Transcription
8/17/202212American College of Gastroenterology1
8/17/202234American College of Gastroenterology2
8/17/2022Participating in the WebinarAll attendees will be muted andwill remain in Listen Only Mode.Type your questions here sothat the moderator can seethem. Not all questions willbe answered but we will getto as many as possible.5How to Receive CME and MOC PointsLIVE VIRTUAL GRAND ROUNDS WEBINARACG will send a link to a CME & MOC evaluation to allattendees on the live webinar.ABIM Board Certified physicians need to complete their MOC activities by December 31,2022 in order for the MOC points to count toward any MOC requirements that are due bythe end of the year. No MOC credit may be awarded after March 1, 2023 for this activity.6American College of Gastroenterology3
8/17/2022MOC QUESTIONIf you plan to claim MOC Points for thisactivity, you will be asked to: Please listspecific changes you will make in your practiceas a result of the information you receivedfrom this activity.Include specific strategies or changes that you plan to implement.THESE ANSWERS WILL BE REVIEWED.7ACG Virtual Grand RoundsJoin us for upcoming Virtual Grand Rounds!Week 34 – Thursday, August 25, 2022Update on the Management of Anticoagulants and AntiplateletGuidelinesFaculty: Neena S. Abraham, MD, MSc (Epid), FACGModerator: Bryan G. Sauer, MD, MSc (Clin Res), FACGThursday, August 25th at Noon Eastern and NEW! 8pm Eastern!Week 35 – Thursday, September 1, 2022ID for the GI – GI Presentations of Unusual InfectionsFaculty: Mark S. Riddle, MD, DrPHModerator: Freddy Caldera, DO, MS, FACGThursday, September 1st at Noon Eastern and NEW! 8pm Eastern!Visit gi.org/ACGVGR to Register8American College of Gastroenterology4
8/17/20229DisclosuresJasmohan S. Bajaj, MD, MS, FACGBausch: Grant/Research SupportBiovie: Grant/Research SupportCosmo Pharmaceuticals: Grant/Research SupportGrifols: Grant/Research SupportMallinckrodt Pharmaceuticals: Grant/Research SupportNorgine: Advisory Committee/Board Member (EndedOctober 1, 2021)Sequana: Grant/Research SupportDavid E. Bernstein, MD, MACGAbbVie: Consultant, Grant/Research SupportContus: Grant/Research SupportCymaBay: Grant/Research SupportGilead: Consultant, Grant/Research SupportNovartis: Grant/Research SupportNovo Nordisk: Grant/Research Support*All of the relevant financial relationships listed for these individuals have been mitigated10American College of Gastroenterology5
8/17/2022Acute‐on‐Chronic Liver DiseaseJasmohan S. Bajaj, MD, MS, FACGProfessor of Medicine,Division of Gastroenterology, Hepatology and NutritionVirginia Commonwealth University andCentral Virginia Veterans Healthcare SystemRichmond, Virginia111212American College of Gastroenterology6
8/17/2022Important questions What is acute on chronic liver disease or failure and how isit it different from decompensated cirrhosis and from acuteliver failure? How do we define and prognosticate patients with ACLF? What are the precipitants and potential preventionstrategies? What are the individual organ failures that we need tofocus on? Should ACLF patients be given priority for liver transplant? What are the future directions?13Case‐ ER presentation A 59-year-old man is brought to the emergency room (ER) by his wifefor new onset confusion and increased abdominal girth. Past medicalhistory is notable for uncontrolled diabetes, obesity, and social alcoholuse. On examination he is afebrile, alert, and oriented only to place.Abdominal examination revealed a fluid wave. He has not sought outpatient care for 3 years, although he underwentemergency surgery for a strangulated inguinal hernia 6 weeks ago. At hospital discharge, a PPI was initiated for “prophylaxis”. Notable admission labs include a serum creatinine 1.3 mg/dL, bilirubin2 mg/dL, albumin 3.1g/dL, INR 1.4, WBC count 7000/mL, and plateletcount 105x109/L.ACLF Guidelines to practiceAJG 202214American College of Gastroenterology7
8/17/2022Case‐ Initial Work‐up The patient has been in the ER for 8 hours and is finallyadmitted with diagnoses of cirrhosis, ascites, and HE. He isstarted on lactulose with some improvement in mental statusbut still has asterixis the next morning. Fourteen hours after initial presentation, a diagnosticparacentesis shows spontaneous bacterial peritonitis (SBP). His serum creatinine and WBC count have increased to 1.8mg/dL and 8600/mL respectively. The urinalysis is bland, and renal sonogram is normal. He isstarted on IV ceftriaxone 2gm daily and IV 25% salt-pooralbumin.ACLF Guidelines to practiceAJG 202215Case‐ 48 hours later Still disoriented despite ceftriaxone for 48 hours, with newonset-shortness of breath. Creatinine is now 3.0mg/dL, sodium 130 mEq/L, bilirubin 3.5mg/dL and INR 1.8. A repeat tap shows a 25% reduction in PMNs. Blood andascitic fluid cultures from the ER are negative. IV norepinephrine is initiated (since terlipressin is not currentlyavailable in the US). Antibiotics are escalated to meropenemand vancomycin since the ascites PMNs have not decreasedby 25%.ACLF Guidelines to practiceAJG 202216American College of Gastroenterology8
8/17/2022Case‐ Next Morning Tachypneic and hypoxic (SpO2: 91%) with a new RLLinfiltrate Obtunded, anuric with a MAP of 45mmHg. He is transferredto the ICU with a serum creatinine of 4.8 mg/dL and WBCcount of 15000/mL. Discussions regarding intubation, renal replacement therapy(RRT), and pressor support are undertaken with his wife.Since he now requires organ support to maintain perfusion,oxygenation, and is obtunded, he is a suboptimal candidatefor liver transplantation Ultimately the patient passes away without liver transplant.ACLF Guidelines to practiceAJG 202217Dominoes fall rapidly if precipitants for ACLF are not recognized early18American College of Gastroenterology9
8/17/2022Pathogenesis and Definitions19Gut‐liver changes andimmune dysfunctionAlbillos et al J Hep 2020, Bajaj et alNEJM 202120American College of Gastroenterology10
8/17/2022Acute liver failure vs ACLFJaundiceAscitesVariceal bleedingHepaticencephalopathyNo liver diseasePrecipitants1. Drugs2. Viral hepatitis3. Autoimmune4. WilsonHepatic icliver disease( SurgeryIdiopathicCompensatedcirrhosisType AACLFDecompensated cirrhosisType BACLFType CACLFHepatic and extrahepaticorgan failuresJalan R et al ACLF WGO Consensus Gastroenterology 201421APASL ACLF ResearchConsortiumEASL CLIF‐C ACLFNACSELDTotal BilirubinPT/INRTotal alysisDialysisBrainHE gradeHE gradeHE grade III/IVCirculatoryLactateMAP, vasopressorsMAP, vasopressorsRespiratory‐‐PaO2 or SpO2 / FiO2Mechanical ventilationPredominantly Hepaticfailure variablesCombination of hepatic andextrahepatic organ failurevariablesPredominantly extra‐hepaticorgan failure variablesOrganLiverMajorOrgan failureCategoryIssuesDiagnosis can be made early Diagnosis of ACLF may beenough for intervention tomade too late to impactalter disease course.disease outcome.Sensitive but not specific forearly mortalityDiagnosis of ACLF may be madetoo late to impact diseaseoutcome.22American College of Gastroenterology11
8/17/2022ACG ACLF definitionACLF is a potentially reversible condition in patientswith chronic liver disease with or without cirrhosisthat is associated with the potential for multipleorgan failure and mortality within 3 months in theabsence of treatment of the underlying liver disease,liver support, or liver transplantationBajaj JS et al ACG ACLF Guidelines 202123ACG Guideline Concept Statements1. In patients with cirrhosis who are hospitalized, the NACSELD score is likelyassociated with futility while the EASL‐CLIF SOFA score is associated with28‐day prognostication.2. None of the three society definitions is optimal for informing managementchange.3. Prognostic markers that predict ACLF outcome should be separate fromdiagnostic markers that confirm the presence of ACLF.4. Microbial composition and microbial‐origin metabolites can be used asbiomarkers for ACLF development and prognosis with further validation.Bajaj JS et al ACG ACLF Guidelines 202124American College of Gastroenterology12
8/17/2022Individual Organ Failures25Brain Failure or Acute Encephalopathy: Mostly HE Stabilize airway, BP Triage appropriately Lab work IV fluids, NG ,antibiotics empiricallyif indicated Lactulose either PO orvia NG or via enemasdepending onmentation Other therapies for HEimprovement Drug screen Psychiatric disorders Neurological disorders Delirium on dementia InfectionsInitiategeneral careEvaluate foralternativesCommenceempiricaltherapy forHEIdentifyprecipitatingfactors andreverse Infections GI bleeding Electrolyte disorder Diuretic overdose UnidentifiedAcharya et al Am J Gastro 201826American College of Gastroenterology13
8/17/2022HyperammonemiaAlcohol intoxicationAlcohol withdrawalSepsisMedications forsleep and pain In ACLF, use of short‐acting dexmedetomidinefor sedation vs otheragents to shorten time toextubation. In ventilated patients, wesuggest againstprophylactic antibiotics toreduce mortality orduration of mechanicalventilationReade et al NEJM 2015ACG ACLF Guidelines 202127AKI Definition Increase in sCr 0.3 mg/dl 48 hours or 50% increase from baselineAKIStage 1: Increase in sCr 0.3 mg/dl in 48 hoursStagingOR Increase in sCr 1.5‐2.0 times from baselineStage 2: Increase in sCr 2.0‐3.0 times from baselineStage 3: Increase in sCr 3.0 times from baseline ORSerum creatinine 4.0mg/dl with an acute increase of 0.3 mg/dlORInitiation of renal replacement therapyHRS‐AKIDiagnostic ‐Cirrhosis and ascites;‐Stage 2 or 3 AKI;Criteria‐No improvement of serum creatinine (decrease of creatinine 0.3mg/dl ofbaseline) after at least 48 hours of diuretic withdrawal and volume expansionwith albumin (1 g/kg body weight/day for 2 days);‐Absence of hypovolemic shock or severe infection requiring vasoactive drugs tomaintain arterial pressure;‐No current or recent treatment with nephrotoxic drugs;‐Proteinuria 500 mg/day and no microhematuria ( 50 RBCs/ml).28American College of Gastroenterology14
8/17/2022Terlipressin increases HRS reversalTerlipressin (N 199)Verified HRS Reversal (%)Placebo (N 101)p 0.01250403029.1%2015.8%100n 58n 16 No overall survival benefit but trend for improved RRT‐free survival and significant improvement in post‐OLTsurvival Serum creatinine 5 mg/dl associated with low response and increased deaths (70 vs 47%) with terlipressin Reduced need for RRT with terlipressinWong et al, NEJM 2021291.In AKI stage 2 & 3 acute kidneyinjury (AKI), we suggest IValbumin and vasoconstrictors vsalbumin alone2.In hospitalized patients HRS‐AKIwithout high grade of ACLF ormajor cardiopulmonary orvascular disease, we suggestterlipressin or norepinephrineto improve renal function.Wong et al 2016, Wong et al NEJM 202130American College of Gastroenterology15
8/17/2022Coagulation Failure: INR is not the be‐all and end‐all1. In ACLF, we suggest against INRto measure coagulation risk2. In patients with ACLF and alteredcoagulation parameters, wesuggest against transfusion in theabsence of bleeding or a plannedprocedure.3. In patients who require invasiveprocedures, we recommend theuse of Thrombo-elastography(TEG) or rotational TEG(ROTEM), vs INR, to accuratelyassess transfusion needs.Northup et al 2015, O’Leary et al 201931Precipitating Factors Infections Alcohol‐related Surgery (Mayo Clinic and Vocal Penn Score) Drug‐induced liver injury Viral hepatitis, including reactivation and flare32American College of Gastroenterology16
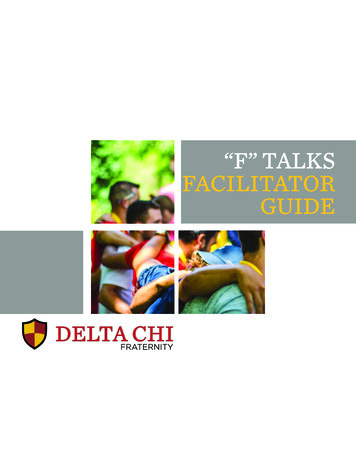
8/17/2022Infections lead to high mortality in cirrhosis30% die within 1 monthAdditional 30% die by 1 yearArvaniti V et al. Gastroenterology 2010; 139: 1246‐125633Clues that can indicate infections in cirrhosis Usual signs of infection may be absent due to impairedimmune response Other signs and symptoms could be relevant– Altered mental status or hepatic encephalopathy– Acute kidney injury– Asymptomatic patients with ascites can have “silent” SBP– Increase in WBC count may not be dramatic since cirrhotic patientshave a lower baseline34American College of Gastroenterology17
8/17/2022No Paracentesis with cell count Culture blood, ascitic fluid, urine Chest x‐ray Stool toxigenic C. difficile (if patient has 3unformed stools)Any of following criteria: MAP 65 mm Hg AND Lactate 2 mmol/L despitevolume resuscitation Oxygen saturation 90% Heart rate 40 130/min Respiratory rate 10 28/min Persistent decrease in level of consciousnessTransfer to ICU Pulmonary Infiltrate and respiratorysymptoms or Temperature 38⁰ c 36⁰ or WBC 10,000 mm‐3 or 4,000 mm‐3 or Rales or crepitationsAscites PMN 250mm‐3SBPPneumoniaCefotaxime 2 g Q8H IVWITH Albumin 1.5g/kg IV at diagnosisand 1 g/kg IV day 3Repeat paracentesis at48 hours to confirm PMN decreaseby 25%YesCommunityAcquiredUrinary symptoms &urine WBC 15/HPF orpositive urine gram stain orpositive urine cultureUrinary tract icile infectionBloodstreaminfectionNosocomialVancomycin 125 mgPO Q 6H for 10 daysAntibiotics**Clinical andradiologicalresolution 3 Unformed stool Toxigenic C difficile llinTazobactam 4.5g Q 6HNegative cultures &symptom resolutionBajaj JS et al NEJM 202135Timing of Antimicrobial Therapy: Impact on Survival36American College of Gastroenterology18
8/17/2022Inappropriate antibiotics increase mortalityOR 9.5 Risk factor: Multidrug resistance organismArabi YM et al. Hepatology, Accepted 201237Judicious use of albumin prevents mortality and AKI in SBP but not in otherinfections and not for all inpatientsSBPNon‐SBPPoca et al J Hepatol 2012, Sort et al N Engl J Med 1999, Thevenot et al J Hepatol 2014, China L et al NEJM 202138American College of Gastroenterology19
8/17/2022ACG ACLF Guideline Recommendations: Infections Check for infection in hospitalized patients. In suspected infection, we suggest early antibiotics In patients not responding to antibiotic therapy, we recommend suspicion ofa resistant organism or fungal infection In SBP albumin with antibiotics to prevent AKI and subsequent organ failuresbut not in other infections. In with prior SBP, we suggest use of antibiotics for secondary SBP prophylaxisto prevent recurrent SBP. In those needing primary SBP prophylaxis, we suggest daily prophylacticantibiotics, although no one specific regimen is superior to another, toprevent SBP We suggest avoiding PPI unless there is a clear indication39Therapeutic strategies General (airway, multi‐disciplinary team, nutrition,treating precipitating factors) Specific treatments (albumin, G‐CSF, Stem celltherapy) Liver‐assist devices (MARS, ELAD) Liver transplant (deceased or living donor)40American College of Gastroenterology20
8/17/2022If no resolution or conditionworsens after initial RxFamily Meeting/DecisionTransfer to ICU End of life careInvestigationsParacentesis, Culture blood, ascitic fluid,urine, Chest x‐rayTreat infectionVancomycin 15 mg/kg Q 6 HMeropenem 1 gram Q 8 HGeneral measuresMAP 60 mg HgMAP 60 HgPersistent shockEnteral nutrition is preferredFluid resuscitation within 3 hoursTherapeutic paracentesisAspiration precautionsDVT prophylaxisStress ulcer prophylaxisNorepinephrine Range:0.125 to 0.2 mcg/kg/minuteHydrocortisone 50 mg Q 6 hBajaj JS et al NEJM 202141Albumin in Inpatients with Cirrhosis: Not Helpful 777 inpatients across multiple UK CentersOpen‐label randomized trialAlbumin targeted to 3g/dl or standard of care for 14 daysPrimary Endpoint: new infection, kidney dysfunction,or death between days 3 and 15 after the initiation oftreatment.Results: No significant change but higher respiratoryfailure in albumin armACG Recommendations: We recommend againstdaily infusion of albumin to maintain albumin 3gm/dl to improve mortality, prevention of renaldysfunction or infectionChina et al NEJM 202142American College of Gastroenterology21
8/17/2022G‐CSF and effect on liver disease severity176 patients randomized 1:1Survival 34.1% vs 37.5% SMT, p 0.81Terminated early due to futiltyACG Recommendations: In ACLF, we suggest against the use of G‐CSF toimprove mortalityKedarisetty CK et al Gastro 2015, Engelmann et al J Hepatol 202143Should ACLF patients get extra listing priorityfor liver transplant?44American College of Gastroenterology22
8/17/2022OrganfailureArguments against prioritizingLiverKidneyEASL‐CLIFNACSELDBilirubin 12mg/dLN/ACreatinine 1.5 md/dL(or 2mg/dL)†Renal replacementtherapyData in UNOSregistry*Serum bilirubinSerum creatinineand dialysis in lastweek (yes/no)None, grade 1‐2,grade 3‐4Serum INRHE West Haven gradesHE West HavenIII/IVgrades III/IVCoagINR 2.5N/AMechanical ventilationRespiratiBiPAP or mechanicalOn ventilator PaO2/FiO2 200 oronventilation(yes/no)SpO2/FiO2 214Vasopressors MAP 60mmHg orInotropes (yes/no);CirculatiSBP reductionUse of vasopressorslife supporton 40mmHg otential for misclassification of UNOS data vs ACLF gradeUsing retrospective data to make prospective decisionsZero –sum game; non‐ACLF pts may be affectedCurrently there is low support to change listing and priority criteriaGoldberg & Bajaj Liver Transpl 2021, Bajaj & Verna Liver Transpl 202045Arguments for transplanting selected ACLF patients1. MELD may not capture thedisease severity2. Acceptable survival post‐LTfor ACLF‐2 and 33. Futility rules may need to bespecifiedTAM score:a. Age 53 years,b. arterial lactate 4 mmol/Lc. mechanical ventilation withPaO2/FiO2 200 mm Hg,d. leukocyte count 10 G/LJalan et al J Hepatol 2021, Artzner et al AJT 202046American College of Gastroenterology23
8/17/2022Transplant versus Futility for ACLF: ACG Guidelinerecommendations ACLF patients who continue to require mechanicalventilation due to ARDS or brain‐related conditionsdespite optimal therapy, we suggest against LT listing In patients with end‐stage liver disease admitted to thehospital, we suggest early goals of care discussion and ifappropriate, referral to palliative care to improveresource utilizationBajaj JS et al ACG ACLF Guidelines 202147Future Directions48American College of Gastroenterology24
8/17/2022What is needed in a biomarker for ACLF?(a) objective,(b) reliable,(c) specific to ACLF and distinct from AD and from otherpatients without cirrhosis requiring critical care,(d) easily translatable into clinical practice,(e) determine who is a good candidate for livertransplantation.Bajaj JS et al ACG ACLF Guidelines 202149Issues with current ACLF definitions & biomarkers Discordance as to underlying liver disease severity and precipitating factors Not prognostic but diagnostic because end-organ failures are likely related to death Need to be more pro-active rather than reactiveAcutedecompensationCirrhosisACLFPatients incritical carewithout liverdiseaseAcute liverfailure50American College of Gastroenterology25
8/17/2022Microbial‐origin Metabolites1. Differentiate between patients with/without ACLF2. Can independently predict who develops ACLFBajaj JS et al Gastroenterology 2020, Moreau et al J Hepatol 202051Back to the case: Opportunities missed thatcan snowball into ACLF52American College of Gastroenterology26
8/17/2022Cirrhosis or Chronic Liver DiseaseSuspect cirrhosis or chronic liverdisease in appropriate patientsClose watch on creatinine,mental status, respiratory statusand circulationEarly suspicion of infectionEarly paracentesis & culturesAppropriate antibiotics initiallyRe‐evaluate antibiotic therapyEarly transfer to preventaspiration pneumoniaHepatic andExtrahepaticOrgan failureORAcute on chronicLiver failure (ACLF)Diagnose precipitatingfactors earlyResuscitateTreat precipitating factorTreat infectionSupport failing organsAssess for ICU managementEarly consideration forLiver transplant eligibility‐Transplant candidate‐ Number of organ failuresNoACLF Guidelines topracticeAJG 2022Evaluate forpalliative andend of life carePrecipitating factors: Alcohol Viral hepatitis DILI Surgery Ischemia InfectionYesEvaluate forliver transplantEarly involvement of palliativecare, family and transplant team53Summary and Take‐Home Messages ACLF represents an increasingly large healthcare and economic burden in theUS with a high mortality Infections are one of the major reasons for ACLF, and their bacteriology ofinfections is changing radically. A high index of suspicion, flexible, rapid and appropriate antibiotics andprevention of acute kidney injury is required to prevent ACLF from infections Avoid unnecessary PPIs Need for systematic efforts to improve patient outcomes (risk factormodification, early diagnosis, effective treatment) Cost‐effective strategies towards higher recovery, less mortality are needed,especially in the context of liver transplant54American College of Gastroenterology27
8/17/20225555Acknowledgements: NACSELD PIs and coordinators56American College of Gastroenterology28
8/17/2022Questions and AnswersJasmohan S. Bajaj, MD, MS, FACGDavid E. Bernstein, MD, MACG57ACG 2021October 22‐27Las Vegas, NV58American College of Gastroenterology29
Surgery (Mayo Clinic and Vocal Penn Score) Drug‐induced liver injury Viral hepatitis, including reactivation and flare 31 32 American College of Gastroenterology . Arvaniti V et al. Gastroenterology 2010; 139: 1246‐1256 30% die within 1 month Additional 30% die by 1 year Clues that can indicate infections in cirrhosis Usual .