Transcription
New Hampshire Crisis Standards of Care PlanTable of ContentsExecutive Summary4Updates and Revisions4Crisis Standards of Care Plan5Background5Situational Awareness5Indicators and Triggers5Activation6SDMAC and State Triage Committee6Crisis Standards of Care Clinical Guidelines Scope7Guidance for Crisis Standards Development8Implementation of Crisis Standards of Care Clinical Guidelines8Appeals Process9Communication9Overview9Coordination of Hospitals and SDMAC10Public Communications11De-escalation and Recovery11CSC Activation Flowchart12Exhibit A: Clinical Concepts of Operations13Continuum of Care13In-Hospital Care14Indicators and Triggers14Core Strategies14Triage14Reactive and Proactive Triage15Triage Committee16Surge Capacity171
Transfer Guidelines20Alternative care sites21Out of Hospital Care21Outpatient Providers22Clinics22Surgical Centers23Long-term care facilities23Group homes and congregate settings24Home care24Family-based care systems25Emergency Medical Services26Palliative and Comfort Care26Palliative and Comfort Care in Hospitals and Acute Care Facilities28Palliative and Comfort Care at Out-of-Hospital Facilities28Palliative and Comfort Care at Alternate Care Sites and Systems28Just-in-Time Training for Palliative and Comfort Care28Advanced Care Planning29Psychosocial Support29Behavioral and Mental Health29Criteria for Behavioral Health Admission30Capacity of Inpatient Behavioral Health Treatment Units30Community and Outpatient Mental Health30Pediatrics31Healthcare Workforce32Quarantine32Scope of Practice32Trainees and Supervision33Other Licensing Considerations33Staff Support33Exhibit B: Ethical Framework34Overview342
Ethical Commitments34Ethical Objectives37References and Resources38AbbreviationsACS – Alternate Care SitesCMHC – Community Mental Health CenterCSC – Crisis Standards of CareDHHS – Department of Health and Human ServicesECMO—Extracorporeal Membrane OxygenationEMS – Emergency Medical ServiceEOP – Emergency Operations PlanESF 8 – Emergency Support Function 8ESU – Emergency Services UnitGSHCC – Granite State Health Care CoalitionHIC – Hospital Incident CommandHTC – Hospital Triage CommitteeICS – Incident Command SystemJIC – Joint Information CenterMACE – Multi-Agency Coordinating EntityNH—New HampshireNHICS –Nursing Home Incident Command SystemNHHA – New Hampshire Hospital AssociationOPLC – Office of Professional Licensure and CertificationPIO – Public Informations OfficerSDMAC – State Disaster Medical Advisory CommitteeSEOC – State Emergency Operations CenterSTC – State Triage Committee3
Executive SummaryThe New Hampshire Crisis Standards of Care Plan (“CSC Plan”) outlines a process forstakeholders and experts to collectively determine, communicate, and rapidly update a set ofstatewide Crisis Standards of Care clincial guidelines (“CSC clinical guidelines”) in response to aspecific crisis. CSC guidelines are activated when maintaining usual standards of care isimpossible due to a public health disaster. They aim to mitigate suffering and death throughequitable allocation of scarce healthcare resources. In addition, individual healthcareorganizations are also expected to develop their own crisis plans, a necessary extension of theirexisting Emergency Operations Plans (EOP). This CSC Plan also provides general guidance forthe creation of statewide CSC guidelines and individual healthcare organizations in preparingfor a crisis (Exhibit A: Clinical Concepts of Operations). All CSC plans and CSC clinical guidelinesare foremost grounded in the ethical principles of justice, proportionality, and solidarity, amongothers, as well as the emergency management legal authorities of the state under which theyare activated. Exhibit B addresses these ethical principles that support all crisis standards ofcare efforts.Updates and RevisionsThe NH Department of Health and Human Services (DHHS) will convene a CSC Committee torevise the CSC Plan and associated CSC guidelines, and solicit stakeholder and communityfeedback on a biennial basis and during any state-wide public health emergency exercise. Onactivation of the CSC Plan, a State Disaster Medical Advisory Committee (SDMAC), withmembers appointed by the Commissioner of the NH DHHS will update the CSC plan and CSCguidelines as outlined below.4
Crisis Standards of Care PlanBackgroundCSC clinical guidelines may represent a radical departure from usual practice and result in asignificantly increased risk of suffering and death. Under such circumstances, even smalldifferences in standards between healthcare organizations can have a magnified impact onperceptions of injustice among patients, healthcare providers, and society. Such differencesmay also represent real inequities in resources that should be promptly addressed. Unifyingcrisis standards thus necessarily entails extensive collaboration and coordination among andbetween healthcare coalitions. This paradigm of crisis management is widely accepted anddiscussed at length in the Institute of Medicine Crisis Standards of Care Framework.Situational AwarenessState CSC clinical guidelines are typically implemented in situations in which there will be aprolonged mismatch in the supply and demand for health care resources.Acute situations such as mass casualty events may provoke a short-term period of crisis care inwhich resources are temporarily limited. These situations are frequently self-limited asresources and help from surrounding regions arrive. These situations should be addressed inhospital EOPs but may not warrant a state-level response and implementation of CSC clinicalguidelines unless a prolonged mismatch (i.e. 24 hours) in supply is expected.Activation of the CSC plan itself does not necessarily constitute implementation of CSC clinicalguidelines including resource rationing and triage. Activiation of the CSC Plan allows forassembly of the SDMAC and creation of a State Triage Committee (STC).CSC clinical guidelines will only be implemented when: Resources have been, or will imminently be, overwhelmed despite exhaustive efforts toaugment and share resources with the assistance of state and federal resources.The need for implementation of resource rationing and triage has been approved by theDHHS Commissioner in consultation with appropriate authorities and stakeholders.Indicators and TriggersThe activation of the NH CSC Plan is dependent on three key factors to be considered by DHHS,details of which are dependent on the continuum of crisis care: Situational awareness indicators: Monitoring of ongoing regional, national, and globalevents for possible threats to New Hampshire.o Activation of the CSC plan, in general, will require a declaration of a State ofEmergency and/or a Public Health Incident.5
o Hospital incident command groups may request activation of the CSC Plan viathe Granite State Health Care Coalition (GSHCC) or direct request to the StateEmergency Operations Center (SEOC) or Emergency Support Function 8 (ESF 8).Indicators: Measurements, events, or other data that predict a change in demand forhealthcare requiring further analysis, or response, often determined at a state level.These can include, but are not limited to:o Disruption of facility or community infrastructure and function or request by oneor more facilities to implement the CSC plano Failure of hospital “contingency” surge capacityo Availability of material resourceso Availability of space for patient careo Pandemic phaseTriggers: Decision points based on availability of resources requiring adaptations alongthe continuum of care (contingency, conventional, and crisis). These are frequentlydependent on local situations. Triggers may include, but are not limited to:o Inability to answer all Emergency Medical Service (EMS) callso Inability to maintain appropriate staffing in healthcare centers orimplementation of atypical patient-to-provider ratioso Inability to transfer patientso Shortage of specific equipment (e.g. ventilators) or medicationsActivationThe DHHS Commissioner, in consultation with stakeholders, will initiate the CSC plan based onkey indicators, triggers, and situational factors. If local conditions necessitate activation ofhospital EOPs, they should simultaneously reach out to the SEOC and DHHS for support,regardless of state CSC plan or CSC clinical guidelines activation status.The NH DHHS will assist in coordinating activation and implementation of CSC plan and CSCclinical guidelines through its Emergency Services Unit (ESU) and ESF 8, SDMAC, and STC.SDMAC and State Triage CommitteeThe NH DHHS will convene the SDMAC to establish CSC clinical guidelines, provide guidance tohealth care facilities, and make recommendations to the Governor and SEOC during theincident. The SDMAC will consist of members appointed by the Commissioner of NH DHHS ofrepresentatives from key stakeholders such as government officials for the state of NH, as wellas legal and medical experts, risk management professionals, community representatives,ethicists, and leaders from medical societies, health care coalitions, and associations supportinghospitals, primary care, long-term care, home care, mental health, patients with disabilities,and palliative care.The SDMAC will solicit key subject matter experts to form a State Triage Commmimttee (STC), asubcommittee of the SDMAC, who will be appointed by the Commissioner of NH DHHS with6
membership relavant to the crisis at hand. Depending on the type and nature of the crisis, thesubject matter experts appointed to the STC may include physicians who are content-matterexperts in areas relevant to the crisis and practicing clinicians in the state of New Hampshire aswell as a medical ethicist, an attorney, a state medical officer, and a state emergencymanagement representative. Other considered roles for inclusion are a critical care nurse, apharmacist, a risk management representative, and 2-3 of the following: internalmedicine/pulmonary critical care physician, anesthesia critical care physician, surgical criticalcare physician, pediatric critical care physician, and emergency medicine physician as indicatedby the type of crisis.The STC will develop the CSC clinical guidelines, which will establish recommendations for thetriage of critical health care resources and provide guidance to hospital triageofficers/committees and the SDMAC. They may consult and collaborate with hospital triagecommittees, hospital ethics committees, and additional experts at their discretion. They maysolicit and use guidelines developed at stakeholder hospitals to inform state recommendations.Crisis Standards of Care Clinical Guidelines ScopeSome crisis standards can and should remain individualized as organizational-level EOPs. StateCSC clinical guidelines should address top priority issues that the SDMAC deems highlyconsequential and broadly applicable for all healthcare stakeholders, and for which alignmentof criteria between hospitals is necessary. While hospitals and other care facilities may haveEOPs and CSC that may have slight variation, any significant variation in CSC in top priorityissues will require coordination and standardization. The following areas should be consideredfor guidelines: Emergency Medical Serviceso Triage policiesAcute care facilitieso Allocation of limited, life-saving treatments, including but not limited to: Oxygen Blood Mechanical ventilation Critical care and hospital beds Hemodialysis Extracorporeal Membrane Oxygenation (ECMO) Medicationso Criteria for hospital admission, escalation of level of care, potentially lifesavingbut high-risk surgical procedures, code situationso Bed management and inter-facility transferso Healthcare personnel policies Quarantine/isolation, and return to work policies Workforce sharing7
o Visitor policiesOut of hospital careAlternative care sitesGuidelines will be prepared for any areas deemed to be of significant enough importance towarrant state guidance to promote alignment amongst healthcare facilities throughout NewHampshire.Guidance for Crisis Standards DevelopmentThe STC will utilize guidance provided in the 2009 and 2012 Institute of Medicine reports onCSC as well as up-to-date, peer-reviewed guidelines and literature relevant to the crisis at hand.Additional guidance is provided in Exhibit A of the CSC Plan. The STC will follow ethicalprinciples as outlined in Exhibit B of this document.Crisis standards of care clinical guidelines developed by the STC will: Be tailored to the crisis at hand and the availability of resources.Be grounded in the ethical principles outlined in Exhibit B. Not consider age, sex, or disability alone. Not discriminate based on religion, race, ethnicity, sexual orientation, state orcountry of origin, insurance status, or ability to pay.Be informed by applicable legal statutes, with integration of state and federalemergency orders, and waivers to expand access to medically necessary services.Primarily consider survivability and benefit from treatment in order to provide the mostbenefit for the community or population.Be transparent and accountable in their development and applicationBe widely disseminated to the public, who will be given the opportunity to providefeedbackDuring activation of the CSC Plan, any standards and guidelines created will be subject toregular updates through an iterative process based on resource availability and feedback fromHospital Incident Commands (HIC), Hospital Triage Committees (HTC), GSHCC, NHHA, and thecommunity. The creation of any state CSC clinical guidelines is expected to be a collaborativeprocess with HTCs, many of whom will already be devoting significant time and resources to thedevelopment of these plans.Implementation of Crisis Standards of Care Clinical GuidelinesThe Chest 2014 Consensus Statement on Triage recommends a multilevel triage committeesystem with a state-level triage committee supporting individual triage committees at eachhospital within the healthcare system (Christian et al. 2014). Decisions regarding triage andallocation of scarce resources, when possible, should not be made by bedside clinicians. Triagecommittees should be utilized to make proactive triage decisions and relieve bedside cliniciansof the burden of decision making when allocating resources.8
Each HIC should appoint a Triage Committee (or at minimum a Triage Officer), typically formedof 2 to 4 willing clinicians tasked with applying the CSC clinical guidelines and protocols in orderto allocate care and resources at the hospital level.1. DHHS and the SDMAC will appoint a STC formed of subject matter experts tocollaboratively develop state level CSC clinical guidelines, assure alignment of crisisstandards within the state, provide guidance to hospitals and alternate care sites ontheir implementation, and adjudicate appeals when indicated.2. HTCs should direct any concerns, recommendations, or questions regarding the CSCclinical guidelines to the STC.The standards used by all triage committees in the state should be aligned in criteria andapplication to minimize disparities in the delivery of care, while accounting for differences inthe available resources at facilities.Appeals ProcessConcurrent AppealsDuring a crisis, bedside clinicians should be provided a mechanism to appeal a triage decision inreal time to the HTC if the initial decision was based on incorrect information, there is a changein patient condition, or new clinical information is available. The HTC may consult the STC ifneeded for clarification or assistance in applying the CSC clinical guidelines.The appeals process therefore starts at the local/institutional level. If a satisfactory decisioncannot be determined at the local level, the STC should be engaged for secondary review.Retrospective AppealsDuring or after a crisis, clinicians, patients, or caregivers should be given the opportunity tosubmit retrospective appeals to help determine if triage guidelines were incorrectly appliedduring the crisis. This process would not be able to change decisions in real time or constitutebinding legal determinations or be used in any way for liability. The retroscpective appealsprocess could provide information to the caregivers and lessons could be applied in futurecrises. These appeals would first be evaluated by individual HTC and/or ethics committees butcould be sent to the STC for adjudication if indicated.Retrospective appeals made after crisis de-escalation and dissolution of crisis response teams atthe local and state level should be heard in the hospital’s ethics committee. When assistance isrequired, these requests should be directed to DHHS.CommunicationOverviewProactive communication regarding implementation of CSC clinical guidelines is critical formaintaining public trust. Clear, unified messaging promotes the ethical principles oftransparency and accountability, and relies on the alignment of CSC clinical guidelines used by9
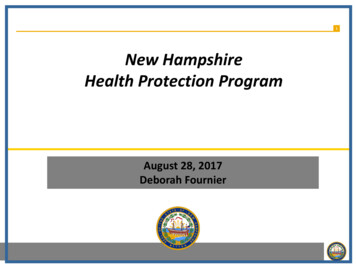
all healthcare facilities and services in the state of NH. Rapid and reliable communicationamong healthcare entities and the SDMAC will promote this alignment, which in turn willsupport strong and consistent messaging at all levels of the response.Coordination of Hospitals and SDMACDirect and indirect lines of communication from DHHS and the SDMAC (and STC) to healthcarefacilities should be established and maintained during activation of the CSC Plan for thepurposes of information sharing and communication of standards of care. Figure 1demonstrates a basic communication structure for the flow of information. Hospital incident command (HIC) groups will nominate two liaisons to the SDMACthrough which urgent communications and feedback can be given. Regional Multi-Agency Coordinating Entities (MACEs) will work with HICs to developplans for regional alternative care sites HIC groups will share summary data regarding triage decisions with the SDMAC, tothe extent deemed necessary to assure general crisis standard alignment and flagpatterns of significant wide scale deviation that may indicate a need to updateguidelines. The STC will not review individual HTC decisions unless requested underthe appeals process.The SDMAC will designate an SDMAC Liaison to facilitate communications and be theprimary point of contact for hospitals and the GSHCC for concerns pertinent to CSCplanning.CSC clinical guidelines will be disseminated to all HTCs and to the GSHCC. The GSHCC will serve as the indirect point of contact between hospitals and theSDMAC and will maintain up-to-date CSC clinical guidelines for dissemination tofacilities in the state.Guidelines or recommendations related to EMS care will be disseminated via DHHS ESUto regional MACEs via established channels.Additional lines of communication to other response organizations and healthcarefacilities (e.g. home care agencies, long-term care facilities, hospice facilities, etc.) willbe established and maintained by the ESU and ESF 8 with relevant feedback passed tothe SDMAC, and relevant recommendations from the SDMAC disseminated to thoseentities.10
Figure 1: Crisis Standards of Care Communications PathwaysPublic CommunicationsPublic communications regarding the CSC Plan and CSC clinical guidelines and their applicationwill be handled primarily by the DHHS Public Information Officer (PIO) in coordination with theSEOC, the Joint Information Center (JIC), and regional public health networks. Like implementation of the CSC clinical guidelines, communications to the publicregarding their purpose and notifications regarding their use should be proactive andtransparent.The NH DHHS will conduct regular virtual town halls to gather community feedback.Stakeholders and members of the community may submit appeals regarding thestandards to DHHS to be considered by the SDMAC during the iterative processDe-escalation and RecoveryContinuous monitoring of the situation and information sharing by the SEOC, NH DHHS/ESU
MACE – Multi-Agency Coordinating Entity . NH—New Hampshire . NHICS –Nursing Home Incident Command System . NHHA – New Hampshire Hospital Association . . insurance status, or ability to pay. Be informed by applicable legal statutes, with integration of state and federal