Transcription
CODING COMPANIONeGeneral Surgery/GastroenterologySamplA comprehensive illustrated guide to codingand reimbursement2 0 21optum360coding.com
ContentsmplGeneral Surgery and Gastroenterology Procedures andServices.1E/M Services . 1Skin . 22Pilonidal Cyst. 56Introduction . 57Repair . 64Destruction.110Breast .115General Musculoskeletal .141Neck.155Thorax .159Back .160Spine .163Abdomen/Musculoskeletal .164Humerus.166Forearm/Wrist .170Hands/Fingers.174Pelvis/Hip .176Femur/Knee.184Leg/Ankle.187Foot/Toes . 192Endoscopy. 194Respiratory . 195Arteries and Veins. 204Spleen. 271Lymph Nodes. 275Diaphragm . 303Esophagus . 306Stomach. 402Intestines . 452Meckel’s Diverticulum . 553Appendix . 556Rectum. 559Anus . 633Liver . 671Biliary Tract. 689Pancreas. 725Abdomen/Digestive . 742Reproductive . 809Thyroid . 810Parathyroid. 820Extracranial Nerves . 825Medicine . 831HCPCS. 845Appendix . 854eGetting Started with Coding Companion.iCPT Codes .iICD-10-CM.iDetailed Code Information .iAppendix Codes and Descriptions.iCCI Edit Updates .iIndex.iGeneral Guidelines .iCorrect Coding Initiative Update 25.3 . 871SaIndex . 891CPT 2020 American Medical Association. All Rights Reserved.Coding Companion for General Surgery/Gastroenterology 2020 Optum360, LLCContents — i
Getting Started with Coding CompanionThe book also allows coders to validate the intended code selectionby providing an easy-to-understand explanation of the procedureand associated conditions or indications for performing the variousprocedures. As a result, data quality and reimbursement will beimproved by providing code-specific clinical information andhelpful tips regarding the coding of procedures.CPT CodesFor ease of use, evaluation and management codes related toGeneral Surgery/Gastroenterology are listed first in the CodingCompanion. All other CPT codes in Coding Companion are listed inascending numeric order. Included in the code set are all surgery,radiology, laboratory, and medicine codes pertinent to the specialty.Each CPT code is followed by its official CPT code description.ICD-10-CMSaOverall, the 10th revision goes into greater clinical detail than didICD-9-CM and addresses information about previously classifieddiseases, as well as those diseases discovered since the last revision.Conditions are grouped with general epidemiological purposes andthe evaluation of health care in mind. New features have beenadded, and conditions have been reorganized, although the formatand conventions of the classification remain unchanged for themost part.Detailed Code InformationOne or more columns are dedicated to each procedure or service orto a series of similar procedures/services. Following the specific CPTcode and its narrative, is a combination of features. A sample isshown on page ii. The black boxes with numbers in themcorrespond to the information on the pages following the sample.Appendix Codes and DescriptionsSome CPT codes are presented in a less comprehensive format in theappendix. The CPT codes appropriate to the specialty are included inthe appendix with the official CPT code description. The codes arepresented in numeric order, and each code is followed by aneasy-to-understand lay description of the procedure.The codes in the appendix are presented in the following order: E/M ServicesCCI Edit UpdatesThe Coding Companion series includes the list of codes from theofficial Centers for Medicare and Medicaid Services’ National CorrectCoding Policy Manual for Part B Medicare Contractors that areconsidered to be an integral part of the comprehensive code ormutually exclusive of it and should not be reported separately. Thecodes in the Correct Coding Initiative (CCI) section are from themost current version available at press time. The CCI edits arelocated in a section at the back of the book. Optum360 maintains awebsite to accompany the Coding Companions series and postsupdated CCI edits on this website so that current information isavailable before the next edition. The website address is http://www.optum360coding.com/ProductUpdates/. The 2021 editionpassword is: XXXXXX. Please note that you should log in eachquarter to ensure you receive the most current updates. An emailreminder will also be sent to you to let you know when the updatesare available.IndexA comprehensive index is provided for easy access to the codes. Theindex entries have several axes. A code can be looked up by itsprocedural name or by the diagnoses commonly associated with it.Codes are also indexed anatomically. For example:mplResequencing of CPT CodesThe American Medical Association (AMA) employs a resequencednumbering methodology. According to the AMA, there are instanceswhere a new code is needed within an existing grouping of codes,but an unused code number is not available to keep the rangesequential. In the instance where the existing codes were notchanged or had only minimal changes, the AMA assigned a code outof numeric sequence with the other related codes being groupedtogether. The resequenced codes and their descriptions have beenplaced with their related codes, out of numeric sequence.CPT codes within the Optum360 Coding Companion series display intheir resequenced order. Resequenced codes are enclosed inbrackets for easy identification.Category II codes are not published in this book. Refer to the CPTbook for code descriptions.eCoding Companion for General Surgery/Gastroenterology is designedto be a guide to the specialty procedures classified in the CPT book.It is structured to help coders understand procedures and translatephysician narrative into correct CPT codes by combining manyclinical resources into one, easy-to-use source book.69501Transmastoid antrotomy (simple mastoidectomy)could be found in the index under the following main terms:AntrotomyTransmastoid, 69501ExcisionMastoidSimple, 69501General GuidelinesProvidersThe AMA advises coders that while a particular service or proceduremay be assigned to a specific section, it is not limited to use only bythat specialty group (see paragraphs two and three under“Instructions for Use of the CPT Codebook” on page xiii of the CPTBook). Additionally, the procedures and services listed throughoutthe book are for use by any qualified physician or other qualifiedhealth care professional or entity (e.g., hospitals, laboratories, orhome health agencies). Keep in mind that there may be otherpolicies or guidance that can affect who may report a specific service.SuppliesSome payers may allow physicians to separately report drugs andother supplies when reporting the place of service as office or othernonfacility setting. Drugs and supplies are to be reported by thefacility only when performed in a facility setting.Professional and Technical ComponentRadiology and some pathology codes often have a technical and aprofessional component. When physicians do not own their ownequipment and send their patients to outside testing facilities, theyshould append modifier 26 to the procedural code to indicate theyperformed only the professional component. Pathology and Laboratory Surgery Medicine Services Radiology Category IIICPT 2020 American Medical Association. All Rights Reserved.Coding Companion for General Surgery/Gastroenterology 2020 Optum360, LLCGetting Started with Coding Companion — i
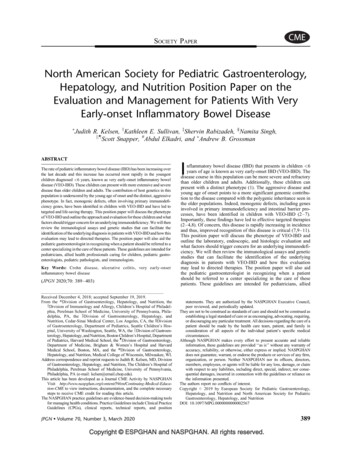
Relative Value Units/Medicare Edits11770-11772Non-Facility RVU11770 Excision of pilonidal cyst or sinus; 2Facility RVUNormal follicleStretched follicleInfected follicleAcute abscessChronic 361.615.3412.7416.68FUD Status MUEModifiers11770 10A1(3) 51 N/A N/A N/A11771 90A1(3) 51 N/A N/A N/A11772 90A1(3) 51 N/A N/A N/A* with documentationIOM ReferenceNoneepithelial tissue. Cells arranged in sheets that cover internal and externalbody surfaces that can absorb, protect, and/or secrete and includes theprotective covering for external surfaces (skin), absorptive linings for internalsurfaces such as the intestine, and secreting structures such as salivary orsweat glands.mplA pilonidal cyst or sinus is entrapped epithelial tissue located in thesacrococcygeal region above the buttocks. These lesions are usually associatedwith ingrown hair. A sinus cavity is present and may have a fluid-producingcystic lining. With a small or simple sinus in 11770, the physician uses a scalpelto completely excise the involved tissue. The wound is sutured in a singlelayer. In 11771, an extensive sinus is present superficial to the fascia overlyingthe sacrum but with subcutaneous extensions. The physician uses a scalpelto completely excise the cystic tissue. The wound may be sutured in severallayers. In 11772, the sinus involves many subcutaneous extensions superficialto the fascia overlying the sacrum. The physician uses a scalpel to completelyexcise the cystic tissue. Local soft tissue flaps (i.e., Z-plasty, Y-V plasty,myofasciocutaneous flap) may be required for closure of a large defect or thewound may be left open to heal by granulation.Coding TipsClosure of the defect is included in this code and should not be reportedseparately. For incision and drainage of a pilonidal cyst, simple, see 10080;complicated, see 10081. Surgical trays, A4550, are not separately reimbursedby Medicare; however, other third-party payers may cover them. Check withthe specific payer to determine coverage.ICD-10-CM Diagnostic CodesPilonidal cyst with abscessPilonidal sinus with abscessPilonidal cyst without abscessPilonidal sinus without abscessAMA: 11772 2018,Jan,8; 2017,Jan,8; 2016,Jan,13; 2015,Sep,12 2020 Optum360, LLCTotaleExplanation56MPabscess. Circumscribed collection of pus resulting from bacteria, frequentlyassociated with swelling and other signs of inflammation.A pilonidal cyst is excisedL05.01L05.02L05.91L05.92PETerms To KnowPilonidal disordersSaPilonidal CystPilonidal cyst117701177111772Workl News Revised Add Onfascia. Fibrous sheet or band of tissue that envelops organs, muscles, andgroupings of muscles.lesion. Area of damaged tissue that has lost continuity or function, due todisease or trauma.pilonidal cyst. Sac or sinus cavity of trapped epithelial tissues in thesacrococcygeal region, usually associated with ingrown hair.pilonidal sinus. Fistula, tract, or channel that extends from an infected areaof ingrown hair to another site within the skin or out to the skin surface.subcutaneous tissue. Sheet or wide band of adipose (fat) and areolarconnective tissue in two layers attached to the dermis.wound repair. Surgical closure of a wound is divided into three categories:simple, intermediate, and complex. simple repair: Surgical closure of asuperficial wound, requiring single layer suturing of the skin epidermis, dermis,or subcutaneous tissue. intermediate repair: Surgical closure of a woundrequiring closure of one or more of the deeper subcutaneous tissue andnon-muscle fascia layers in addition to suturing the skin; contaminated woundswith single layer closure that need extensive cleaning or foreign body removal.complex repair: Repair of wounds requiring more than layered closure(debridement, scar revision, stents, retention sutures).z-plasty. Plastic surgery technique used primarily to release tension orelongate contractured scar tissue in which a Z-shaped incision is made withthe middle line of the Z crossing the area of greatest tension. The triangularflaps are then rotated so that they cross the incision line in the oppositedirection, creating a reversed Z.AMA: CPT Assist[Resequenced]S LateralityCPT 2020 American Medical Association. All Rights Reserved.Coding Companion for General Surgery/Gastroenterology
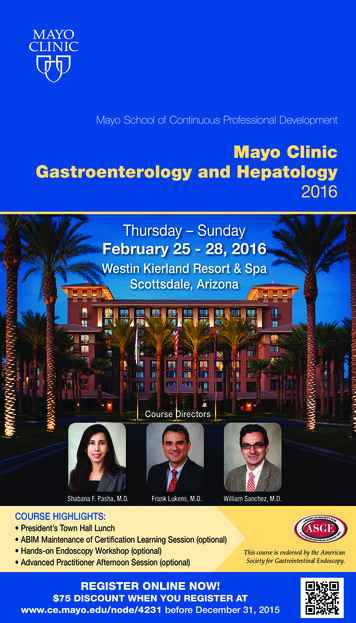
R22.221550Localized swelling, mass and lump, trunkAMA: 21550 2018,Sep,721550 Biopsy, soft tissue of neck or thoraxRelative Value Units/Medicare EditsNon-Facility RVUSkin, fat, andsubfascial tissues21550Facility 080.284.47FUD Status MUEPlatysma muscleTotalModifiers21550 10A2(3) 51 N/A N/A N/A* with documentationIOM ReferenceNoneTerms To KnowA soft tissue excisional biopsyof superficial tissues is takenbenign. Mild or nonmalignant in nature.biopsy. Tissue or fluid removed for diagnostic purposes through analysis ofthe cells in the biopsy material.ecarcinoma in situ. Malignancy that arises from the cells of the vessel, gland,or organ of origin that remains confined to that site or has not invadedneighboring tissue.The physician performs a biopsy of the soft tissues of the neck or thorax. Withproper anesthesia administered, the physician identifies the mass throughpalpation and x-ray (reported separately), if needed. An incision is made overthe site and dissection is taken down to the subcutaneous fat or further intothe fascia or muscle to reach the lesion. A portion of the tissue mass is excisedand submitted for pathology. The area is irrigated and the incision is closedwith layered sutures.Coding TipsSaA biopsy is not reported separately when followed by an excisional removalduring the same operative session. When 21550 is performed with anotherseparately identifiable procedure, the highest dollar value code is listed as theprimary procedure, and subsequent procedures are appended with modifier51. For a needle biopsy of muscle, see 20206. Surgical trays, A4550, are notseparately reimbursed by Medicare; however, other third-party payers maycover them. Check with the specific payer to determine coverage.ICD-10-CM Diagnostic D49.89L03.221L03.313R22.1Malignant neoplasm of connective and soft tissue of head, faceand neckMalignant neoplasm of connective and soft tissue of thoraxMalignant neoplasm of head, face and neckMalignant neoplasm of thoraxSecondary malignant neoplasm of other specified sitesCarcinoma in situ of other specified sitesBenign neoplasm of connective and other soft tissue of head,face and neckBenign neoplasm of connective and other soft tissue of thoraxNeoplasm of unspecified behavior of other specified sitesCellulitis of neckCellulitis of chest wallLocalized swelling, mass and lump, neck 2020 Optum360, LLC156malignant. Any condition tending to progress toward death, specifically aninvasive tumor with a loss of cellular differentiation that has the ability tospread or metastasize to other body areas.mplExplanationl News Revised Add OnAMA: CPT Assistneoplasm. New abnormal growth, tumor.secondary. Second in order of occurrence or importance, or appearing duringthe course of another disease or condition.soft tissue. Nonepithelial tissues outside of the skeleton that includessubcutaneous adipose tissue, fibrous tissue, fascia, muscles, blood and lymphvessels, and peripheral nervous system tissue.subcutaneous tissue. Sheet or wide band of adipose (fat) and areolarconnective tissue in two layers attached to the dermis.suture. Numerous stitching techniques employed in wound closure.buried suture. Continuous or interrupted suture placed under the skin for alayered closure.continuous suture. Running stitch with tension evenly distributed across asingle strand to provide a leakproof closure line.interrupted suture. Series of single stitches with tension isolated at eachstitch, in which all stitches are not affected if one becomes loose, and theisolated sutures cannot act as a wick to transport an infection.purse-string suture. Continuous suture placed around a tubular structureand tightened, to reduce or close the lumen.retention suture. Secondary stitching that bridges the primary suture,providing support for the primary repair; a plastic or rubber bolster may beplaced over the primary repair and under the retention sutures.[Resequenced]S LateralityCPT 2020 American Medical Association. All Rights Reserved.Coding Companion for General Surgery/Gastroenterology
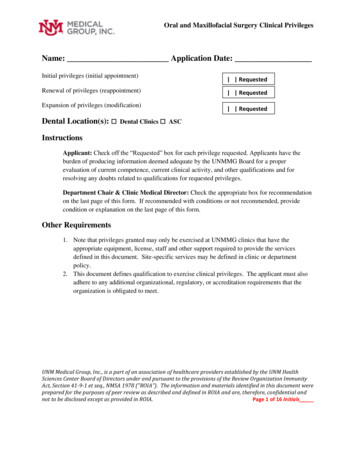
K76.5K76.6K76.893714037140 Venous anastomosis, open; portocavalHepatic veno-occlusive diseasePortal hypertensionOther specified diseases of liverAMA: 37140 2014,Jan,11Relative Value Units/Medicare EditsPortal veinNon-Facility RVU37140Inferior vena cavaFacility RVU37140L. renal veinR. renal 69.7467.7FUD Status MUESchematic of portocaval anatomyTotalModifiersIOM ReferenceNone37140 90A1(2) 51 N/A 62* N/A* with documentationTerms To KnowLigationeanastomosis. Surgically created connection between ducts, blood vessels,or bowel segments to allow flow from one to the other.ascites. Abnormal accumulation of free fluid in the abdominal cavity, causingdistention and tightness in addition to shortness of breath as the fluidaccumulates. Ascites is usually an underlying disorder and can be amanifestation of any number of diseases.ExplanationmplExample of an end-to-sideportocaval anastomosisSaCoding TipsWhen this code is performed with another separately identifiable procedure,the highest dollar value code is listed as the primary procedure and subsequentprocedures are appended with modifier 51. An open venous anastomosis,renoportal, is reported with code 37145. For TIPS (percutaneous) procedure,see 37182. For peritoneal-venous shunt, see 49425.ICD-10-CM Diagnostic .1K76.0K76.1K76.3Portal vein thrombosisBudd-Chiari syndromeSecondary esophageal varices with bleedingCompression of veinAlcoholic fatty liverAlcoholic cirrhosis of liver without ascitesAlcoholic cirrhosis of liver with ascitesOther cirrhosis of liverPhlebitis of portal veinFatty (change of) liver, not elsewhere classifiedChronic passive congestion of liverInfarction of liverCPT 2020 American Medical Association. All Rights Reserved.l NewCoding Companion for General Surgery/Gastroenterologybifurcated. Having two branches or divisions, such as the left pulmonaryveins that split off from the left atrium to carry oxygenated blood away fromthe heart.Budd-Chiari syndrome. Thrombus or other obstruction of the hepatic vein,with an enlarged liver, intractable ascites, portal hypertension, and the growthof extensive collateral vessels.hepatic portal vein. Blood vessel that delivers unoxygenated blood fromthe gastrointestinal tract, spleen, pancreas, and gallbladder to the liver.inferior. Located toward the feet or lower part of the body.ligation. Tying off a blood vessel or duct with a suture or a soft, thin wire.portal hypertension. Abnormally high blood pressure in the portal vein.thrombosis. Condition arising from the presence or formation of blood clotswithin a blood vessel that may cause vascular obstruction and insufficientoxygenation.thrombus. Stationary blood clot inside a blood vessel.varices. Enlarged, dilated, or twisted turning veins.vena cava. Main venous trunk that empties into the right atrium from boththe lower and upper regions, beginning at the junction of the common iliacveins inferiorly and the two brachiocephalic veins superiorly.s Revised Add OnAMA: CPT Assist[Resequenced]S Laterality 2020 Optum360, LLC255Arteries and VeinsThe physician performs portocaval venous anastomosis. The physician placesa long right thoracoabdominal incision and exposes the liver. The physicianexposes the inferior vena cava and portal vein through careful dissection. Thephysician places a plastic sling around the portal vein and ties it closed, justproximal to its bifurcation. The physician clamps and divides the portal vein.The physician applies a partial exclusion vascular clamp to the front of thevena cava and removes a small oval of tissue from the vena cava to allowend-to-side anastomosis of portal vein to the inferior vena cava. The physicianremoves the clamps and checks for appropriate flow without anastomoticleakage. The physician closes the incision, leaving a chest tube in place (butno abdominal drains, as this may lead to protein loss from postoperativedrainage of ascites).
25.4K25.5K25.643620 Gastrectomy, total; with esophagoenterostomy43621with Roux-en-Y reconstructionStomachis removedMalignant carcinoid tumor of the stomachBenign neoplasm of stomachNeoplasm of uncertain behavior of stomachBenign carcinoid tumor of the stomachNeoplasm of unspecified behavior of digestive systemAcute gastric ulcer with hemorrhageAcute gastric ulcer with perforationAcute gastric ulcer with both hemorrhage and perforationAcute gastric ulcer without hemorrhage or perforationChronic or unspecified gastric ulcer with hemorrhageChronic or unspecified gastric ulcer with perforationChronic or unspecified gastric ulcer with both hemorrhage andperforationChronic gastric ulcer without hemorrhage or perforationAcute peptic ulcer, site unspecified, with hemorrhageAcute peptic ulcer, site unspecified, with perforationAcute peptic ulcer, site unspecified, with both hemorrhage andperforationAcute peptic ulcer, site unspecified, without hemorrhage orperforationChronic or unspecified peptic ulcer, site unspecified, withhemorrhageChronic or unspecified peptic ulcer, site unspecified, withperforationChronic or unspecified peptic ulcer, site unspecified, with bothhemorrhage and perforationChronic peptic ulcer, site unspecified, without hemorrhage orperforationPolyp of stomach and duodenumContusion of stomach, initial encounterLaceration of stomach, initial encounterOther injury of stomach, initial encounterK25.7K27.0K27.1K27.2DiaphragmThe body of the stomach is removed. Theremaining duodenum is mobilized upwardand anastomosed to the distal esophagusEsophaguseK27.3Roux-en-Ybowel sectionK27.4mplK27.5ExplanationK27.6The physician removes the stomach and approximates a limb of small bowelto the esophagus by performing an esophagoenterostomy in 43620 or aRoux-en-Y esophagojejunostomy in 43621. The physician makes a midlineabdominal incision. The stomach is dissected free of surrounding structuresand its blood supply is divided. The stomach is divided at the gastroesophagealjunction and at the gastroduodenal junction and removed. In 43620, theremaining duodenal end of the intestine is simply mobilized to the end of theesophagus and connected. In 43621, a measured limb of Roux, or limb of smallintestine, is created by dividing the upper jejunum. The distal part of the nowdivided upper jejunum, the limb in continuity with the ileum, is brought upand anastomosed to the esophagus. The proximal end of the divided jejunum,the segment containing the duodenum, must be connected back into thelimb of small bowel farther down from the esophageal anastomosis. Thismaintains continuity for the duodenal section, which was sealed upon removalof the stomach, but which is also receiving bile from the liver and gallbladderas well as pancreatic juice.SaStomach43620-43621Coding TipsFor total gastrectomy with formation of an intestinal pouch, any type, see43622. For partial distal gastrectomy, with gastroduodenostomy, see 43631;with gastrojejunostomy, see 43632; with Roux-en Y reconstruction, see 43633;with formation of a gastrointestinal pouch, see 43634.ICD-10-CM Diagnostic 32XAS36.33XAS36.39XAAMA: 436202014,Jan,11; 2013,Jan,11-12436212014,Jan,11; 2013,Jan,11-12Relative Value Units/Medicare EditsNon-Facility RVU4362043621Facility .3757.8966.22FUD Status MUEModifiers43620 90A1(2) 51 N/A 62* 8043621 90A1(2) 51 N/A 62* 80* with documentationIOM ReferenceNoneMalignant neoplasm of cardiaMalignant neoplasm of fundus of stomachMalignant neoplasm of body of stomachMalignant neoplasm of pyloric antrumMalignant neoplasm of pylorusMalignant neoplasm of overlapping sites of stomachSecondary malignant neoplasm of other digestive organs 2020 Optum360, LLC406K27.7l News Revised Add OnAMA: CPT Assist[Resequenced]S LateralityCPT 2020 American Medical Association. All Rights Reserved.Coding Companion for General Surgery/Gastroenterology
497044970 Laparoscopy, surgical, appendectomyTrocars deliversurgical instrumentsLaparoscope is insertednear the umbilicusAppendixOther acute appendicitis without perforation, with gangreneOther appendicitisHyperplasia of appendixAppendicular concretionsDiverticulum of appendixFistula of appendixOther specified diseases of appendixRight lower quadrant abdominal tendernessRight lower quadrant rebound abdominal tendernessAMA: 44970 2018,Jan,8; 2017,Jan,8; 2016,Jan,13; 2015,Mar,3; 2015,Jan,16;2014,Jan,11; 2013,Jan,11-12; 2013,Dec,3Relative Value Units/Medicare EditsNon-Facility RVUAscendingcolonIleum44970Facility PTotal9.455.822.2217.49eFree teniaFUD Status MUEAppendix and Mesoappendixappendicular artery44970 90A1(2) 51 N/A 62* with documentationExplanation80IOM ReferenceNoneTerms To KnowCoding Tipsappendicitis. Inflammation and infection of the appendix. In the acute stageof the disease, common symptoms include severe pain in the right lowerquadrant of the abdomen, nausea, and vomiting.mplThe physician performs a laparoscopic appendectomy. The physician placesa trocar at the umbilicus and insufflates the abdomen. The laparoscope isplaced through the umbilical port and additional trocars are placed into theabdominal cavity. The appendix is identified, dissected from surroundingstructures, and its blood supply divided. The appendix
Coding Companion for General Surgery/Gastroenterology Getting Started with Coding Companion — i Getting Started with Coding Companion Coding Companion for General Surgery/Gastroenterology is designed to be a guide to the specialty procedures classified in the CPT book. It is structured to help coders understand procedures and translate