Transcription
SupplementSeptember 2018REFRACTIVE LASER JOURNEYNavigating Laser Vision CorrectionSponsored by Carl Zeiss Meditec AG
GLOSSARYReLEx SMILE in the Context of a Patient’s Lifelong Ocular Journey 1Martin Bechmann MDState of the Art LVC Procedures: Identifying Appropriate Patients 3Paola Piccinini MDEnhancement Options After SMILE 5Walter Sekundo MD, PhDEvaluating Corneal Refractive Options for Presbyopic Patients:Efficacy and Patient Satisfaction 8Jakob Siedlecki MDFine-tuning Results for Cataract Patients After Previous Refractive Surgery Amir Hamid MDRefractive Laser Journey Navigating Laser Vision Correction10
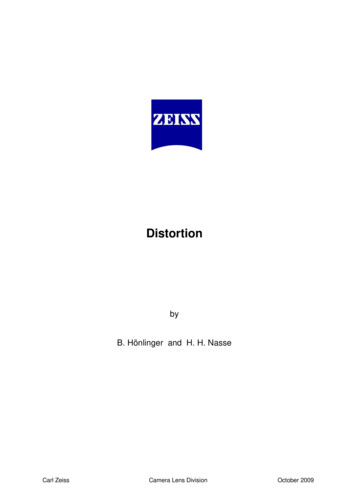
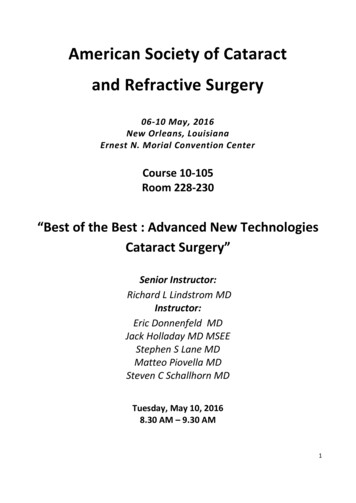
ReLEx SMILE in the Context of a Patient’s LifelongOcular JourneyMartin Bechmann MD, Medical Director, SMILE Eyes Clinics, Munich and Trier, Germany“A man who does not plan long ahead will find trouble at his door.”Confucius, Chinese philosopherAs refractive surgeons we have a duty of care toour patients to plan treatments that will standthe test of time. This means taking account ofthe patient’s ocular journey over the course of alifetime and making provision for the procedures they arelikely to require 20, 30 or even 50 years down the road,not just the 24 months that we typically follow them upafter their initial surgery. Our choice of procedure for ourrefractive patients – the majority of whom are myopes –must be suitable for them now as well as for the otherprocedures still to come over the course of their lifetime.need to be aware of the risk of ectasia in vulnerable corneas.The enhancement opportunities for LASIK are excellent – butonly in the short term, as we shall discuss later.SMILE ADVANTAGESAs a newer technique of refractive surgery, SMILE offersdistinct advantages over its predecessors: it is minimallyinvasive and does not require a flap, with therefore lessincidence of flap-related complications, there is a strongassumption that there is better retention of biomechanicalstrength2, less dry eye, better and faster recovery of cornealsensation, as well as proven predictability, efficacy and safety.Our first contact with the refractive patient is usually whenthey are in their 20s or 30s. Patients at this stage of theirlife are more adventurous, less prone to plan for the futureand their budget may be somewhat limited. For thesemyopic patients, we can offer laser vision correction in theform of photorefractive keratectomy (PRK), laser-assistedin situ keratomileusis (LASIK), small-incision lenticuleextraction (SMILE ) or if suitable a phakic IOL.At an early stage of its evolution, SMILE’s uptake wassomewhat hampered by the perception that enhancementswere not easily achieved with this technique. While it wascertainly possible to perform a PRK touch-up after SMILE,the results were not sufficiently impressive to convincemany naysayers to make the transition to SMILE. In recentyears, however, advances in laser design, software andsurgical techniques mean that this roadblock has nowbeen comprehensively cleared.In our center we currently perform 70% SMILE, 20%PRK and 10% femtosecond LASIK in LVC procedures. Thepercentage of SMILE procedures will almost certainlygrow with the introduction of a hyperopic solution in thefuture. We perform ReLEx SMILE for every patient that iseligible and will only consider femtosecond LASIK or PRK ifthere is some compelling reason to exclude SMILE, such ashyperopia, myopia minor than -1.5 dioptres1 or thin andirregular corneas.CIRCLE BREAKTHROUGHThe breakthrough came with the development of CIRCLE, asoftware used specifically with the VisuMax femtosecondlaser (Carl Zeiss Meditec AG, Germany), whereby thelaser creates several cuts that convert a SMILE cap into afemtosecond LASIK (femto-LASIK) flap. This means thatthe flap can be easily lifted using a standard flap-lifttechnique and the patient can then be enhanced usingstandard excimer laser ablation.Looking at these refractive surgery options in turn, PRK isa safe, economical and well-known technique, but it hasdownsides including postoperative discomfort and pain forthe patient and slow visual rehabilitation. The opportunityfor touch-up procedures with PRK exists but they are notperfect, and particularly so in the case of over-correction.With LASIK, we have a tried-and-trusted technique that isvery convenient and that offers rapid visual recovery, but weThe safety and efficacy of the CIRCLE technique forenhancement after SMILE was amply demonstrated in recentresults published by Jakob Siedlecki MD. Of 2,065 SMILEprocedures, 22 eyes were successfully retreated with CIRCLE,with 91% of eyes reported within 0.5D of target refractioncompared to 32% before enhancement. The percentageof eyes within 0.5D of target refraction is according tothe spherical equivalent. Safety was also excellent with alleyes gaining at least one line of uncorrected distance visualacuity (UDVA) and no eyes losing more than two lines ofvision (BSCVA). In terms of efficacy, this is close to what wewould achieve with LASIK in virgin eyes.The implications of this are quite dramatic when weconsider the long-term perspective. If the patient’s firstrefractive surgery treatment has been SMILE and aretreatment is necessary some 15 or 20 years later, we caneasily transfer the SMILE treatment into a femtosecondlaser treatment with excellent enhancement possibilities.This is important bearing in mind the ocular journeythat the patient will take over their lifetime. The realityis that we will need these touch-up opportunities in thefuture because our patients will definitely come back.CIRCLE enhancement after myopic SMILE 1Refractive Laser Journey Navigating Laser Vision Correction
They typically return to our clinics 15, 20 or 30 years aftertheir initial surgery, except now they will be asking forpresbyopic correction.If the patient underwent a PRK procedure in their 20sor 30s, we can do a touch-up without any problem butthe predictability is comparatively low and it is quiteuncomfortable. If the initial technique used was LASIK, wecan perform a flap re-lift in order to perform an additionalablation. However, we need to bear in mind that the riskof epithelial ingrowth increases dramatically over time forthese LASIK patients.4 That is why we prefer not to touchthe flap again.PRESBYOPIC OPTIONSWe can offer patients in this age group a traditionalmonovision approach, or perhaps a binocularly optimisationreceipt like PRESBYOND (Carl Zeiss Meditec AG, Germany).However, for different reasons we prefer other solutionsthan these cornea-based approaches to treat our presbyopicpatients. One possible exciting solution on the horizon forthese patients is the extended depth of focus phakic IOL,which is currently at an advanced stage of development. Ifthese lenses fulfil their promise, this could really be a gamechanger for our presbyopic patients.If the patient had undergone SMILE as the primaryrefractive procedure, we now have an elegant surgicalmethod for enhancement using the CIRCLE software.Using this approach there is no increased risk of epithelialingrowth and we perform what is essentially a primaryLASIK procedure in these eyes.A multifocal refractive lens exchange for this age group isnot a good option because of the risk of retinal detachmentin patients who have previously undergone myopic laservision correction. This has been shown very clearly in thescientific literature, and in particular a landmark Frenchstudy of 2.5 million cases where it was shown that ageis the most important risk factor for the development ofretinal detachment in myopic patients aged 40-to-55.3In my experience, refractive lens exchange with amultifocal implant is not usually a good option for thesemyopic patients. In our clinic we tend to err on the sideof caution and will rule out patients with amblyopia,primary myopia higher than 6 dioptres (because in thesehigh myopic patients the retinal function can be too muchaltered to give satisfactory results with multifocal IOLs),macular pathology and irregular corneas.CONCLUSIONPutting all of this into context, SMILE is the currentprocedure of choice in our clinic as it offers the best touchup opportunities of all the laser vision correction optionsover the long term. I believe that this really does heralda paradigm shift in refractive surgery because the CIRCLEenhancement results are so good. There is a popularGerman saying “Aller guten Dinge sind drei”, which meansthat all good things come in threes. We can expect ourpatients to keep coming back to our clinics at least threetimes for separate interventions over the course of theirlifetime. It is our responsibility and duty to be preparedfor that and to make adequate provision for their lifelongrefractive needs. SMILE helps us to achieve that.“We have become much betterthese days at attaining targetrefraction thanks to modern powercalculation formulas”CATARACT OPTIONSThe third major contact that we will have with our patientscomes when they return to us for cataract surgery. Thesepatients are usually over 55, very risk averse and liable tobe very demanding about their overall and ocular health.In this age group, refractive surgery equates to lenssurgery, with the key decision being whether to opt fora monofocal refractive lens exchange with a monovisionapproach or multifocal/EDOF IOL implantation.REFERENCES-1.5D is the clinical protocol the author used in his clinic. The CEapproved range for SMILE is: Sphere: -0.50 to -10.00D; Cylinder: 0to 5.00 D; Spherical equivalent: -0.50 to -12.50D.1Sinha Roy A et al, Comparison of biomechanical effects of smallincision lenticule extraction and laser in situ keratomileusis: finiteelement analysis. J Refract Surg. 2018 Jun 1;34(6):419-423. doi:10.3928/1081597X-20180402-05.2Lens surgery after previous laser vision correction isdemanding because of predictability issues and biometryis definitely more challenging in these cases. Nevertheless,we have become much better these days at attaining targetrefraction thanks to modern power calculation formulassuch as the Haigis-L and tools such as the ASCRS online IOLcalculator. We are definitely looking forward to using theTK formula of the IOLMaster 700 in post-LASIK cases. Themeasurement of the posterior corneal surface will help usin getting even better results. In our clinic in Munich weare currently undertaking a study in SMILE cases regardingthis topic. Despite such advances, there is still a chance thatwe will need to resort to an enhancement procedure tofine-tune the refractive outcomes. This is where the type ofrefractive laser surgery that the patient initially underwentplays a role in orienting our choices for current treatment.Refractive Laser Journey Navigating Laser Vision Correction3Daien, V. et al. Incidence, Risk Factors, and Impact of Ageon Retinal Detachment after Cataract Surgery in France.Ophthalmology 2015, Volume 122, Issue 11, 2179-2185.4Friehmann A, Mimouni M, Nemet AY, Sela T, Munzer G, KaisermanI. Risk factors for epithelial ingrowth after LASIK. J Refract Surg.2018 Feb 1;34(2):100-105.2
State of the Art LVC Procedures:Identifying Appropriate PatientsPaola Piccinini MD, Centro Oculistico Sardo, Sassari, ItalyIn just a few short years, small-incision lenticuleextraction (SMILE ) has made the transition fromniche surgical curiosity to mainstream technique, withsurgeons attracted in increasing numbers to the lure ofa minimally invasive intrastromal procedure that deliversLASIK-like results for myopia and myopic astigmatism.error. In our clinic we consider all patients in the range of-2.0D to -10D and astigmatism up to 5.0D to be potentialSMILE candidates1 unless there is an obvious reason toexclude them such as thin corneas, irregular astigmatismor topographic data indicative of potential subclinicalkeratoconus. I prefer to be conservative and always erron the side of caution when it comes to operating onthinner corneas. As we all know, the risk of post-refractivesurgery ectasia is a very real one and I see no reason atall to increase the risk even slightly by performing cornealrefractive surgery on suspect corneas when there are otheralternatives available.I was immediately attracted by the possibilities of SMILE when it was first introduced by some of my Europeancolleagues. The concept of a minimally invasive procedurethat delivered consistently excellent refractive outcomesand that respected the biomechanical integrity of thecornea was something that was very appealing to me as arefractive surgeon. By focusing the treatment exclusivelyon the stroma, SMILE preserves Bowman’s layer, which isinherently good for biomechanical stability, and, when itis possible to perform the treatment under 130 microns,preserves the superficial nerve plexus.I would estimate that about 40% of our patients undergoSMILE procedures, and that percentage is increasingall the time due to patient demand and expandedindications on the back of multiple robust clinical studies.Like other refractive surgery clinics, we eagerly anticipatebeing able to offer a hyperopic SMILE solution in the nearfuture, and this will undoubtedly generate even moredemand for our services.I liked the fact that SMILE offered a tissue-sparingprocedure focused on the stroma, but without all ofthe inconveniences of PRK such as postoperative pain,discomfort and delayed visual rehabilitation. Up until2010, the vast majority of my refractive surgery cases hadbeen PRK. Around that time, our clinic decided to investin the VisuMax femtosecond laser (Carl Zeiss Meditec AG,Germany) and we soon started performing femtosecondLASIK with very good results.“The concept of a minimally invasiveprocedure that delivered consistentlyexcellent refractive outcomes and thatrespected the biomechanical integrityof the cornea was very appealing”However, once ReLEx SMILE (Carl Zeiss Meditec AG,Germany) became commercially available and started tomake an impact, we knew that this was the direction thatwe wanted to take our practice. SMILE seemed to offerall of the advantages of LASIK, but without the downsideof a flap and the flap-related complications. We werealready familiar with the VisuMax laser, so that definitelyshortened the learning curve for us. Nevertheless, it wasstill an exciting moment for us when we performed ourfirst myopic SMILE procedures in April 2014.CHAIR TIME KEY TO SUCCESSWhen the patient first comes into our clinic we always taketime to explain to them all of the corneal refractive optionsthat are available to them. It is important that they fullyunderstand the differences between the various optionssuch as LASIK, PRK and SMILE, and why we believe thata particular procedure will be the appropriate choice forthem. Chair time is vital in managing patient expectationsand we spend a lot of time discussing patients’ wishes andtheir particular ocular needs in terms of their individualcareer, lifestyle or hobbies. After all, these patients aretypically in the 20-to-40 years of age bracket and theseare the most active years of their lives, so we need to besure that we are offering them the best surgical solutiontailored to their own particular situation. There is no “onesize-fits-all” solution for these young refractive patients.IMPRESSIVE RESULTSFrom the outset, we were impressed by the results interms of the quantity and quality of vision that ourpatients achieved. While it has often been said that SMILEis technically difficult, this was not really our experience.Although our familiarity with the VisuMax platform clearlyhelped in this respect, we found that once the basic stepsof the procedure had been mastered, the surgery itself wasnot overly complex and usually proceeded in a smooth andcontrolled manner. Based on the excellent initial resultsand the positive feedback of patients, we soon began tooffer SMILE as the first-choice procedure to our patientswith myopia and myopic astigmatism who expressed aninterest in corneal refractive surgery.When it comes to discussing SMILE, I explain to the patientthat this is a minimally invasive procedure, which does notrequire a flap, and that they can usually return to normalactivities within a day or two of their procedure. This isa very attractive proposition for this younger age groupwho lead an active lifestyle and who do not want to beincapacitated for several days after surgery or who canPatient selection remains a critical component in achievingpostoperative success in refractive surgery, and SMILE is noexception. Many of the requirements for SMILE surgeryreflect the standard parameters for other laser refractivetechniques, including ocular health, age and refractive3Refractive Laser Journey Navigating Laser Vision Correction
afford to wait a long time on full visual rehabilitation.SMILE frequently appeals to them because it offers thepossibility of a rapid return to their normal activities orhobbies, even if those pastimes happen to be boxing orwater sports. Patients are also apprehensive about theprospect of postoperative pain or discomfort with surfaceablation procedures, so they are usually very relievedwhen they hear that SMILE offers them a virtually painfree recovery period.under-corrected for distance vision did not feel that itwas sufficiently bothersome to warrant further surgeryand they were quite happy overall with the quality oftheir vision.CONCLUSIONI experienced a lot of initial scepticism from my colleaguesin Italy when I first started performing SMILE, but theyare a lot more interested and less sceptical today. Whatis patently clear to me and most of my colleagues is thatSMILE is here to stay. LASIK is a wonderful procedure andwill be around for a long time to come, but there is aclear trend towards minimally invasive procedures and themomentum is with SMILE.One of the aspects that has particularly impressed mewith this technique is the positive feedback that we getfrom patients after their SMILE procedures, either directlyto us or posted on our clinic’s social media pages. Happypatients are the best form of advertisement for anyrefractive surgery procedure and it is gratifying to seehow enthusiastic our patients are in recommending SMILEto other family members and friends. Patients are verypleased with the quality of vision and the fact that thepostoperative recovery is so comfortable and that they canreturn to work usually within one day of their procedure.We are seeing a lot more results published showing thatthe safety and efficacy is equal to or better than LASIK andSMILE clearly has the edge in terms of preserving nervefibres. Taking all this into consideration, I truly believethat SMILE gives us even more treatment options andrepresents the future of corneal refractive surgery.Overall, I am very satisfied with the quality of my clinicalresults with myopic SMILE, which are broadly in line withthose reported in the scientific literature. I did makesome adjustments to my nomogram after my initial seriesof patients experienced slight under-correction, and therefractive outcomes are much tighter now. Perhaps it isdown to judicious patient selection, but for the momentI have not had to perform even one enhancement afterSMILE. Even those early patients who were slightlyRefractive Laser Journey Navigating Laser Vision CorrectionREFERENCESThis is the clinical protocol of the author used in her clinic. TheCE-approved range for ReLEx SMILE is: Sphere: -0.50 to -10.00D;Cylinder: 0 to 5.00 D; Spherical equivalent: -0.50 to -12.50D.14
Enhancement Options After SMILEWalter Sekundo MD, PhD, Chairman of the Department of Ophthalmology,Philipps University of Marburg, GermanyWith more than 1.5 million proceduresworldwide performed by more than 1,300surgeons in 65 countries, together with agrowing and impressive body of evidence inthe scientific literature, I think it is safe to say that SMILE has already established its credentials as a safe, accurateand efficacious refractive surgical procedure. Nevertheless,the reality of refractive surgery is that sometimesenhancements
such as the Haigis-L and tools such as the ASCRS online IOL calculator. We are definitely looking forward to using the TK formula of the IOLMaster 700 in post-LASIK cases. The measurement of the posterior corneal surface will help us i