClinicalTrials.gov Identifier: NCT0205277814
CCA2References1. Okusaka T, et al. Br J Cancer 2010;103:469–74.2. Valle J, et al. N Engl J Med 2010;362:1273–81.3. Lamarca A, et al. J Natl Cancer Inst 2020;112:200–10.4. Arai Y, et al. Hepatology 2014;59:1427–34.5. Graham RP, et al. Hum Pathol 2014;45:1630–8.6. Farshidfar F, et al. Cell Rep 2017;19:2878–80.7. Jain A, et al. JCO Precis Oncol 2018;2:1–12.8. Dai S, et al. Cells 2019;8:614.9. Abou-Alfa GK, et al. Lancet Oncol 2020;21:671–84.10. Ochiiwa H, et al. Mol Cancer Ther 2013;12(suppl 11):A270.11. Kalyukina M, et al. ChemMedChem 2019;14:494–500.12. Bahleda R, et al. Ann Oncol published online July 2, 2020.doi:10.1016/j.annonc.2020.06.018.13. Meric-Bernstam F, et al. Oral presentation at: AACR Annual Meeting,March 29–April 3, 2019; Atlanta, GA; CT238.14. Sootome H, et al. Mol Cancer Ther 2013;12:A271.15. Goyal L, et al. Cancer Discov 2019;9:1064–79.Acknowledgments We thank the patients and families who made this trial possible andthe clinical study teams who were involved in this trial, as well as thedata and safety monitoring board members This study is sponsored by Taiho Oncology, Inc., and TaihoPharmaceutical Co., Ltd. Professional medical writing and editorial assistance was provided byKelly M. Fahrbach, PhD, and Jennifer Rob
cConsists of nail discoloration, onychalgia, onycholysis, and paronychia. Dosing modifications occurred in 28 patients (42%) because of an AE of special interest Median time to onset of any grade hyperphosphatemia was 5.0 days (range, 3.0–103.0), and grade 3 hyperphosphatemia resolved in a median of 6.0 days (range, 2.0–26.0)