Transcription
For your treatment-naive and relapsed/refractory SAA patients See a ProvenTrilineage ResponseWith PROMACTA1,2Patient portrayal.The first treatment for SAA approved by the FDA in nearly30 years1,3,4 —and the first and only TPO-RA approved for SAA1,5,6FDA, US Food and Drug Administration; SAA, severe aplastic anemia; TPO-RA, thrombopoietin receptor agonist.Indications and Important Safety InformationIndications for PROMACTA (eltrombopag)PROMACTA is indicated in combination with standard immunosuppressive therapy for the first-line treatment of adult and pediatricpatients 2 years and older with severe aplastic anemia.PROMACTA is indicated for the treatment of patients with severe aplastic anemia who have had an insufficient response toimmunosuppressive therapy.Limitations of UsePROMACTA is not indicated for the treatment of patients with myelodysplastic syndromes (MDS).Safety and efficacy have not been established in combination with direct-acting antiviral agents used without interferon fortreatment of chronic hepatitis C infection.Important Safety Information for PROMACTA (eltrombopag)WARNING: RISK FOR HEPATIC DECOMPENSATION IN PATIENTS WITH CHRONIC HEPATITIS CIn patients with chronic hepatitis C, PROMACTA in combination with interferon and ribavirin may increase the risk ofhepatic decompensation.RISK OF HEPATOTOXICITYPROMACTA may increase the risk of severe and potentially life-threatening hepatotoxicity. Monitor hepatic functionand discontinue dosing as recommended.Please see additional Important Safety Information for PROMACTAthroughout, and click here for full Prescribing Information, includingBoxed WARNING, and Medication Guide.
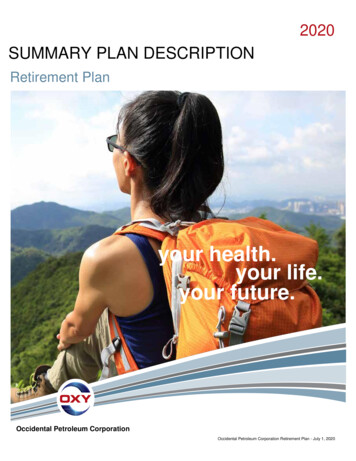
When treating SAA with PROMACTA in combination with standard IST See the proven responsein the first-line setting1,7See proven overall survivalwith PROMACTA8RESPONSE RATES AT 6 MONTHS (COHORT 3 EXTENSION COHORT)OVERALL SURVIVAL AT 2 YEARSResponse rates1Overall n 38 of 87; 95% CI, 33-55)96.7%89 of 92 patients were still alive at 24 months(n 69 of 87; 95% CI, 69-87) 2 the ratehistorically seen with standard IST alone (17%; n 102)1,7 4 of 5 patients achieved a responsewith PROMACTA1In combination with standard IST, PROMACTA is the only TPO-RAproven effective in patients with treatment-naive SAA1,5,6Median duration of response124.3monthsNo difference in median duration of responsebetween patients who achieved a complete response(n 46; 95% CI, 23.0-NE) and patients who achievedan overall response (n 70; 95% CI, 21.4-NE)Study Design Single-arm, open-label, sequential cohort trial in patients 2 years of age or older (N 153)1 All cohorts received h-ATG Days 1 to 4 and CsA for 6 to 24 months1 Cohort 3 extension cohort patients received PROMACTA (eltrombopag) Day 1 to 6 months (n 92)1‡- 66 patients were 17 years of age; 26 patients were 2 to 16 years of ageImportant Safety Information for PROMACTA (eltrombopag) (continued)HepatotoxicityPROMACTA may increase the risk of severe and potentially life-threatening hepatotoxicity.Treatment of ITP, chronic hepatitis C, and refractory severe aplastic anemia Measure serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and bilirubin prior to initiation ofPROMACTA, every 2 weeks during the dose-adjustment phase, and monthly following establishment of a stable dose2Please see additional Important Safety Information for PROMACTA throughout, and click herefor full Prescribing Information, including Boxed WARNING, and Medication Guide.ANC, absolute neutrophil count; CsA, cyclosporine A; h-ATG, horse antithymocyte globulin; Hb, hemoglobin;IST, immunosuppressive therapy (h-ATG CsA); NE, not estimable.*Complete response was defined as hematologic parameters meeting all 3 of the following values on 2 consecutiveserial blood count measurements at least 1 week apart: ANC 1000/mcL, platelet count 100,000/mcL, and Hbcount 10 g/dL.1†Overall response rate was defined as the number of partial responses (blood counts no longer meeting thestandard criteria for severe pancytopenia in SAA) plus complete responses.1‡Of these patients, 5 were not included in analyses of hematologic response at Month 6, as they had neitherreached the 6-month assessment nor withdrawn earlier.1
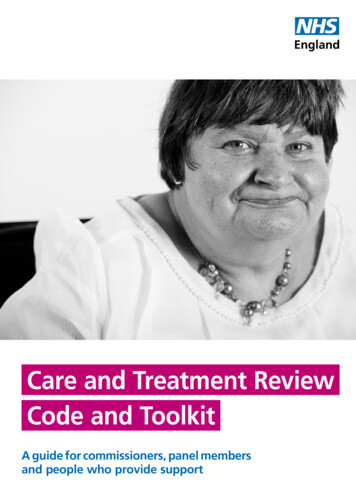
For patients with relapsed/refractory SAA A multilineage response was seenwith PROMACTA monotherapy1Safety profile in first-line andrelapsed/refractory populations1HEMATOPOIESIS MAINTAINED AFTER DISCONTINUATION1,2FIRST-LINE SAA (COHORT 3 EXTENSION COHORT)Initial Phase40%Extension Phase(n 17 of 43)achieved ahematologic response57%(n 8 of 14)achieved amultilineage responsea50%Adverse Reactions ( 5%)(n 4 of 8)achieved atrilineage responseThree of the 17 eligible patients did not enter the extension phase. 2a A multilineage response is defined as an increase in production in 2of the following hematologic markers: Platelets, white blood cells,and red blood cells2,9All 4 patients taperedand maintained atrilineage responsePROMACTA(n 92)Nausea33%AST increased17%Fatigue28%Blood bilirubin increased17%Cough23%Rash8%Diarrhea21%Skin discoloration includinghyperpigmentation5%Headache21%Pain in extremity19%Pyrexia14%Dizziness14%Oropharyngeal pain14%Abdominal pain12%Muscle spasms12%Transaminases increased12%Arthralgia12%Rhinorrhea12% Patients had bone marrow aspirates evaluated forcytogenetic abnormalities. Seven patients in Cohort 3 extension cohort had a new cytogenetic abnormalityreported, of which 4 had the loss of chromosome 7Median red blood celltransfusion-free period: 208 daysMedian platelettransfusion-free period: 200 days(6.8 months; range, 15-1082 days)(6.6 months; range, 8-1096 days)PROMACTA(N 43)29%abnormalities were 15% and 2% for AST, 26% and 4%for ALT, and 12% and 1% for bilirubin, respectivelyMEDIAN TRANSFUSION-FREE PERIOD WAS 6 MONTHSAdverse Reactions( 10%)ALT increased Grade 3 and grade 4 liver function laboratory1RELAPSED/REFRACTORYPOPULATIONPEDIATRIC VS ADULTPATIENTS (COHORT 3 EXTENSION COHORT) If new cytogenetic abnormalities are observed, considerdiscontinuation of PROMACTAAdverseReactions( 10%)Study Design Prospective, open-label, nonrandomized, single-arm, dose-modification, investigator-sponsored study conducted by the NIH to assess the safety andefficacy of PROMACTA (eltrombopag) in patients with SAA and IST-refractory thrombocytopenia (N 43)1,2,9 Primary end point was hematologic response at Week 12 or Week 16, defined by meeting 1 or more of the following criteria1,9:- Platelet count increase to 20,000/mcL above baseline or stable platelet counts with transfusion independence for a minimum of 8 weeks- Hb count increase 1.5 g/dL for patients with pretreatment Hb count 9 g/dL or a reduction in 4 units of red blood cell transfusions for8 consecutive weeks- ANC increase of 100% or 500/mcL Patients who responded in the initial phase were eligible to continue therapy in an extension phase1,2 Patients had a median age of 45 years and either had an insufficient response to at least 1 prior course of IST or were relapsed/refractory and had respondedto at least 1 prior cycle of IST but were refractory to the most recent course of IST1,9aImportant Safety Information for PROMACTA (eltrombopag) (continued)Hepatotoxicity (continued)Treatment of ITP, chronic hepatitis C, and refractory severe aplastic anemia (continued) PROMACTA inhibits UGT1A1 and OATP1B1, which may lead to indirect hyperbilirubinemia. If bilirubin is elevated, performfractionation Evaluate abnormal serum liver tests with repeat testing within 3 to 5 days. If the abnormalities are confirmed, monitor serumliver tests weekly until resolved or stabilized3Please see additional Important Safety Information for PROMACTA throughout, and click herefor full Prescribing Information, including Boxed WARNING, and Medication Guide.PROMACTAPediatric: Aged2 to 16 (n 26)PROMACTAAdult: Aged 17and Older (n 66)ALT increased23%32%AST increased12%20%Blood bilirubinincreased12%20%Rasha12%6% Patients had bone marrow aspirates evaluated forcytogenetic abnormalities Eight patients had a new cytogenetic abnormalityreported while on therapy, including 5 patients whohad complex changes in chromosome 7Rash and upper respiratory tract infection were the only serious adverse drugreactions experienced by 10% of pediatric patients.ALT, alanine aminotransferase; AST, aspartate aminotransferase; NIH, National Institutes of Health.
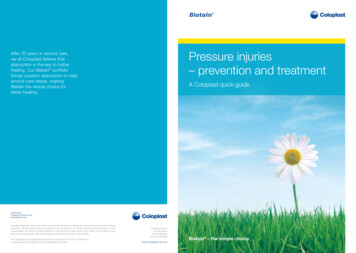
PROMACTA has been proven toeffectively restore bone marrow cellularity1,10PROMACTA is the only TPO-RAFDA approved in SAA with atrilineage response1,5,6,9,10SAA is characterized byat least 2 of the following11:PROMACTA Impaired red blood cell production Impaired white blood cell productionTPO Receptor Impaired platelet productionBoneCommittedPrecursor CellsStem CellMegakaryocyte andErythroid ProgenitorMegakaryocyte andErythroid LineageCommitted CellsPatient portrayal.Works synergistically with endogenous TPO for a trilineage response1,10Important Safety Information for PROMACTA (eltrombopag) (continued)Hepatotoxicity (continued)Treatment of ITP, chronic hepatitis C, and refractory severe aplastic anemia (continued) Discontinue PROMACTA if ALT levels increase to 3 times the upper limit of normal (ULN) in patients with normal liver functionor 3 times baseline in patients with pretreatment elevations in transaminases and are progressively increasing; or persistentfor 4 weeks; or accompanied by increased direct bilirubin; or accompanied by clinical symptoms of liver injury or evidence forhepatic decompensation If the potential benefit for reinitiating treatment with PROMACTA outweighs the risk for hepatotoxicity, then considercautiously reintroducing PROMACTA and measure serum liver tests weekly during the dose-adjustment phase. Hepatotoxicitymay reoccur if PROMACTA is reinitiated. If liver test abnormalities persist, worsen, or recur, then permanently discontinuePROMACTA4Please see additional Important Safety Information for PROMACTA throughout, and click herefor full Prescribing Information, including Boxed WARNING, and Medication Guide.PlateletsErythrocytes(Red Blood Cells)Neutrophils(White Blood Cells)TPOEPOG-CSFPROMACTAEPO, erythropoietin; G-CSF, granulocyte colony-stimulating factor; TPO, thrombopoietin.
Support for your patientswhen they need it mostNovartis is committed to supportingpatients and caregiversPatient Assistance Now Oncology Patient Assistance Now Oncology (PANO) is a support center consisting of insurance specialists and case managerswho provide access to information regarding an array of services. Consider PANO your first stop for information aboutNovartis Oncology Patient Support services. Dedicated support specialists help direct callers to the services that bestfit their needsPROMACTAUniversal Co-pay ProgramBrought to you by Novartis Oncology Patient SupportPatients may be eligible for immediate co-pay savings on their nextprescription of PROMACTA (eltrombopag).For more information, call 1-800-282-7630or visit www.PROMACTA-SAA4U.com Eligible patients with private insurance may pay 0per month Novartis will pay the remaining co-pay, up to 15,000 per calendar year,per product*Universal Co-pay CardEligible patients save onout-of-pocket costsTell your patients to visitCopay.NovartisOncology.comor call 1-877-577-7756.*Limitations apply. This offer is only available to patients with private insurance. The program is not available for patients who are enrolled in Medicare, Medicaid,or any other federal or state health care program. Novartis reserves the right to rescind, revoke, or amend this program without notice. For full Terms andConditions, visit Copay.NovartisOncology.com or call 1-877-577-7756.Encourage your patients to find out if they are eligible to enroll in the Novartis Oncology Universal Co-pay Program by visitingCopay.NovartisOncology.com or calling 1-877-577-7756.Financial assistance may be available for eligible underinsuredor uninsured patientsLow to no co-pay for Medicare patients 72% pay 10 or less—and 61% have a 0 co-pay12Patient Navigator Program The Patient Navigator Program is staffed by a dedicated team of specialists who support eligible patients during theirtreatment journey † Patients who enroll in the program receive a series of phone calls from a trained professional to help answer questionsas they begin treatment with PROMACTAHelp your patients start on Day 1!1 Ask about our sampleand voucher programPatient portrayal.5Please see additional Important Safety Information for PROMACTA throughout, and click herefor full Prescribing Information, including Boxed WARNING, and Medication Guide.The Novartis Patient Navigator Program is available for select Novartis Oncology products. Patient Navigator servicesdo not involve the practice of nursing or provide clinical advice and counseling.†
Once-daily oral dosing with PROMACTA1For treatment-naive patients1:Initiate concurrently with h-ATG CsAAdult and adolescentaged 12 and older:150 mgonce daily for 6 monthsFor patients with SAA who are of Asian ancestry(such as Chinese, Japanese, Taiwanese, Korean,or Thai) or those with mild, moderate, or severehepatic impairment (Child-Pugh Class A, B, C),PROMACTA (eltrombopag) should be initiatedat a dose of 75 mg once daily for 6 months.PediatricFor relapsed/refractory patients1:Initiate as monotherapyPROMACTA should bestarted at a dose of50 mgonce dailyFor patients with SAA who are of Asian ancestry orhave mild, moderate, or severe hepatic impairment,PROMACTA should be initiated at a reduced doseof 25 mg once daily. Adjust the dose every 2 weeks as necessary to achievetarget platelet counts1aged 6 to 11 years:75 mgonce daily for 6 monthsFor patients with SAA who are of Asian ancestryor those with mild, moderate, or severe hepaticimpairment (Child-Pugh Class A, B, C), PROMACTAshould be initiated at a dose of 37.5 mg once dailyfor 6 months.aged 2 to 5 years:2.5mg/kgFor all PROMACTA patients:PROMACTA helps your patientsmanage their dosing schedule1 PROMACTA is the only oral TPO-RA that can betaken without a meal or with a meal low in calcium( 50 mg)1,5 PROMACTA should be taken 2 hours before or4 hours after medications such as antacids andmineral supplements or foods high in calcium1once daily for 6 monthsFor patients with SAA who are of Asian ancestryor those with mild, moderate, or severe hepaticimpairment (Child-Pugh Class A, B, C), PROMACTAshould be initiated at a dose of 1.25 mg/kg oncedaily for 6 months.Important Safety Information for PROMACTA (eltrombopag) (continued)Hepatotoxicity (continued)First-line treatment of severe aplastic anemia ALT, AST, and bilirubin should be measured prior to initiation of PROMACTA During treatment, increases in ALT levels should be managed based on recommendation in Dosing and Administrationsection for hepatic impairmentThrombotic/Thromboembolic Complications Thrombotic/thromboembolic complications may result from increases in platelet counts with PROMACTA Reported thrombotic/thromboembolic complications included both venous and arterial events, and were observed at low andat normal platelet counts Portal vein thrombosis has been reported in patients with chronic liver disease receiving PROMACTA To minimize the risk for thrombotic/thromboembolic complications, do not use PROMACTA in an attempt to normalizeplatelet counts. Follow the dose-adjustment guidelines to achieve and maintain target platelet countsIncreased Risk of Death and Progression of Myelodysplastic Syndromes (MDS) to Acute Myeloid Leukemia (AML) In a clinical trial of patients with intermediate to high-risk MDS and thrombocytopenia receiving PROMACTA, an increasednumber of progressions from MDS to AML and deaths have been observed compared to placebo PROMACTA is not indicated for the treatment of patients with MDSCataracts Development or worsening of cataracts with PROMACTA has been reported with a frequency of 5% to 11% in 6 clinical studies Perform a baseline ocular examination prior to initiating PROMACTA. Regularly monitor patients for signs and symptoms ofcataracts while on PROMACTALaboratory Monitoring Monitor serum liver tests Monitor clinical hematology tests regularly throughout therapy with PROMACTA and modify the dosage regimen ofPROMACTA based on platelet counts Hematologic response may take up to 16 weeks after starting PROMACTA. If no hematologic response has occurred after16 weeks with PROMACTA, discontinue therapyDrug/Drug and Drug/Food Interactions PROMACTA must be taken at least 2 hours before or 4 hours after any medications or products containing polyvalent cationssuch as antacids, calcium-rich foods, and mineral supplements Take PROMACTA without a meal or with a meal low in calcium ( 50 mg)Adverse ReactionsAcross all indications, the most common adverse reactions ( 20% in any indication) were: anemia, nausea, pyrexia, ALTincreased, cough, fatigue, headache, and diarrhea.The most common adverse reactions ( 5%) in a single-arm trial of 92 patients 2 years and older with severe aplastic anemia(SAA) who had not received prior immunosuppressive therapy were increased ALT (29%) and AST (17%), blood bilirubinincreased (17%), rash (8%), and skin discoloration including hyperpigmentation (5%). Upper respiratory infection, particularlyin pediatric patients, was also reported. The most common adverse reactions ( 20%) in a single-arm, open-label trial in43 patients with refractory SAA who received PROMACTA were nausea (33%), fatigue (28%), cough (23%), diarrhea (21%),and headache (21%). In this trial, patients had bone marrow aspirates evaluated for cytogenetic abnormalities. Eight patientshad a new cytogenetic abnormality reported, including 5 patients who had complex changes in chromosome 7. If newcytogenetic abnormalities are observed, consider discontinuation of PROMACTA.References:1. Promacta [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2020.2. Data on file. Study ELT112523. Novartis Pharmaceuticals Corp; February 2014.3. Passweg JR, Tichelli A. Immunosuppressive treatment for aplastic anemia: are we hitting the ceiling? Haematologica. 2009;94(3):310-312.4. ClinicalTrials.gov. Bethesda, MD: US National Library of Medicine, National Institutes of Health; 2000. https://clinicaltrials.gov/ct2/results?cond severe aplastic anemia&Search Apply&recrs e&age v &gndr &type &rslt . Accessed January 3, 2020.5. Doptelet [prescribing information]. Durham, NC: Dova Pharmaceuticals Inc; 2019.6. Nplate [prescribing information]. Thousand Oaks, CA: Amgen Inc; 2019.7. Townsley DM, Scheinberg P, Winkler T, et al. Eltrombopag added to standard immunosuppression for aplastic anemia. N Engl J Med. 2017;376(16):1540-1550,S1-S39. doi:10.1056/NEJMoa1613878. A single treatment course of h-ATG should beadministered intravenously at a dose of 40 mg/kg/dayfor 4 consecutive days starting Day 11 CsA should be administered at a dose of 6 mg/kg/day(12 mg/kg/day for children under 12 years of age) fromDay 1 for at least 6 months as tolerated. In responders, CsAshould be continued at a fixed daily dose, 2 mg/kg/day,for an additional 18 months1,76Please see additional Important Safety Information for PROMACTA throughout, and click herefor full Prescribing Information, including Boxed WARNING, and Medication Guide.8. Data on file. Study ETB115AUS01T 120-day update. Novartis Pharmaceuticals Corp; July 2018.9. Desmond R, Townsley DM, Dumitriu B, et al. Eltrombopag restores trilineage hematopoiesis in refractory severe aplastic anemia that can be sustained ondiscontinuation of drug. Blood. 2014;123(12):1818-1825.10. Lum SH, Grainger JD. Eltrombopag for the treatment of aplastic anemia: current perspectives. Drug Des Devel Ther. 2016;10:2833-2843.11. Camitta BM, Thomas ED, Nathan DG, et al. Severe aplastic anemia: a prospective study of the effect of ear
Patient portrayal. PROMACTA has been proven to effectively restore bone marrow cellularity 1,10 PROMACTA is the only TPO-RA FDA approved in SAA with a trilineage response1,5,6,9,10 Works synergistically with endogenous TPO for a trilineage response 1,10 Important Safety Information for PROMACT