Transcription
Update on PostRefractive SurgeryIOL CalculationsHawaiian Eye 2014KauaiRhonda G WaldronMMSc, COMT, CRA, ROUB, RDMSDiagnostic Echographer, Senior Associate in OphthalmologyEmory Eye CenterAtlanta,GAOwner, Eye Scan Consultingrhondawaldron@comcast.net
Financial DisclosuresResearch Funds: Accutome; Carl ZeissMeditec; Ellex; Haag-Streit USA; QuantelMedical; Sonomed Escalon
We must first get the correctaxial length! Eyes 25.0 mm or longer:Optical tends to measurelong eyes too long –hyperopic surprisesreported - do immersionand B-scan biometry toverify
Long Eye:Optical vs. Ultrasound28.51 mm28.37 mm28.10 mm28.09 mmPost-op using I mm:OD: -0.75 1.25 X 140 (SE -0.125)OS: -0.50 0.50 X 008 (SE -0.25)
Optimizing Axial Length in Long EyesWang, et al, J Cataract Refract Surg 2011; 37:2018-2027 Holladay I formula:0.8814 x AL(IOLM) 2.8701 Adjusted AL Haigis formula:0.9621 x AL(IOLM) 0.6763 Adjusted AL SRK/T formula:0.8981 x AL(IOLM) 2.5637 Adjusted AL Hoffer Q formula:0.8776 x AL(IOLM) 2.9269 Adjusted AL
Optimizing Axial Length in Long Eyes The problem with using an optimizationequation is that sometimes optical gets itright! Adjusting a measurement that didn’tneed adjusting will still lead to a post-opsurprise The best way to measure the high myopeis with ultrasound so you know it iscorrect
Immersion Technique Probe immersed inshell of saline Most accurate/nocorneal compression(0.015 - 0.05 mmdepending onmanufacturer) The method to whichoptical wascalibrated in itsdevelopment
Why High Myopes areHarder to Measure
Why High Myopes areHarder to Measure The eye is misshapen, oval or elongatedrather than round Macula on a “slope” Perpendicularity impossible
Posterior Staphyloma Uvea bulging into thin,stretched sclera Commonly in posteriorpole Perpendicularityimpossible Measurements varygreatly
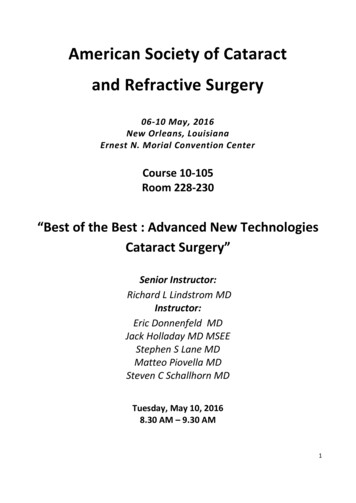
B-Biometry Technique Align B-scan with “HMAC”position (probe on cornealvertex, marker nasal) with 4or 5 mm of gel on probe tip Corneal vertex andposterior lens surfacecentered on left, maculacentered on right inferior tooptic nerve Macula 4.5 mm down fromcenter of optic disc Place one caliper on frontof cornea, move the otherthrough the center of thelens to macular surface
If you don’t see the cornea,you aren’t using enough gel!
B-biometry 30.34 mmA-scan 30.03,30.26, 30.0, 30.20,30.15, 29.98
B-Biometry TechniqueComparison to Good Immersion23.78 on A-scan23.80 on B-scan
IOL Calculationsafter Refractive Surgery
The Post-Refractive SurgeryKeratometry Challenge Central cornea either flattened (myopiccorrection) or steepened (hyperopiccorrection), causing erroneous readingsfrom standard keratometers Readings now either underestimated oroverestimated by reading the wrong area Results in hyperopic surprise aftermyopic correction, myopic surprise afterhyperopic correction if not addressed
So What Do We Do?
Clinical History MethodKoch, et al AJO 1989; 108:676-82 Previously considered “Gold Standard”,but now one of least favored methods Need three numbers:1. Pre-Op MR (sph eq)2. Pre-Op K’s (average)3. Post-Op MR (sph eq)
Clinical History MethodKoch, et al AJO 1989; 108:676-82For example: Average K pre-LASIK 45.75 D - 5.00 D myope pre-LASIK - 0.25 D myope post-LASIK Change in MR 4.75 D K 45.75 D - (4.75 D) 41.00 D-10-9-8-7-6-5 -4--33--224.75-1012345678910
Shammas PLfor Myopic LASIKShammas, et al AJO 2003; 136:426-32 Measure K’s post-op ( IOL Masteror Sim K preferred), average, thenK 1.14 (K post-op) - 6.8 In his study, 93.3% within 1D oftarget
Shammas PHLFor Hyperopic LASIK Presented at ASCRS 2013 Accepted for publicationKc 1.0457 (Kpost-op) – 1.9538
Wang-Koch-Maloney MethodWang, Booth, Koch. Ophthalmol 2004; 111(10):1825-1831For myopic LASIK patients: Obtain topography post-op, thenK 1.114 (Ccp) – 6.1Where Ccp is the central corneal power withcursor at the exact center of the Axial MapRecommend using Atlas topographer
Masket MethodMasket S, Masket SE. JCRS 2006; 32:430-434 Best performance in recent studies forPRK and LASIK patients (not RK!) Must know amount of correction fromhistory (LSE spherical equivalent ofchange after laser vision correction)IOL Adjustment LSE x (-.326) 0.101
Masket MethodMasket S, Masket SE. JCRS 2006; 32:430-434 Adjust final power, not measurementsUsed IOLM K’s and Biometry for studyMay use Sim K and immersion insteadNo need to determine corneal powerMean outcome -0.15 D, 28 out of 30 eyeswithin 0.5 D of target
Masket Formula ExamplesPrior Myopia (use SRK/T ): Formula yields 16.0 D LSE -6.00 D -6.0 X (-0.326) 0.101 2.057 16.0 2.0 18.0 D Final IOL Power
Masket Formula ExamplesPrior Hyperopia (use Hoffer Q): Formula yields 22.0 D LSE 3.0 D 3.0 X (-0.326) 0.101 - 0.877 22.0 – 1.0 21.0 D Final IOL Power
Haigis L For both myopic and hyperopicLASIK Measure the patient on opticalbiometer as always and chooseHaigis L for either myopic orhyperopic LASIK No other modifications necessary!
Haigis L For myopia, Haigis L has acorrection function for IOL Masterkeratometry plus a correctionfactor for the ACD change (0.5mm steeper since part of cornearemoved) due to ablation – nohistory required For hyperopia, since no ablation,has correction function for K’sonly
ASCRS websitePost-Refractive SurgeryIOL Calculatorwww.ASCRS.org(link at top of home page)Uses Holladay I with double K method
Prior Myopic LASIK/PRK
Prior Myopic LASIK/PRK
Prior Myopic LASIK/PRK From results from thousands of eyes at two majorcenters, methods in second and third columnsperformed better than those of the first column Now shows average of 2nd and 3rd columns aboveaverage from entire calculator
Prior Myopic LASIK/PRKBest results were from Masket,Shammas, Haigis-L, and WangKoch-Maloney
Prior Hyperopic LASIK/PRK
Prior Hyperopic LASIK/PRK
Prior RK
Prior RK
RK Patients History method not as good forpost-RK due to unstable post-oprefraction Measure them in morning ratherthan afternoon – K’s flatter in theam, steeper in pm Make them plano in the am, myopicin pm – not hyperopic am, planopm!
RK Patients Aim for -0.75 or -1.00 in post-RKpatients because of hyperopic shift overseveral years Don’t want them to drift into hyperopia drift into plano instead After RK, many patients have ahyperopic surprise that will settle outover time Do NOT do IOL exchange until after 2stable refractions on 2 different visits atleast 2 months out!
Patient Unsure Patient had LASIK OU, wasn’t sure what type When asked if she was nearsighted or farsightedbeforehand, her answer was “both”
Patient Unsure Patient had LASIK on OS only to be able to read upclose (monovision) Was plano OU beforehand Would that be myopic or hyperopic LASIK?
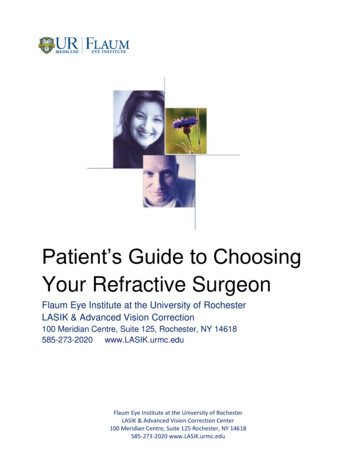
TopographyMyopic LASIK Flat zone centrally
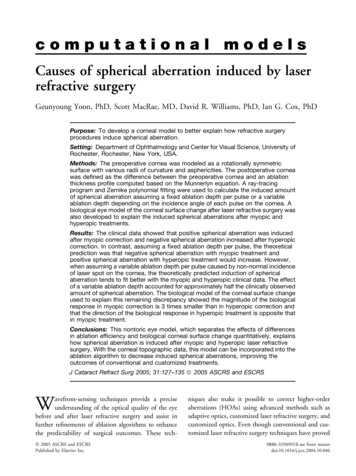
TopographyHyperopic LASIK Steep zone centrally
Conclusion ALL methods require good data in! If measurements are not accurate,none of the methods work! Don’t forget to use ultrasound forlong eyes!
Thank you!
Mahalo!
Prior Myopic LASIK/PRK From results from thousands of eyes at two major centers, methods in second and third columns performed better than those of the first column Now shows average of 2nd and 3rd colu