Transcription
Indiana Public HealthSystem ReviewI U R I C H A R D M . FA I R B A N K S S C H O O L O F P U B L I C H E A LT HDecember 2020
C R E D I TSProject LeadsPaul K. Halverson, DrPH, FACHE, MSHA, is the Founding Dean and Professor of the IU Richard M. Fairbanks School PublicHealth. He holds additional appointments at the IU School of Medicine and the Regenstrief Institute. Halverson previouslyserved as the State Health Officer in Arkansas and as a Division Director at the US Centers for Disease Control and Prevention.Valerie A. Yeager, DrPH, MPhil, is an Associate Professor in the Department of Health Management and Policy. Previously,Yeager was a Lister Hill Policy Fellow in the Division of Global Migration and Quarantine at the Centers for Disease Controland Prevention. Her research focuses on public health systems and services across local, state, and federal levels.External Consultants and ReviewersGlen P. Mays, PhD, MPH, Professor and Chair, Department of Health Systems, Management and Policy, Colorado Schoolof Public Health, Anschutz Medical Campus; Former Coordinating Center Director, Public Health Systems and ServicesResearch, Robert Wood Johnson Foundation.Hugh Tilson, MD, DrPH, Senior Advisor to the Dean of the Richard M. Fairbanks School of Public Health; Adjunct Professor,UNC Gillings School of Global Public Health, Co-Chair of the Institute of Medicine’s 1988 Future of Public Health Report;former North Carolina State Health Officer and former Local Public Health Director in Oregon and Maine.With contributions fromAmber Blackmon, MPHAmanda Briggs, MSJyotsna Gutta, MPHHarold Kooreman, MA, MSWNir Menachemi, PhD, MPHNadia Unruh Needleman, MSJoshua R. Vest, PhD, MPHThe authors wish to express sincere gratitude to all participants who shared their experiences and insights via participation ina qualitative interview.This report is made possible by funding from the Richard M. Fairbanks Foundation.2IU Richard M. Fairbanks School of Public Health
TA B L E O F C O N T E N T SExecutive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Section 1: Introduction to Public Health Systems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Section 2: The Public Health System in Indianaand Comparison States . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Section 3: Evidence Synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Section 4: Qualitative Insights from Key Stakeholders in Indiana . . . . . . . . . . . . . . . . 55Section 5: Recommendations for Public Health System Change . . . . . . . . . . . . . . . . . . 64Section 6: Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82IU Richard M. Fairbanks School of Public Health3
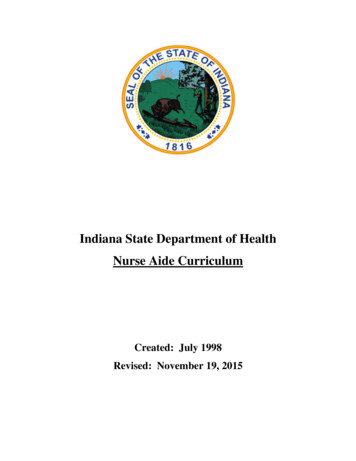
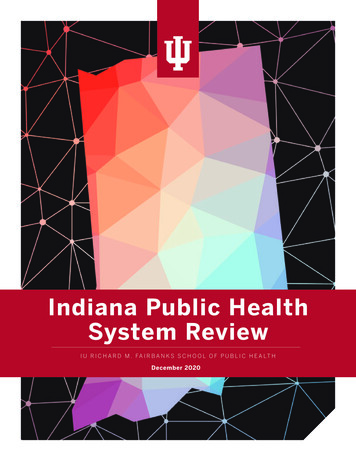
EXECUTIVE SUMMARYEXECUTIVE SUMMARYPublic health is “the science and art of preventingdisease, prolonging life and promoting health throughthe organized efforts and informed choices of society,organizations, public and private communities, and6individuals”. In the period of the 20th century, the UShas gained an additional 30 years in life expectancy,and 25 of those 30 years are attributed to public healthefforts. As a field, public health includes expertise inbiostatistics and informatics, epidemiology, healthpolicy and management, social and behavioral health,and environmental health. In practice, this expertiseincludes activities that influence the social and physicalenvironments in which we live, policies and interventionsthat influence behaviors, and assuring access toessential and high quality health care. More specifically,public health activities include a wide range of activitiessuch as identifying and tracking food-borne pathogens,intervening in an outbreak, educating communities,inspecting restaurants, training restaurant workers inRegardless of where you live, all people in Indiana deservea strong public health system, one that protects andimproves the health of your community and is basedon science and data. However, today, the extent andquality of public health services that are available in yourcommunity is entirely dependent on what county you livein. Because most individuals are often not aware of what“good public health” looks like, or when they might need it,they generally do not choose to live in a county based onthe public health services available. Fortunately, the workof defining what “good public health” looks like and how tomeasure it is well established and guidance from that workcan be used to inform improvements to Indiana’s publichealth system. This study examines the current state of1-5Indiana’s public health system. In particular, this reportfocuses on the centerpiece of the public health system the network of local and state governmental public healthagencies - their structure, human and financial resources,authorities, and activities.THE 10 ESSENTIALPUBLIC HEALTHSERVICESBuild and maintain astrong organizationalinfrastructure forpublic healthTo protect and promote the health of allpeople in all communitiesThe 10 Essential Public Health Servicesprovide a framework for public healthto protect and promote the health of allpeople in all communities. To achieveoptimal health for all, the Essential PublicHealth Services actively promote policies,systems, and services that enable goodhealth and seek to remove obstacles andsystemic and structural barriers, such aspoverty, racism, gender discrimination,and other forms of oppression, that haveresulted in health inequities. Everyoneshould have a fair and just opportunity toachieve good health and well-being.Improve and innovatethrough evaluation,research, and qualityimprovementInvestigate,diagnose, andaddress healthhazards androot causesBuild a diverse andskilled workforceSource: s andmonitorpopulationhealthIU Richard M. Fairbanks School of Public HealthStrengthen, support, andmobilize communitiesand partnershipsEnable equitableaccessUtilize legaland regulatoryactionsCreate, champion,and implement policies,plans, and laws
EXECUTIVE SUMMARYfood-borne illness prevention, and developing policiesto make food processing safer. It also includes assuringthat children are immunized, tracing infectious diseasesand contacting individuals who may have been exposed,and leading communities in public health emergenciesand disasters such as an event that compromises ourwater systems, or in outbreaks such as the COVID-19pandemic.(LHDs), where many of the essential, community-facingpublic health activities are conducted, is typically sharedacross federal, state, and local sources with the averageUS LHD receiving a quarter of its funding from localfunds. However, Indiana’s LHDs rely on local sourcesfor the majority of their budgets, unlike most otherUS communities that rely equally on state and federal(passthrough) funding in addition to local funding.Clarifying what public health is and what services itshould provide is an essential goal of this report. In fact,one of the most important findings of this study is thatmany key state stakeholders are unable to differentiatebetween public health and healthcare. While both work toimprove the health of Hoosiers, public health is focusedon preventing illness and protecting the populationfrom injury, communicable diseases, and prematuredeath whereas, the vast majority of the time, healthcareprimarily serves to treat disease and injury and is focusedon making people well again. Unfortunately, when we areunable to differentiate between these two roles, makinga case for investing more in the public health system ischallenging, especially given the existing high costs ofhealth care in our state.This ensures that less resourced communities that likelyhave a greater need for the protection and preventiveservices public health provides also have less funding andless capacity to ensure that they receive them. Althoughthere is value in having direct local connections in everycounty, the current structure ensures that many of the 94LHDs are able to provide only a fraction of the necessarypublic health services and expertise that should beavailable to all communities. Epidemiologic expertise,data analytics to inform education and services relevantto the needs of communities, emergency preparednesscapabilities, and an information technology infrastructurethat allows for an efficient and effective system are skillsand tools that are not present in many of Indiana’s localsettings. This missing expertise and resources translatesto paper-based reporting systems and delays in routineoutbreak identification for diseases like syphilis and HIV– triggers that should alert officials about acute crisesearlier rather than later. It also means that public health isoften not factored into local policymaking or communitydecisions. While it may be difficult to imagine, during theearly response to the COVID-19 pandemic, there wereLHDs in Indiana that literally closed their doors and werenot participating in the response or available to theircommunities. It cannot be more obvious that the publichealth system is not functioning as a system when LHDsare not seamlessly plugged into a statewide response toa pandemic.Evidence shows that when communities invest more inpublic health, they actually spend less on health careand live longer. However, findings presented in thisreport show that Indiana communities are less likely tobe implementing nationally recommended public healthactivities compared to other states. Further, Indiana’scommunities receive less public health funding comparedto neighboring states, companion states, or exemplarstates. Funding for local public health departmentsHealth is a dynamic state of complete physical,mental, spiritual, and social well-being and notmerely the absence of disease or infirmity.World Health Organization, 1998Public health is “what we as a society docollectively to assure the conditions in whichpeople can be healthy.”Institute of Medicine, 1988These issues are not for lack of dedication of the publichealth workers at the local or the state levels. These areissues of a system that has been chronically underfundedand undervalued. In fact, one thing that is consistent is thatpublic health investments in Indiana are routinely belowUS averages and frequently among the lowest acrossneighboring, companion, and exemplar states. America’sHealth Rankings rank Indiana 48th for public health funding.Funding at the local level is particularly low compared toIU Richard M. Fairbanks School of Public Health5
EXECUTIVE SUMMARYother states. The national median funding among LHDs is 41 per capita and the 25th percentile is 23 per capita,but the majority of LHDs in Indiana have per capita budgetsfar below these levels. In fact, at least 37 of the 94 LHDs inIndiana have per capita budgets of less than 10 per capita.Understanding how Indiana’s public health system isstructured and financed is important in the contextof benchmarking health outcomes across states.For example, Indiana ranks 41st among all states onpublic health and is at least 10% below the US averagerate for preventable mortality such as infant deaths,accident deaths, and alcohol, drug, and suicide deaths.In terms of prevention, Indiana has particularly lowrates of vaccinations for influenza, childhood vaccines,and adult and elderly vaccines, and the state scores inthe bottom tier nationally with respect to public healthpreparedness. Indiana also has one of the highest ratesof adult smokers in the nation (21.8% compared to thenational average of 17.1%), contributing to higher rates ofpreventable chronic diseases and cancers.Based on feedback from stakeholders, Indiana’scommunities are ready for change and willing to worktogether to make improvements to the public healthsystem. A total of 49 stakeholders participated in an6IU Richard M. Fairbanks School of Public Healthinterview for this report and contributed feedback and/or ideas for improvements to the public health system inIndiana. The review of the scientific evidence for publichealth systems change presented in Section 3 and theinsights provided by Indiana stakeholders in Section 4informed the recommendations in this report.In general, the recommendations are focused onachieving better health for Hoosiers through a morerobust public health system and one that ensures thatthe Foundational Public Health Services are providedto all communities. A stronger, appropriately-fundedpublic health system means better capacity at the localand state levels and improved effectiveness of publichealth efforts. These improvements will allow Indiana’spublic health agencies to work with public healthpartners and to have a bigger collective impact andbegin to address the upstream social determinants ofhealth. Indiana’s public health system needs substantialfunding increases at both the state and local levels. Fouroverarching recommendations are presented in Section5. These include:1.Create a uniform approach to deliver theFoundational Public Health Services (FPHS)across the state
EXECUTIVE SUMMARY2.3.4.Create a district-level mechanism to enableresource sharing among LHDsStrengthen the State Health Department’soversight and enabling capacity to support thelocal public health delivery systemUnder the auspices of the state board ofhealth, create a multi-disciplinary state-wideimplementation committee tasked with executingthe recommended implementation steps outlinedin Section 5In addition to the 4 recommendations, 15 implementationsteps necessary to improve the capacity and effectivenessof Indiana’s public health system are provided. In brief,these steps include the establishment of district levelcapacity that will provide resource-sharing of expertiseand services in support of existing LHDs. District officesshould be led by a full-time District Health Officerwith formal public health training. The District HealthOfficer should be supported by a district leadershipnetwork comprised of health officials/administratorsfrom each LHD within the district. Such a structure willprovide district-level strategies that are both resourcedand informed by expertise, local-level data, and localperspectives. Existing LHDs and district offices willwork together to provide a core package of public healthservices that is aligned with the Foundational PublicHealth Services for local public health and supports thestate public health system in assuring the 10 essentialservices across Indiana.Specific state-level improvements recommended inthis report include: structures to ensure expertise andessential skills across the state and local workforce;information systems that employ a common dataplatform and ensure real-time reporting at all levels of thepublic health system; state-wide standards that assurecontinuous quality and performance improvement; andimproved collaboration between the state and local levelsand with partners external to public so that the state canwork more effectively to improve the health of Hoosiers.The implementation of the recommendations in thisreport will need a clear path to implementation withfunding but with incremental rollout and should beinformed by an empowered state-wide committee madeup of state and local public health representatives as wellas state, county, and city leaders, health care leaders, andother key stakeholders. While priority should be givento the establishment of the district health offices andthe provision of core public health services, each of theimplementation steps will need to be strategically phasedinto the plan to improve Indiana’s public health system.Lastly, although all of the costs needed to makeimprovements to the public health system are notestimated in this report, estimates for the priorityactions (district health offices supported by a statelevel expertise and the provision of core public healthservices) have been provided along with potentialfunding mechanisms for consideration. Of particularimportance is the potential of an increase in tax on thesale of tobacco products, the most effective mechanismto reduce tobacco use. Revenue from an increasedtobacco tax should be dedicated to the public healthsystem and should fund the establishment of an IndianaPublic Health Trust Fund. The Trust Fund would allow forthe new revenue to generate interest and to support thephased implementation of public health improvements.The Trust Fund should be explicitly limited to ensuringthe provision of Foundational Public Health Servicesand related infrastructure for the public health system.As a matter of priority, an initial 50 million should bededicated in year one of this work with increases annuallyover 5 years so that the system has consistent, annualfunding of at least 338 million from the Public HealthTrust Fund. This consistent funding will allow public healthagencies to plan strategically for a future where Indianais among the top states in health outcomes rather thanthe bottom. There is a bi-directional connection betweenhealth and wealth, not just for individuals but for theircommunities and their economies.As the report indicates, substantial changes are neededto improve the Indiana public health system, and it is clearthat stakeholders are ready and willing to get started.Specific thanks and appreciation are due to the hundredsof public health workers at the state and local levels thattoil every day on behalf of the people of the state and whodo so without the resources they need to do the best jobthey can. This report was written to support their workand give them the tools they need to improve the publichealth system for Hoosiers. COVID-19 sounded the alarmand the status quo is no longer sufficient.IU Richard M. Fairbanks School of Public Health7
S E C T I O N 1 : I N T R O D U C T I O N T O P U B L I C H E A LT H S Y S T E M S A N D B A C K G R O U N DSECTION 1: INTRODUCTION TO PUBLIC HEALTHSYSTEMS AND BACKGROUNDThe US public health system includes local, state, andfederal governmental public health agencies as wellas numerous multisectoral partners including healthcare organizations, community-based organizations,schools, industry, and other governmental agencies. Withleadership from state and local public health departments,the public health system protects and promotes thehealth of all members of our communities. Through theprovision of the Essential Public Health Services, state andlocal agencies ensure policies, systems, and services thatenable good health and work to remove barriers to healthequity, ensuring that all individuals have the opportunity5to achieve good health and well-being (see Figure 1).efforts and informed choices of society, organizations,6public and private communities, and individuals”. Whilepublic health and medicine work together, the focusof public health is on prevention rather than curativeaspects of health. Additionally, public health is focusedon the population as a whole rather than one individualor one individual health issue. As a field, public healthincludes expertise in biostatistics, epidemiology, healthpolicy and management, social and behav
He holds additional appointments at the IU School of Medicine and the Regenstrief Institute. Halverson previously . Harold Kooreman, MA, MSW Nir Menachemi, PhD, MPH Nadia Unruh Needleman, MS Joshua R. Vest, PhD, MPH . there is value in having direct local connections in every coun