Transcription
computational modelsCauses of spherical aberration induced by laserrefractive surgeryGeunyoung Yoon, PhD, Scott MacRae, MD, David R. Williams, PhD, Ian G. Cox, PhDPurpose: To develop a corneal model to better explain how refractive surgeryprocedures induce spherical aberration.Setting: Department of Ophthalmology and Center for Visual Science, University ofRochester, Rochester, New York, USA.Methods: The preoperative cornea was modeled as a rotationally symmetricsurface with various radii of curvature and asphericities. The postoperative corneawas defined as the difference between the preoperative cornea and an ablationthickness profile computed based on the Munnerlyn equation. A ray-tracingprogram and Zernike polynomial fitting were used to calculate the induced amountof spherical aberration assuming a fixed ablation depth per pulse or a variableablation depth depending on the incidence angle of each pulse on the cornea. Abiological eye model of the corneal surface change after laser refractive surgery wasalso developed to explain the induced spherical aberrations after myopic andhyperopic treatments.Results: The clinical data showed that positive spherical aberration was inducedafter myopic correction and negative spherical aberration increased after hyperopiccorrection. In contrast, assuming a fixed ablation depth per pulse, the theoreticalprediction was that negative spherical aberration with myopic treatment andpositive spherical aberration with hyperopic treatment would increase. However,when assuming a variable ablation depth per pulse caused by non-normal incidenceof laser spot on the cornea, the theoretically predicted induction of sphericalaberration tends to fit better with the myopic and hyperopic clinical data. The effectof a variable ablation depth accounted for approximately half the clinically observedamount of spherical aberration. The biological model of the corneal surface changeused to explain this remaining discrepancy showed the magnitude of the biologicalresponse in myopic correction is 3 times smaller than in hyperopic correction andthat the direction of the biological response in hyperopic treatment is opposite thatin myopic treatment.Conclusions: This nontoric eye model, which separates the effects of differencesin ablation efficiency and biological corneal surface change quantitatively, explainshow spherical aberration is induced after myopic and hyperopic laser refractivesurgery. With the corneal topographic data, this model can be incorporated into theablation algorithm to decrease induced spherical aberrations, improving theoutcomes of conventional and customized treatments.J Cataract Refract Surg 2005; 31:127–135 ª 2005 ASCRS and ESCRSWavefront-sensing techniques provide a preciseunderstanding of the optical quality of the eyebefore and after laser refractive surgery and assist infurther refinements of ablation algorithms to enhancethe predictability of surgical outcomes. These tech-ª 2005 ASCRS and ESCRSPublished by Elsevier Inc.niques also make it possible to correct higher-orderaberrations (HOAs) using advanced methods such asadaptive optics, customized laser refractive surgery, andcustomized optics. Even though conventional and customized laser refractive surgery techniques have proved0886-3350/05/ -see front matterdoi:10.1016/j.jcrs.2004.10.046
CORNEAL BIOMECHANICS: SPHERICAL ABERRATION AFTER LASER REFRACTIVE SURGERYeffective in improving patient visual performance, abetter understanding of the wave aberration induced bya laser ablation procedure is required to achieve greaterimprovement in vision.Clinical observation shows that laser refractivesurgery increases HOAs, mainly spherical and coma1–5(Llorente L, et al. IOVS 2002; 43:ARVO E-Abstract2006). In particular, spherical aberrations induced bya procedure show a clear tendency that positivespherical aberration is induced after myopic treatmentand a strong correlation with the amount of attempteddioptric power correction in myopic and hyperopictreatments. Spherical aberration is not only 1 of themost important HOAs that degrade retinal imagequality; it also affects the subjective refraction ofdefocus because of the interaction between defocus andspherical aberration.6 In other words, adding anappropriate amount of defocus when spherical aberration exists can make retinal image quality better thanthe same amount of spherical aberration with zerodefocus. Therefore, if a significant amount of sphericalaberration is uncorrected or induced after a surgicalprocedure, the full correction of defocus may not bethe best way to obtain the best surgical outcomes.Several studies propose possible reasons for induced spherical aberrations as well as algorithms to correct them. Holladay and coauthors7 report that cornealasphericity increases after laser in situ keratomileusis(LASIK) for myopia, causing a functional visiondecrease. Jı́menez and coauthors8 developed a theoret-Accepted for publication October 28, 2004.From the Department of Ophthalmology (Yoon, MacRae) and Centerfor Visual Science (Yoon, MacRae, Williams), University of Rochester,and Bausch & Lomb (Cox), Rochester, New York, USA.Supported by grants from the National Institutes of Health(R01-EY014999), the Research to Prevent Blindness, and NYSTAR(CEIS) and a research grant from Bausch & Lomb.Presented in part at the annual meeting of the Association for Researchin Vision and Ophthalmology, Ft. Lauderdale, Florida, USA, May2003.Drs. Yoon and Williams are consultants to Bausch & Lomb andreceive royalties based on the Zyoptix system. None of the other authorshas a financial or proprietary interest in any material or methodmentioned.Reprint requests to Geunyoung Yoon, PhD, Center for Visual Science,University of Rochester, 262 Meliora Hall, Rochester, New York14627, USA. E-mail: yoon@cvs.rochester.edu.128ical equation that represents the change in cornealasphericity. Gatinel and coauthors9,10 also theoreticallypredicted corneal asphericity changes after myopic andhyperopic laser refractive surgery. In a recent study,Anera et al.11 made similar conclusions and found thata greater increase in corneal asphericity and subsequentdecrease in visual performance were observed withhigher degrees of myopia.Changes in corneal asphericity can explain some ofthe induced spherical aberration because when the radiusof curvature of a cornea is constant, corneal asphericity isa predominant factor affecting the amount of the aberration. The corneal wound-healing process could be another reason laser ablation induces HOAs. Huang andcoauthors12 developed a mathematical model of cornealsurface smoothing. They mathematically modeled epithelial thickness modulations to explain regression andinduction of the aberrations clinically observed afterlaser ablation. Porter et al.13 recently found that inLASIK, the laser ablation, not the microkeratomecut, seems to be a bigger factor in inducing sphericalaberration. However, there was wide variation in theresponses of other Zernike modes across patients afterthe flap was cut.Mrochen and Seiler14 propose that the ablationdepth per laser pulse across the cornea varies under theinfluence of a difference in the effective illuminationarea and reflection losses that occur during laser–tissueinteraction. Jı́menez and coauthors15 theoretically investigated the effect of laser-ablation algorithms ofreflection losses and the non-normal incidence of laserpulse on the anterior cornea. Dupps and Roberts16 andRoberts17,18 propose another mechanism for inducedspherical aberration after surgery; that is, corneal shapeor curvature change caused by the biomechanical response of the cornea.Some studies propose modified ablation algorithms to compensate for the spherical aberration.Schwiegerling and Snyder19 developed the ideal ablation pattern to correct the introduced spherical aberration based on clinical data after photorefractivekeratectomy. Manns and coauthors20 calculated thecorneal asphericity of a postoperative cornea that produces zero primary spherical aberration.More precise understanding of the sources ofinduced spherical aberrations is needed for moreeffective correction of lower-order aberrations andJ CATARACT REFRACT SURG—VOL 31, JANUARY 2005
CORNEAL BIOMECHANICS: SPHERICAL ABERRATION AFTER LASER REFRACTIVE SURGERYHOAs. However, there is little evidence on how laserrefractive surgery induces spherical aberrations. In thispaper, we hypothesize that 2 factors induce sphericalaberration: (1) the variable laser ablation depth perpulse at different locations on the cornea that is causedby the oblique incidence of the laser spot and (2) thecorneal shape change caused by the biological responseof the cornea. We use the term biological response torepresent factors that may occur during and after laserrefractive surgery. The factors could include the biomechanical and wound-healing responses of the corneaand unexpected corneal surface change caused by imperfect laser ablation. A theoretical eye model based onclinical observations was developed. The model takesinto account the effects described above. We sought toseparate the effect of each factor on induced sphericalaberration. We also demonstrated that our model canquantitatively predict the change in corneal asphericity.Patients and MethodsThe aberration data were collected at the RefractiveSurgery Center, University of Rochester, under protocolapproved by the University of Rochester Research SubjectReview Board. All patients signed an informed consentbefore they participated in the study.Preoperative and postoperative spherical aberrationswere measured with a Shack-Hartmann wavefront sensor(Zywave, Bausch & Lomb) in 32 myopic and 17 hyperopiceyes. Corneal asphericity in the same eyes was measuredwith an Orbscan II corneal topographer (Bausch & Lomb).All postoperative measurements were done 1 month afterlaser refractive surgery. The magnitude of sphericalaberration for a 6.0 mm pupil was expressed in microns asthe Zernike coefficient corresponding to spherical aberration(Z 04 ). All eyes had conventional LASIK with a Technolas217 laser (Bausch & Lomb). The nomogram and ablationprofile design were not adjusted preoperatively. Changes inthe measured spherical aberration and asphericity betweenpreoperative and postoperative values were compared withthe theoretical prediction on the basis of the aspheric corneamodel. The attempted correction of spherical refractive errorranged from C5.19 diopters (D) to 6.48 D.Model of the Spherical CorneaThe cornea can be expressed as a rotationally symmetricsurface with different radii of curvature and asphericities(conic constant or shape factor). A rotationally symmetricsurface, C (x), can be mathematically defined by the following equation:C ðxÞ ¼cx ffiffiffiffiffiffiffiffiffiffiffiffiffiffi1 þ 1 ð1 þ kÞc 2 x 2ð1Þwhere x is the radial distance from the cornea’s center, k isasphericity, and c is the reciprocal of the corneal radius ofcurvature. A surface with k O 0, k Z 0, and 1 ! k ! 0represents an oblate spheroid, sphere, and prolate spheroid, respectively. This equation was used to define thepreoperative aspheric cornea. In the calculation of sphericalaberration induced by laser ablation, a conic constantof 0.3 and a radius of curvature of 7.8 mm were assumedas preoperative corneal parameters. These values werechosen as an average, although a wide range of radii ofcurvature and asphericity of the normal cornea has beenreported.To obtain the postoperative cornea, an ablationthickness profile was calculated with the spherical Munnerlyn algorithm.21 The effect of the oblique incidence of thelaser spot across the cornea on the ablation depth was takeninto account when the ablation profile was computed. Theequations proposed by Mrochen and Seiler15 were used tocalculate the loss of ablation depth per pulse caused by thenon-normal incidence of the laser spot. This calculatedablation depth per pulse with the effect of oblique incidenceof the laser spot is referred to as the variable ablation depthin this paper. The postoperative cornea, CpostOP(x), was simply defined by subtracting the ablation profile from thepreoperative cornea as shown by CpostOP x ¼ CpreOP x Tablation rð2Þwhere CpreOP(x) is a preoperative corneal profile calculatedfrom the equation 1 and Tablation(x) is an ablation thicknessprofile based on the Munnerlyn algorithm.Calculation of Spherical AberrationOnce the preoperative and postoperative cornealsurfaces were calculated, a conventional ray-tracing program(CodeV, Optical Research Associates) was used to computethe spherical aberration generated by the preoperative andpostoperative corneal surface profiles. With the sameprogram, Zernike polynomials were fit to the ray-tracingresults to compute the magnitude of Zernike sphericalaberration (Z 04 ) for comparison with the clinically measureddata. The sign convention of spherical aberration recommended by the VSIA Standards Taskforce team22 was used.This simulation was conducted for a range of correctionfrom 10.0 D (myopic treatment) to C10.0 D (hyperopictreatment) in 1.0 D steps. The asphericity of preoperativeand postoperative corneas was also calculated to evaluate theeffect of laser ablation on the change in corneal asphericity.All spherical aberration and corneal asphericity measurements and calculations were for a 6.0 mm pupil.J CATARACT REFRACT SURG—VOL 31, JANUARY 2005129
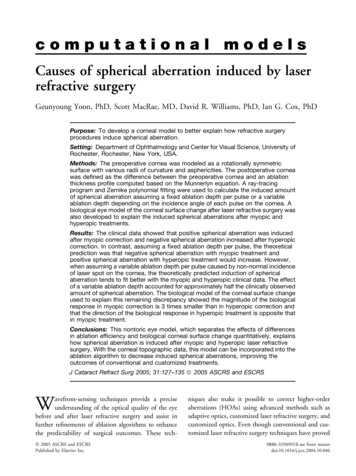
CORNEAL BIOMECHANICS: SPHERICAL ABERRATION AFTER LASER REFRACTIVE SURGERYResultsSpherical Aberration of Rotationally Symmetric CorneaFigure 1 shows the spherical aberration generatedby rotationally symmetric corneal surfaces with different radii of curvature and asphericities. More positive spherical aberration is produced with a larger conicconstant (more oblate spheroid). If the conic constantis larger than that of the spherical aberration-freecornea, a smaller radius of curvature (steeper cornea)would cause more positive spherical aberration. Theconic constant in which the spherical aberration is zerois independent of the radius of curvature when the refractive index is constant. The conic constant for thespherical aberration-free cornea is approximately 0.53 when the refractive index of the cornea isassumed to be 1.376.Spherical Aberration Induced by Refractive SurgeryFigure 2 summarizes clinical observations of thechange in spherical aberration after myopic and hyperopic LASIK. Change in the spherical aberration expressed as a Zernike coefficient, Z 04 , is the differencebetween preoperative and postoperative spherical aber-Figure 1. Theoretical calculation of spherical aberration produced by a rotationally symmetric cornea with different radii ofcurvature (7.0 mm, 7.8 mm, and 8.5 mm) and asphericities (conicconstant), k, ranged from 1.5 to 1.5. Spherical aberration is zerowhen corneal asphericity, k, equals 0.53 when the refractive indexof the cornea is 1.376.130ration; that is, postoperative spherical aberration –preoperative spherical aberration. In myopic treatment,positive spherical aberration increased. However, negative spherical aberration increased after hyperopictreatment. In both procedures, there was a significantcorrelation between the induced spherical aberrationand the amount of the attempted defocus correction.Separate regression analysis of the myopic data and thehyperopic data yielded a correlation coefficient (r) of66% and 64%, respectively. Based on these data, thecorrelation between the change in spherical aberrationand the attempted defocus correction can be describedby the following linear equations:DSA myopic ¼ 0:0465 ! D 0:0096 in myopiccorrection ð3ÞandDSAhyperopic ¼ 0:0952 ! D 0:1961 in hyperopiccorrection ð4Þwhere DSA is the induced spherical aberration and D isthe attempted defocus correction in diopters. Corresponding regression functions of equations 3 and 4 arerepresented by solid gray lines in Figure 2.From the slopes of equations 3 and 4, with thesame amount of defocus correction, the magnitude ofthe induced spherical aberration by a hyperopic procedure is larger than that induced by a myopic procedure by a factor of approximately 2.Effect of Oblique Incidence of Laser SpotA conventional algorithm that has been used tocalculate an ablation profile in laser refractive surgery isbased on the Munnerlyn equation that assumesa constant ablation depth of each laser pulse over theentire cornea. Recent studies, however, propose theablation depth is variable, mainly due to the obliqueincidence of laser pulse on the cornea. Because thecorneal surface is curved, the efficiency of laser ablationdecreases as each pulse hits the cornea farther from thecenter. Maximum ablation efficiency can be achievedwhen the laser pulse hits the corneal surface witha normal incidence angle. Figure 3 shows the calculated spherical aberration induced by conventionalrefractive surgery with fixed and variable ablationdepths. An induced spherical aberration with a fixedJ CATARACT REFRACT SURG—VOL 31, JANUARY 2005
CORNEAL BIOMECHANICS: SPHERICAL ABERRATION AFTER LASER REFRACTIVE SURGERYablation depth is shown by the dashed line. In both themyopic and hyperopic groups, the theoretical expectation with the fixed ablation depth has a tendency tobe opposite that of the clinical data, represented bysolid circles. Theoretically, more negative and positivespherical aberrations are induced in myopic correctionsand hyperopic corrections, respectively.However, with the variable ablation depth (solidline in Figure 3) caused by the oblique incidence of thelaser spot, there is qualitative agreement with the clinical data. Positive spherical aberration in myopic correction tends to increase with a larger amount of defocuscorrection. Almost no spherical aberration in hyperopic correction is induced. However, a significant quantitative discrepancy between the theory and clinicaldata remains, although the overall tendency of thetheoretical prediction seems to better fit the clinicaldata than with a fixed ablation depth.Effect of Biological Response of the CorneaA hypothesis that could account for this remainingdiscrepancy is the biological response of the cornea. Inmyopic treatments, corneal biomechanics cause thecentral cornea to flatten and the peripheral cornea tosteepen. The corneal epithelium after refractive surgerytends to fill in the abruptly changed surface to maintain a smooth surface profile. This corneal woundhealing response is included in biological factors forhypothesis. In simulation, the biological response ofthe cornea in terms of the amount of flattening andsteepening required to account for the observedinduced spherical aberration was quantitatively modeled. Figure 4 shows a biological model used tocalculate the theoretical effect of the biological cornealsurface change on the induced spherical aberration. Inmyopic treatment (Figure 4, top), the optical zone isdivided into flattening and steepening zones. Theflattening zone diameter is assumed to correspond toa central area that is 1.0 mm smaller than the opticalzone diameter. Therefore, the steepening zone is anouter annular area with a width of 0.5 mm. In hyperopic treatment (Figure 4, bottom), the steepening andflattening zones are defined as a central area and anouter annular area, respectively. The magnitude of thebiological effect, Mbio, is defined as a percentage of theamount of defocus correction in diopters. The actualFigure 2.Clinically observed change in spherical aberration inmyopic and hyperopic corrections expressed as a Zernike coefficient(Z 04) in microns. The change was computed by subtracting themeasured preoperative spherical aberration from the postoperativeone. The gray lines represent the best-fit linear regression performedon myopic and hyperopic data separately.Figure 3.Theoretical expectations of the induced sphericalaberration when assuming the fixed ablation depth per pulse(dashed line) and the variable ablation depth (solid line) due t
Geunyoung Yoon, PhD, Scott MacRae, MD, David R. Williams, PhD, Ian G. Cox, PhD Purpose: To develop a corneal model to better explain how refractive surgery procedures induce spherical aberration. Setting: Department of Ophthalmology and Center for Visual