Transcription
Clinical OphthalmologyDovepressopen access to scientific and medical researchOriginal ResearchClinical Ophthalmology downloaded from https://www.dovepress.com/ by 137.108.70.13 on 23-Jan-2020For personal use only.Open Access Full Text ArticleComparison of simulated keratometric changesfollowing wavefront-guided and wavefrontoptimized myopic laser-assisted in situkeratomileusisThis article was published in the following Dove Press journal:Clinical OphthalmologyWen-Shin LeeEdward E MancheDepartment of Ophthalmology, ByersEye Institute, Stanford University, PaloAlto, CA, USAPurpose: The aim of the study was to determine and compare the relationship between changein simulated keratometry (K) and degree of refractive correction in wavefront-guided (WFG)and wavefront-optimized (WFO) myopic laser-assisted in situ keratomileusis (LASIK).Methods: A total of 51 patients were prospectively randomized to WFG LASIK in one eye andWFO LASIK in the contralateral eye at the Byers Eye Institute, Stanford University. Changes insimulated K and refractive error were determined at 1 year post-operatively. Linear regressionwas employed to calculate the slope of change in simulated K (ΔK) for change in refractiveerror (ΔSE). The mean ratio (ΔK/ΔSE) was also calculated.Results: The ratio of ΔK to ΔSE was larger for WFG LASIK compared to WFO LASIK whencomparing the slope (ΔK/ΔSE) as determined by linear regression (0.85 vs 0.83, p 0.04). Uponcomparing the mean ratio (ΔK/ΔSE), subgroup analysis revealed that ΔK/ΔSE was larger forWFG LASIK for refractive corrections of .3.00 D and .4.00 D (0.89 vs 0.83; p 0.0323 and0.88 vs 0.83; p 0.0466, respectively). Both linear regression and direct comparison of themean ratio (ΔK/ΔSE) for refractive corrections ,4.00 D and .4.00 D revealed no differencein ΔK/ΔSE between smaller and larger refractive corrections.Conclusion: WFO LASIK requires a smaller amount of corneal flattening compared to WFGLASIK for a given degree of refractive correction. For both, there was no significant difference in change in corneal curvature for a given degree of refractive error between smaller andlarger corrections.Keywords: LASIK, keratometry, wavefront guided, wavefront optimizedIntroductionCorrespondence: Edward E MancheByers Eye Institute, Stanford University,2452 Watson Court, Palo Alto,CA 94303, USATel 1 650 723 6995Fax 1 650 723 7918Email edward.manche@stanford.edu613submit your manuscript www.dovepress.comClinical Ophthalmology 2018:12 613–619Dovepress 2018 Lee and Manche. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.phpand incorporate the Creative Commons Attribution – Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/). By accessing the work youhereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permissionfor commercial use of this work, please see paragraphs 4.2 and 5 of our Terms i.org/10.2147/OPTH.S161387Powered by TCPDF (www.tcpdf.org)Laser photoablation is used to correct myopia by flattening the cornea proportionally tothe intended amount of refractive correction. The degree of change in corneal curvaturerelative to the amount of corrected myopia is represented by the ratio of change insimulated keratometry (K) to change in spherical equivalent (SE) of refractive error.Understanding this relationship is important for pre-operative planning, as significantflattening of the cornea may yield sub-optimal quality of vision after myopic laserphotoablation.1,2 These scenarios may be avoided by better predicting the post-operativesimulated K for a given degree of refractive correction.Additionally, understanding this relationship is relevant when consideringcataract extraction and intraocular lens (IOL) implantation in patients with a historyof prior myopic laser photoablation. A number of studies have demonstrated that
Clinical Ophthalmology downloaded from https://www.dovepress.com/ by 137.108.70.13 on 23-Jan-2020For personal use only.Lee and Manchekeratometric measurements following laser-assisted in situkeratomileusis (LASIK) are frequently overestimated.3 Thisin turn results in the selection of underpowered IOLs withconsequent hyperopic surprise. This phenomenon has beendemonstrated with various topographers, including manualkeratometry, automated keratometry, videokeratography,and IOLMaster.4–11 As a result, different methods have beenproposed to better calculate IOL power after myopic laserphotoablation.11–14A previous study has shown that the ratio of changein simulated K to change in corrected refractive error isnot linear or constant following myopic LASIK.2 Instead,for larger refractive errors, there is a smaller change insimulated K relative to degree of refractive correction.2 Thesame investigators demonstrated that custom LASIK resultsin a greater ratio of change in corneal curvature to degreeof myopic correction compared to conventional LASIK.2Whether there is a significant difference in this ratio betweenwavefront-optimized (WFO) vs wavefront-guided (WFG)LASIK has yet to be determined.Both WFO and WFG LASIK yield outstanding clinicaloutcomes and induce fewer higher order aberrations relativeto conventional LASIK.15,16 Here, the relationship betweeninduced change in corneal curvature and change in refractiveerror for both WFO and WFG LASIK was investigated, andfurthermore, any difference in this relationship when comparing the two ablation profiles was determined.MethodsA total of 102 eyes of 51 patients undergoing LASIK wereenrolled from the refractive surgery service at Byers EyeInstitute, Stanford University. Patients were followed prospectively for 1 year post-operatively. The inclusion criteriafor this study were as previously reported:15 ,12.00 D ofmyopia with ,3.00 D of astigmatism, stable refractionwith ,0.50 D change in sphere and cylinder in the prioryear, best-corrected visual acuity (BCVA) of 20/20 or betterin both eyes, cessation of soft contact lens use for 7 daysprior to the pre-operative visit, and age 21 years.The study was conducted at the Stanford Eye Laser Centerand adhered to the tenets of the Declaration of Helsinki aswell as the Health Insurance Portability and AccountabilityAct. Written informed consent was obtained from all thepatients to participate in this study. Institutional review board(IRB) approval was obtained from the Stanford UniversityIRB. The trial was publicly registered with the NationalInstitutes of Health at wered by TCPDF (www.tcpdf.org)submit your manuscript www.dovepress.comDovepressDovepressA computer-generated schedule was utilized to randomize patients to WFG LASIK (VISX CustomVue Star S4 IRexcimer laser system; Abbot Medical Optics) in one eye andWFO LASIK (WaveLight Allegretto Wave Eye-Q 400 Hzexcimer laser system; Alcon Surgical) in the contralateraleye. Allegretto used a 6.5 mm optical zone with a variableblend zone. VISX employed an optical zone of 6.0 mm with ablend zone out to 8.0 mm. Both platforms resulted in 15 µmof tissue removal per diopter of corrected myopia. The Intralase iFS 150 femtosecond laser (Abbot Medical Optics) wasused for flap creation, with flaps standardized to 9.0 mm indiameter and 105 µm in thickness.A manifest refraction was performed at the pre-operativevisit and at the post-operative year 1 visit. The differencebetween the SE at these visits was used to determine theamount of refractive change at post-operative year 1. At bothvisits, a 12 mm vertex distance was used to shift the refractionfrom the spectacle plane to the corneal plane. Scanning-slittopography (Orbscan; Bausch & Lomb) was used to determine mean corneal topography at the pre-operative visit andat the post-operative year 1 visit. The difference betweenthese measurements was used to determine the change insimulated K at post-operative year 1.A linear regression was then employed using the equation, ΔK α β [ΔSE], to assess the relationship betweenchange in simulated K (ΔK) relative to change in refractiveerror (ΔSE) for both the WFO and WFG LASIK groups.In this equation, the slope β represented the ratio of changein simulated K to change in SE (ΔK/ΔSE). The data fromthe two groups were pooled, and a joint pooled cross-sectionregression was employed using a standard F test of the equality of the coefficients to compare the slopes (β) for the WFOand WFG LASIK groups, respectively.The ratios of change in simulated K to change in SE(ΔK/ΔSE) were alternatively compared between the twoablation profiles by calculating the mean values of thisratio for each group followed by the two-variable t-test tocompare the mean values after confirming normality by theShapiro–Wilk test. All subgroups were tested for normalityusing the Shapiro–Wilk test. The Wilcoxon rank-sum testwas used to compare non-normally distributed data. Thetwo-variable t-test was used to compare normally distributed data. Subgroup analysis was performed comparing themean values of the ratio (ΔK/ΔSE) between the two ablationprofiles for changes in refractive error of .2.00 D, .3.00 D,and .4.00 D. Finally, the mean values of the ratio (ΔK/ΔSE)for changes in refractive error of ,4.00 D vs .4.00 D werecompared within each group.Clinical Ophthalmology 2018:12
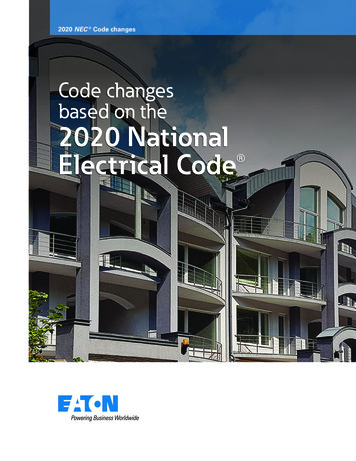
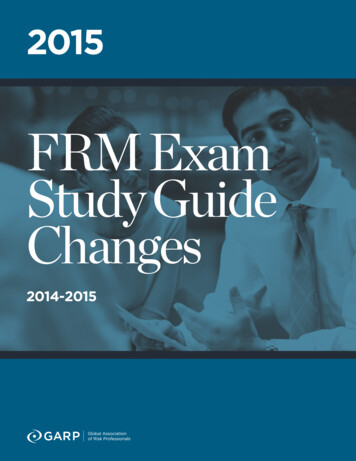
DovepressComparison of simulated keratometric changesClinical Ophthalmology downloaded from https://www.dovepress.com/ by 137.108.70.13 on 23-Jan-2020For personal use only.ResultsThere were no significant differences in pre-operative SE ofrefractive error, cylindrical error, or K values between theWFG and WFO LASIK groups (Table 1).Linear regression modeling using the equation, ΔK α β [ΔSE], demonstrated several key findings (Table 2and Figure 1). For both ablation profiles, the slope (β) waspositive (p , 0.0001), which was consistent with a positivelinear correlation between ΔK and ΔSE. The differencebetween the estimate of β between the WFG and WFOLASIK groups was statistically significant (0.85 vs 0.83,respectively, p 0.04), revealing that the degree of changein simulated K per unit of change in SE was larger in theWFG compared to the WFO LASIK cohort.The estimate of α was positive for both the WFG and WFOLASIK groups; however, this did not reach statistical significance for either group (p 0.399 and p 0.9476, respectively).Thus, the relationship between ΔK and ΔSE for both ablationprofiles did not include a positive y-intercept. Therefore, theratio (ΔK/ΔSE) in this model was constant between small andlarge changes in refractive error. That is, correcting smallerand larger refractive errors required similar correspondingflattening in corneal curvature for both ablation profiles.To more thoroughly investigate this relationship, themean values of the ratio (ΔK/ΔSE) were compared betweenchanges in refractive error ,4.00 D and .4.00 D for bothWFG and WFO LASIK (Table 3 and Figure 2). In the WFGLASIK group, there was no statistically significant difference between the ratio for refractive corrections of ,4.00 Dcompared to .4.00 D (0.91 vs 0.88, respectively, p 0.5591).In the WFO group, there was also no statistically significant difference between the ratio for refractive correctionsof ,4.00 D compared to .4.00 D (0.85 vs 0.83, respectively,p 0.6311). Thus, both linear regression modeling and directcomparison of the mean values of the ratio (ΔK/ΔSE) betweenpatients with smaller (,4.00 D) and larger (.4.00 D) refractive errors revealed that the ratio (ΔK/ΔSE) did not vary withdegree of corrected refractive error.There was no statistically significant difference whencomparing the mean ratio (ΔK/ΔSE) between the WFG andWFO LASIK groups as a whole (0.89 vs 0.84, p 0.0913)(Table 4). In subgroup analyses comparing WFG and WFOLASIK for changes in refractive error of .2.00 D, .3.00 D,and .4.00 D, all subgroups demonstrated a larger ratio(ΔK/ΔSE) for the WFG LASIK subgroups compared tothe WFO LASIK subgroups, with statistical significancereached in the .3.00 D and .4.00 D subgroups (0.89 vs0.83; p 0.0323 and 0.88 vs 0.83; p 0.0466, respectively).Thus, for larger degrees of refractive correction, WFGLASIK required more corneal flattening for a given changein refractive error when compared to WFO LASIK.DiscussionBoth WFO and WFG photoablation have become widely usedamong refractive surgeons in recent years, as these techniquesresult in a lower post-operative induction of higher orderaberrations relative to conventional therapies.16 Althoughboth WFO and WFG LASIK have been shown to result inexcellent visual outcomes, in head-to-head comparison, WFGLASIK results in less residual refractive error, improveduncorrected distance visual acuity, and improved contrastsensitivity.15 Despite the demonstrated advantages of WFGcompared to WFO LASIK, both modalities continue to bewidely used among refractive surgeons. Thus, understandingthe extent of corneal flattening induced for a given degree ofrefractive correction with both ablation profiles is importantfor both pre-operative planning and future IOL selection.The present study demonstrates that WFO LASIK requiresa smaller amount of corneal flattening for a given degree ofmyopic refractive correction compared to WFG LASIK. Thiswas demonstrated both in comparing the slope β in the linearregression model (ΔK α β [ΔSE]) and directly comparingthe mean ratio (ΔK/ΔSE) between WFG and WFO LASIK.Although comparing the mean ratio (ΔK/ΔSE) between thetwo ablation profiles for the entire cohort did not reveal astatistically significant difference, upon subgroup analysis itwas revealed that at higher degrees of refractive correction(.3.00 D and .4.00 D), WFG LASIK resulted in a largerratio of change in simulated K to change in refractive errorcompared to WFO LASIK. In other words, at higher degreesTable 1 Pre-op refractive measuresAblation profilePre-op SEPre-op cylPre-op KWFG LASIK (n 51)WFO LASIK (n 51) 4.56 1.91 ( 1.23 to 8.63) 4.61 1.66 ( 1.23 to 7.71)p 0.87290.82 0.72 (0–2.81)0.79 0.80 (0–2.90)p 0.504943.8 0.92 (42.37–46.24)43.7 0.98 (41.62–45.92)p 0.7518Notes: cyl, cylindrical error; K, simulated keratometry.Abbreviations: LASIK, laser-assisted in situ keratomileusis; pre-op, pre-operative; SE, spherical equivalent; WFG, wavefront-guided; WFO, wavefront-optimized.Clinical Ophthalmology 2018:12submit your manuscript www.dovepress.comDovepressPowered by TCPDF (www.tcpdf.org)615
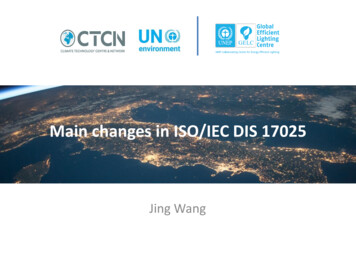
DovepressLee and MancheTable 2 Estimation results for the model (ΔK α β [ΔSE])WFG LASIKABR2Observations (n)WFO LASIKABR2Observations (n)Test of equalityF-statistica for αF-statistic for βEstimate95% .850.89510.399,0.0001 0.230.760.570.930.010.830.86510.9476,0.0001 0.420.730.450.932.544.420.080.04Notes: α, constant in the linear regression; β, slope in the linear regression; andR2, square of the correlation coefficient in the linear regression. aFor equality of thecoefficients across the two ablation profiles.Abbreviations: LASIK, laser-assisted in situ keratomileusis; WFG, wavefrontguided; WFO, wavefront-optimized.of refractive correction, WFO LASIK produced a smallerdegree of corneal flattening compared to WFG LASIK.As excessive corneal flattening may result in sub-optimalvisual outcomes,1,2 these results suggest that WFO LASIKAChange in KClinical Ophthalmology downloaded from https://www.dovepress.com/ by 137.108.70.13 on 23-Jan-2020For personal use only.Parametermay be preferable to WFG LASIK in cases when over flattening of the cornea is a concern, including patients with ahigher degree of myopia and concurrent flatter K values.With regard to post-LASIK IOL selection, corneal powercalculations are often overestimated following myopic laserphotoablation, which results in the selection of underpoweredIOLs with consequent hyperopic surprise.4–11 Our resultsindicate that at higher degrees of refractive correction, theratio (ΔK/ΔSE) is larger for WFG LASIK compared to WFOLASIK. That is, the ratio of change in corneal curvature tochange in refractive error is closer to 1:1 for WFG LASIK athigher degrees of refractive correction. As such, there maybe a smaller degree of error in post-operative corneal powercalculations for WFG LASIK compared to WFO LASIKat higher degrees of refractive correction, which may haveimplications for future IOL selection.The present study also revealed that there was no significant difference in the ratio (ΔK/ΔSE) when comparingsmaller to larger degrees of refractive error. These resultscontrast with prior work demonstrating smaller amountsof refractive correction resulting in proportionally largerchanges in corneal curvature when compared to largeramounts of refractive correction for both custom and conventional LASIK.2 This discrepancy may be related to study765VISXY 0.85X 0.17R2 0.89432112345678678Change in SEChange in KB765WlightY 0.83X 0.01R2 0.86432112345Change in SEActual99% upper limit99% lower limitFittedFigure 1 Linear regression of the change in simulated K vs the change in SE induced by WFG LASIK (A) and by WFO LASIK (B).Abbreviations: K, keratometry; LASIK, laser-assisted in situ keratomileusis; SE, spherical equivalent; WFG, wavefront-guided; WFO, wavefront-optimized; Wlight, wavelight.616Powered by TCPDF (www.tcpdf.org)submit your manuscript www.dovepress.comDovepressClinical Ophthalmology 2018:12
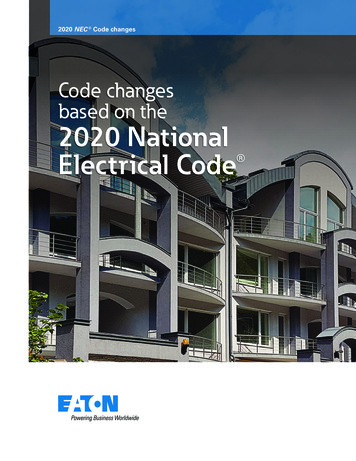
DovepressComparison of simulated keratometric changesTable 3 Comparison of the ratio of change in K to change in SE by the amount of refractive correctionParameterChange in SEa (D)RatioMeanSDMean pre-op K, D (range)Observations, np-value (ratio)p-value (pre-op K)WFO LASIK,4.00.4.00,4.00,4.000.910.2243.5 (42.4–45.9)240.55910.080.880.0944.0 (42.5–45.1)280.850.2343.6 (41.6–45.9)210.63110.33650.830.1043.8 (42.2–45.9)31Note: aInduced by LASIK.Abbreviations: LASIK, laser-assisted in situ keratomileusis; pre-op, pre-operative; SE, spherical equivalent; WFG, wavefront-guided; WFO, wavefront-optimized.methodology, as the refractive error in the previous studywas measured at the spectacle plane,2 whereas our study wasadjusted for vertex distance to calculate refractive error at thecorneal plane. In the absence of this adjustment, non-lineareffects due to change in the relative impact of vertex distancewith increased refractive error may have contributed to thedifference in the ratio (ΔK/ΔSE) between smaller and largerdegrees of refractive error demonstrated previously.2Other studies have demonstrated smaller amounts ofrefractive correction resulting in proportionally largerchanges in corneal curvature when compared to largeramounts of refractive correction in myopic photorefractive keratectomy (PRK).17,18 At that time, it was postulatedthat this phenomenon might be related to the increasedamount of stromal tissue removal required for larger corrections. That is, increased stromal tissue removal wouldbe expected to result in a greater reduction in axial lengthrelative to smaller corrections; a greater contribution tomyopic correction through reduction of axial length forlarger corrections might in turn require less corneal flattening proportionally. It is unclear why this effect was notdemonstrated in the setting of LASIK in the present study,AVISXRatio of change inK to change in SEClinical Ophthalmology downloaded from https://www.dovepress.com/ by 137.108.70.13 on 23-Jan-2020For personal use only.WFG LASIK432112345678678Change in SEBRatio of change inK to change in SEWlight432112345Change in SEActual99% upper limit99% lower limitFittedFigure 2 Ratio of change in simulated K to change in SE plotted by the amount of refractive correction for WFG LASIK (A) and WFO LASIK (B).Abbreviations: K, keratometry; LASIK, laser-assisted in
ize patients to WFG LASIK (VISX CustomVue Star S4 IR excimer laser system; Abbot Medical Optics) in one eye and WFO LASIK (WaveLight Allegretto Wave Eye-Q 400 Hz excimer laser system; Alcon Surgical) in the contralateral eye. Allegretto used a 6.5 mm optical zone with a variable b