Transcription
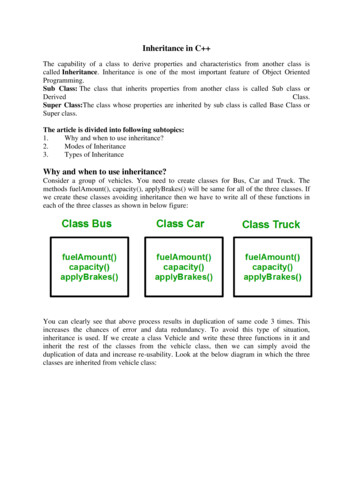
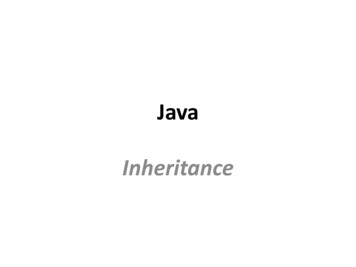
Mechanisms of InheritanceCONTENTSMENDELIAN INHERITANCEAutosomal Dominant InheritanceAutosomal Recessive InheritanceX-Linked Recessive InheritanceX-Linked Dominant InheritancePenetrance and ExpressivityLate-Acting GenesNONMENDELIAN INHERITANCETriplet RepeatsGenomic ImprintingMosaicismMitochondrial InheritanceMULTIFACTORIAL INHERITANCEPhenotypic DistributionLiability and RiskRisk and SeverityGender DifferencesEnvironmental FactorsCharacteristics of Multifactorial InheritanceOne of the most remarkable characteristics of chromosomesis the ability to sort precisely the genetic material representedin homologous pairs of chromosomes into daughter cells andgametes, as previously discussed. This assortment is recognizedthrough the many visible characteristics of individuals. Thisphenotype, or visible presentation of a person, is influencedby the expression of alleles at different times during development, at different efficiencies, and in different cells ortissues. Observed differences are the result of a cell’s genotype,or molecular variation in alleles.Mechanisms of inheritance generally refer to traits resultingfrom a single factor or gene, called unifactorial inheritance,or from the interaction of multiple factors or genes, calledmultifactorial inheritance. Because it is the simplest inheritance pattern, unifactorial inheritance is the best understood.Gregor Mendel first investigated this type of inheritance inhis famous studies of garden peas in 1865. Because theunderlying principles of Mendel’s work became hallmarks tounderstanding inheritance, mechanisms of unifactorial inheritance are often called mendelian inheritance and the othermechanisms are referred to as nonmendelian inheritance.3Multifactorial inheritance is more complex because of thevariation of traits within families and populations. Individualgenes within a disease demonstrating multifactorial inheritancemay have a dominant or recessive inheritance pattern; but whennumerous nongenetic factors and genes interact to cause thedisease, the mechanisms can be difficult to interpret and explain. MENDELIAN INHERITANCEGenes are found on autosomes and sex chromosomes, andevidence for the existence of genes prior to the molecularrevolution was based on measurable changes in phenotype.These changes resulted from allelic variation. Observingvariation depends on the relationship of one allele to another.The terms used to describe this relationship are dominant andrecessive. If only one allele of a pair is required to manifest aphenotype, the allele is dominant. If both alleles must be thesame for a particular phenotypic expression, the allele isrecessive. This is described by the notation AA, Aa, aa, where“A” is dominant and “a” is recessive. The AA condition iscalled homozygous dominant, Aa is called heterozygous, andaa is called homozygous recessive.Sex chromosomes also have alleles with dominant andrecessive expression. However, this situation is differentbecause for males all X chromosome genes are expressedfrom the same single chromosome. Females have two Xchromosomes, but the scenario is different from that ofautosomes because of lyonization.Variation in alleles results from mutations. The effects ofany mutation may influence the character and function of theprotein formed. Many times the mutation will create a proteinwith a recessive nature, but this is not always the case. Severalmechanisms through which an allele can affect a function areshown in Table 3-1. These mechanisms are independent ofmode of inheritance.Autosomal Dominant InheritanceMendelian inheritance is classified as autosomal dominant,autosomal recessive, and X-linked (Box 3-1). A diagram representing family relationships is called a pedigree and can beinformative about inherited characteristics. Figure 3-1 showsconventional symbols used in pedigree construction.The family pedigree shown in Figure 3-2 has featuressuggesting autosomal dominant inheritance. It can be noted
28MECHANISMS OF INHERITANCETABLE 3-1. Selected Mechanisms of Allele ActionBox 3-1. EXAMPLES OF elianAutosomal dominantAchondroplasiaMarfan syndromeNeurofibromatosis type 1BrachydactylyNoonan syndromeAutosomal recessiveAlbinismCystic ridosesX-linked dominantHypophosphatemic ricketsOrofaciodigital syndromeX-linked recessiveDuchenne/Becker musculardystrophiesHemophilia A and BGlucose-6-phosphatedehydrogenase deficiencyLesch-Nyhan syndromeTriplet repeatsFragile X syndromeMyotonic dystrophySpinocerebellar ataxiaFriedreich ataxiaSynpolydactylyGenomic imprintingPrader-Willi syndromeAngelman Gene product oractivity is reduced.Waardenburg syndromeresults from mutations inPAX3, a DNA bindingprotein important inregulating embryonicdevelopment.Gain-offunctionGene product isincreased.Gene expressionoccurs at the wrongplace or time.Charcot-Marie-Toothdisease results from theoverexpression of PMP22(peripheral myelin protein)caused by geneduplication.Gene product hasincreased activity.ProteinalterationNormal proteinfunction isdisrupted.Kennedy disease resultsfrom CAG (polyglutamine)expansion at the 5 endof the androgen receptor.The mutant proteinmisfolds, aggregates, andinteracts abnormally withother proteins, leading totoxic gain of function andalteration of normalfunction.Dominanteffects ofrecessivemutationAlleles arerecessive at themolecular level butshow a dominantmode ofinheritance.Retinoblastoma isinherited as a recessiveallele. A mutation in thesecond, normal allele(also known as the twohit hypothesis) results intumor formation.that each affected person has at least one affected parent.Moreover, the normal children of an affected parent, whenthey in turn marry normal persons, have only normaloffspring. In this particular instance, the mutant allele isdominant and the normal allele is recessive. In nearly allinstances of dominant inheritance, as exemplified by thepedigree, one parent carries the detrimental allele and showsthe anomaly, whereas the other parent is normal. The affectedparent will pass on the defective dominant allele, on average,to 50% of the children. Normal children do not carry theharmful dominant allele, hence their offspring and furtherdescendants are not burdened with the dominant trait.There are numerous examples in humans of defective genesthat are transmitted in a dominant pattern. Achondroplasia,a form of dwarfism, is inherited as an autosomal dominanttrait. Achondroplasia is a congenital disorder, a defect presentat birth. Affected individuals are small and disproportionate,with particularly short arms and legs. With an estimatedfrequency of 1 in 15,000 to 40,000 live births, achondroplasiais one of the more common mendelian disorders. Most infantsaffected by achondroplasia with two mutated alleles, repre-senting a homozygous condition, are stillborn or die ininfancy; heterozygous individuals surviving to adulthoodproduce fewer offspring than normal. This observation underscores an important point for many autosomal dominantdisorders—two mutated alleles often have severe clinicalconsequences.Characteristics of Autosomal DominantInheritanceGuidelines for recognizing autosomal dominant inheritancein humans may be summarized as follows:1. The affected offspring has one affected parent, unless thegene for the abnormal effect was the result of a newmutation.2. Unaffected persons do not transmit the trait to theirchildren.3. Males and females are equally likely to have or totransmit the trait to males and females.4. The trait is expected in every generation.5. The presence of two mutant alleles generally presentswith a more severe phenotype. Detrimental dominanttraits are rarely observed in the homozygous state.Autosomal Recessive InheritanceA gene can exist in at least two allelic forms. For the sake ofsimplicity, two will be considered—A and its alternative(mutant) allele, a. From these two alleles, there are three
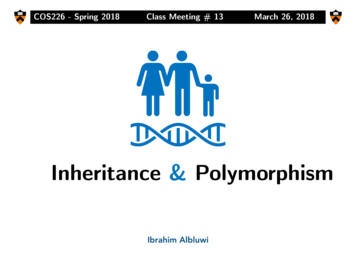
MENDELIAN INHERITANCENormal femaleMatingNormal maleConsanguineous matingUnknown sex, normalDizygotic twins (two eggs)Affected femaleAffected maleMonozygotic twins (one egg)Affected child of unknown sexMale heterozygote (carrier of recessive allele)Proband or propositus/propositaFemale heterozygote (carrier of recessive allele)I, IIRoman numerals designate generation number1, 2Arabic numerals designate individualswithin generationsSpontaneous abortion or stillbirthDeceasedFigure 3-1. Conventional symbols used in pedigrees.I12II1234567III1234567891011121314Figure 3-2. Pedigree of a family with an autosomal dominant trait.different genotypes, AA, Aa, and aa, that can be arrangedin six types of marriages. These genotypes and theiroffspring are listed in Table 3-2. The outcome of each type ofmarriage follows the mendelian principles of segregationand recombination.In the vast majority of cases of recessive inheritance,affected persons derive from marriages of two heterozygouscarriers; affected individuals receive a mutant allele fromeach parent and represent homozygous recessive expression.In other words, recessive disorders in family histories tend toappear only among siblings and not in their parents. This isdemonstrated by the family pedigree in Figure 3-3. Thispedigree shows that a normal male marries a normal woman.Apparently, both were heterozygous carriers, since one of thefour children (the first child, designated II-1) exhibited therecessive trait. This son, although affected, had two normaloffspring (III-1 and III-2). These two children must be carriers(Aa), having received the a allele from their father (II-1) andthe A allele from their unaffected mother (II-2). The geneticconstitution of the mother (II-2) cannot be ascertained; shemay be either homozygous dominant (AA) or a heterozygouscarrier (Aa). The marriage of first cousins (III-3 and III-4)increases the risk that both parents of IV-1 and IV-3 havereceived the same detrimental recessive gene through acommon ancestor. In this case, the common ancestors are theparents in generation I.It can be deduced from this pedigree that the daughter(II-6) of the first marriage was a carrier (Aa). Her two childrenwere normal, but it is noted that her first child (III-4) marrieda first cousin (III-3), and from this marriage affected children(IV-1 and IV-3) were born. Accordingly, the daughter of thethird generation (III-4) must have been heterozygous, and inturn, her mother (II-6) was most likely heterozygous (or elseshe married a heterozygous man). Similarly, the male involvedin the cousin marriage (III-3) must have been heterozygous,as was his father (II-3).29
30MECHANISMS OF INHERITANCETABLE 3-2. Possible Combinations of Genotypes and Phenotypes in Parents and the Possible Resulting OffspringGametesMating TypeFirst ParentSecond pePhenotypeAA x AANormal x normalAAAA100% AA100% NormalAA x AaNormal x normalAAAa50% AA50% Aa100% NormalAa x AaNormal x normalAaAa25% AA50% Aa25% aaAA x aaNormal x abnormalAAaa100% AaAa x aaNormal x abnormalAaaa50% Aa50% aa50% Normal50% Abnormalaa x aaAbnormal x abnormalaaaa100% aa100% Abnormal75% Normal25% Abnormal100% NormalFigure 3-3. Pedigree of a family with anautosomal recessive trait.I12II121234567III3456345IV12Pedigrees of the above kind typify the inheritance of suchrecessively determined traits in humans as albinism, cysticfibrosis, and phenylketonuria. Special significance is attachedto the heterozygous carrier—the individual who unknowinglycarries the recessive allele. It is usually difficult to tell, priorto marriage, whether the individual bears a detrimentalrecessive allele. Thus, a recessive allele may be transmittedwithout any outward manifestation for several generations,continually being sheltered by the dominant normal allele.The recessive allele, however, becomes exposed when twocarrier parents happen to mate, as seen in Figure 3-3. Thisexplains cases in which a trait, absent for many generations,can suddenly appear without warning.Often only one member in a family is afflicted with aparticular disorder. In such an event, it would be an error tojump to the conclusion that the abnormality is not geneticsolely because there are no other cases in the family.Withouta positive family history, and sometimes the corroboration ofdiagnoses, the occurrence of a single afflicted individual mayrepresent a new, sporadic mutation.Characteristics of Autosomal RecessiveInheritanceGuidelines for recognizing autosomal recessive inheritancemay be summarized as follows:1. Most affected individuals are children of phenotypicallynormal parents.2. Often more than one child in a large sibship is affected.On average, one fourth of siblings are affected.3. Males and females are equally likely to be affected.4. Affected persons who marry normal persons tend to havephenotypically normal children. (The probability is greaterof marrying a normal homozygote than a heterozygote.)5. When a trait is exceedingly rare, the responsible allele ismost likely recessive if there is an undue proportion ofmarriages of close relatives among the parents of theaffected offspring.Consanguinity and Recessive InheritanceOffspring affected with a recessive disorder tend to arisemore often from consanguineous unions than from marriages
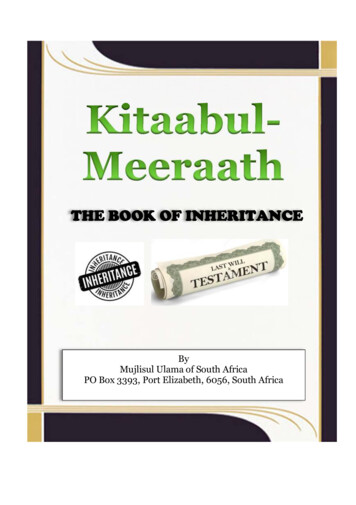
MENDELIAN INHERITANCEof unrelated persons (see Chapter 12). Close relatives sharemore of the same alleles than persons from the at-largepopulation. If a recessive trait is extremely rare, the chance isvery small that unrelated marriage partners would harbor thesame defective allele. The marriage of close relatives, however,increases the risk that both partners have received the samedefective allele through some common ancestor. Not all allelesare equally detrimental. Stated in another way, identical allelesmay produce an extreme phenotype, whereas two differentalleles of the same gene may appear mild or even normal.With increasing rarity of a recessive allele, it becomesincreasingly unlikely that unrelated parents will carry thesame recessive allele. With an exceedingly rare recessivedisorder, the expectation is that most affected children willcome from cousin marriages. Thus, the finding that theparents of Toulouse-Lautrec, a postimpressionist artist whodocumented bohemian nightlife, particularly at the MoulinRouge in Paris, were first cousins is the basis for the currentview that the French painter was afflicted with pycnodysostosis, characterized by short stature and a narrow lower jaw.This condition is governed by a rare recessive allele unlikeachondroplasia, another form of short stature that isdetermined by a dominant allele.Thus, it was more likely thatToulouse-Lautrec suffered a rare disorder expressed as aresult of his parents’ relatedness rather than a commondisorder that could only be explained by a new mutation.Codominant ExpressionIn some heterozygous conditions, both the dominant andrecessive allele phenotypes are expressed. From a molecularviewpoint, the relationship between the normal allele and themutant allele is best described as codominant. This meansthat, at the molecular level, neither allele masks the expression of the other. An example of codominance is sickle cellanemia. In this example, two types of hemoglobin are produced:normal type hemoglobin A and a mutant form, called hemoglobin S. Another example is the expression of both A and Bantigens on the surface of red blood cells in individuals withtype AB blood.The terms dominant and recessive have little, if any, utilitywhen both gene products affect the phenotype. Dominanceand recessiveness are attributes of the trait, or phenotype,not of the gene. An allele is not intrinsically dominant orrecessive—only normal or mutant.X-Linked Recessive InheritanceNo special characteristics of the X chromosome distinguish itfrom an autosome other than size and the genes found on thechromosome, but these features distinguish all chromosomesfrom each other. X chromosome inheritance, often called Xlinked or sex-linked, is remarkable because there is only one Xchromosome in males. Most of these alleles are thereforehemizygous, or present in only one copy, in the male becausethere is no corresponding homologous allele on the Ychromosome. Presence of a mutant allele on the X chromosome in a male is expressed, whereas in the female a singleBIOCHEMISTRY & PHYSIOLOGYHemoglobinHemoglobin is composed of heme, which mediates oxygenbinding, and globin, which surrounds and protects the heme.Hemoglobin is a tetramer of globin chains (two α-chains andtwo β-chains in adults), each associated with a heme. Thereare many variants of hemoglobin. In sickle cell, the β-globinchain is a mutation and is known as hemoglobin S (HbS). Amissense mutation causes valine to be placed in the protein inplace of glutamic acid.The mutation that causes HbS produces oxygenatedhemoglobin that has normal solubility; however, deoxygenatedhemoglobin is only about half as soluble as normal HbA. Inthis low-oxygen environment, HbS molecules crystallize intolong fibers, causing the characteristic sickling deformation ofthe cell. The deformed cells, which can disrupt blood flow, areresponsible for the symptoms associated with sickling crisessuch as pain, renal dysfunction, retinal bleeding, and asepticnecrosis of bone, and patients are at an increased risk foranemia owing to hemolysis of the sickled cells.IMMUNOLOGYABO Blood GroupsThere are 25 blood group systems that account for more than250 antigens on the surface of red blood cells. The ABO bloodgroup is one of the most important, and the antigensexpressed are produced from alleles of one gene. There arethree major alleles—A, B, and O—but more than 80 have beendescribed.The ABO gene encodes glycosyltransferases, which transferspecific sugars to a precursor protein known as the H antigen.The H antigen is a glycosphingolipid consisting of galactose,N-acetylglucosamine, galactose, and fructose attached to aceramide. In the absence of sialic acid, it is a globosiderather than a ganglioside. The A allele encodes α1,3-N-acetylgalactosamyl transferase, which addsN-acetylgalactosamine to the H antigen to form the A antigen.The B allele produces α1,3-galactosyltransferase, whichtransfers galactose to the H antigen, thus forming the Bantigen. The O allele produces the H antigen, but it has noenzyme activity.mutant allele may have a corresponding normal allele tomask its effects, as expected in the situation of dominanceversus recessiveness.The special features of X-linked recessive inheritance areseen in the transmission of hemophilia A (Fig. 3-4). This is ablood disorder in which a vital clotting factor (factor VIII) islacking, causing abnormally delayed clotting. Hemophiliaexists almost exclusively in males, who receive the detrimental mutant allele from their unaffected mothers. Figure3-4 shows part of the pedigree of Queen Victoria of England.Queen Victoria (I-2) was a carrier of the mutant allele that31
32MECHANISMS OF INHERITANCEFigure 3-4. X-linked inheritance ofhemophilia A among descendants ofQueen Victoria (I-2) of 0V12occurred either as a spontaneous mutation in her germline orwas a mutation in the sperm of her father, Edward Augustus,Duke of Kent. Queen Victoria had one son (II-9) withhemophilia and two daughters (II-3 and II-10) who werecarriers.The result of these children marrying into royal families in other countries spread the mutant factor VIII allele toSpain, Russia, and Germany. The children of II-3 have hemophilia in two more generations (III-7, IV-3, IV-5, and IV-10).The families of II-9 and II-10 also revealed hemophiliathrough two more generations (not shown). Though thegrandson of III-2 married V-1, no hemophilia allele wasintroduced back into the family of the first son of QueenVictoria, Edward VII, and the royal family of England hasremained free of hemophilia. Generation V is represented byQueen Elizabeth and Prince Philip.For alleles on the X chromosome, each son of a carriermother has a 50% chance of being affected by hemophilia,and each daughter has a 50% chance of being a carrier.Hemophilic females are exceedingly rare, since they can onlyderive from an extremely remote mating between a hemophilic man and a carrier woman. A few hemophilic womenhave been recorded in the medical literature; some havemarried and given birth to hemophilic sons.Characteristics of X-Linked Recessive InheritanceGuidelines for recognizing X-linked recessive inheritancemay be summarized as follows:1. Unaffected males do not transmit the disorder.2. All the daughters of an affected male are heterozygouscarriers.3. Heterozygous women transmit the mutant allele to 50%of the sons (who are affected) and to 50% of thedaughters (who are heterozygous carriers).4. If an affected male marries a heterozygous woman, halftheir sons will be affected, giving the erroneous impressionof male-to-male transmission.X-Linked Inheritance and GenderAs noted, X-linked inheritance is distinguished by thepresence of one chromosome in males but two in females. Toexplain the appearance of a condensed body in female cells,known as a Barr body, and to justify the possibility of twiceas many X chromosome gene products in females as in males,the Lyon hypothesis was proposed. This hypothesis, whichhas been become well established, recognizes the Barr bodyin female cells as an inactivated X chromosome. Throughinactivation, dosage compensation occurs in a female thatgenerally equalizes the expression between males and females.In general, lyonization suggests that (1) alleles found on thecondensed X chromosome are inactive, (2) inactivation occursvery early in development during the blastocyst stage, and(3) inactivation occurs randomly in each blastocyst cell.Lyonization is more complicated than this simplisticpresentation because some alleles are expressed only fromthe inactive X chromosome, other alleles escape inactivationand are expressed from both X chromosomes, and still otheralleles are variably expressed. It is easiest to understand Xinactivation as a random event, or that about 50% of cellshave the maternal X chromosome inactivated and about 50%of cells have the paternal X chromosome inactivated;however, this situation does not always occur. It is possible tohave skewed inactivation, whereby the X chromosome fromone parent is more or less likely to become inactivated.Depending on the degree of skewing, a clinical presentationwill be affected. The more extreme the skewing in favor ofkeeping the mutant X active, the poorer the prognosis for theindividual.The onset of X inactivation is controlled by the XIST gene.This gene is expressed only from the inactive X chromosomeand is a key component of the X inactivation center (XIC)found at the proximal end of Xq. The cell recognizes thenumber of X chromosomes by the number of XICs in the cell.In the presence of two X chromosomes, XIST is activated and
MENDELIAN INHERITANCEFigure 3-5. Inheritance of an X-linked dominant trait. Note that daughters always inherit the trait from an affected father whereassons of an affected father never inherit the trait.RNA molecules are produced that bind to regions of the Xchromosome, rendering it inactive. It is not known how somegenes escape the influence of the RNA molecules and remainactive.X-Linked Dominant InheritanceDisorders resulting from X-linked dominant inheritanceoccur far less frequently than other forms of inheritance. Asnoted, X-linked recessive inheritance can occur, and malesare almost always the affected gender although in very rarecases it is possible for females to acquire two mutant allelesor express milder phenotypes as carriers. With X-linkeddominant inheritance, there are no carriers; expression of thedisease occurs in both males and females, and only onemutant allele is required.As might be expected, heterozygousfemales may be less affected than males because of thepresence of a normal, nonmutated allele. The distinguishingfeature between an X-linked dominant and an autosomaldisorder is that an autosomal mutation is transmitted frommales and females to male and female offspring. When amutation is located on the X chromosome and expressed in adominant manner, females transmit the mutant allele to bothmale and female offspring; however, males can only transmitit to females (Fig. 3-5). In addition, affected females may onlytransmit the mutant allele to 50% of offspring; males willtransmit the mutant allele to 100% of females.phenotype is present (penetrant) or not (nonpenetrant) inthat one individual. In penetrant individuals, there may bemarked variability in the clinical manifestations of thedisorder. When more than one individual is considered, suchas a population of individuals, a percentage is usually appliedto the proportion of individuals likely to express aphenotype. To illustrate this point, if a trait occurs with 80%penetrance, expression is expected in 80% of individualswith the trait.Nonpenetrance is a cul-de-sac for clinicians and geneticcounselors. Figure 3-6 demonstrates a pedigree with anautosomal dominant trait in which nonpenetrance ispervasive. Individual II-2 most likely carries the diseaseallele, unless offspring III-2 arose from a new dominantmutation.The future offspring III-4 is at risk for the dominantdisease. The calculated mathematical risk would take intoconsideration the empirical penetrance percentage for thetrait (say, 60%) and the probability that a person from thegeneral population (spouse II-6) would harbor the diseaseallele.Expressivity is the term used to refer to the range ofphenotypes expressed by a specific genotype. This is muchmore frequent than nonpenetrance. A good example ofexpressivity is seen in neurofibromatosis (NF). NF consists oftwo disorders, NF1 and NF2, caused by mutations in differentgenes. NF is an autosomal dominant disorder, and in bothPenetrance and ExpressivityNot every person with the same mutant allele necessarilymanifests the disorder. When the trait in question does notappear in some individuals with the same genotype, the termpenetrance is applied. Penetrance has a precise meaning—namely, the percentage of individuals of a specific genotypeshowing the expected phenotype. If the phenotype is alwaysexpressed whenever the responsible allele is present, the traitis fully penetrant. If the phenotype is present only in someindividuals having the requisite genotype, the alleleexpressing the trait is incompletely penetrant. For a givenindividual, penetrance is an all-or-none phenomenon; i.e., theI1234II121256III34Figure 3-6. Nonpenetrance in a family with an autosomaldominant disorder. The light-colored boxes indicate individualswho do not express the phenotype for the disorder.33
34MECHANISMS OF INHERITANCEforms over 95% of affected individuals have café-au-laitspots. Café-au-lait spots are flat, coffee-colored macules. Theexpressivity of these spots, which resemble birthmarks, isvariable and differs in number, shape, size, and positionamong individuals.Late-Acting GenesProper interpretation of penetrance and expressivity may becomplicated when the genes involved are expressed in theadult rather than the child. These late-acting genes includemany genes involved with aging but may also include certaindisease genes. Huntington disease is an inherited disordercharacterized by uncontrollable swaying movements of thebody and the progressive loss of mental function. Themutation in the gene is present at birth in all cells of theindividual, but the effect of the protein is not evident untilmuch later. The symptoms usually develop in an affectedperson between the ages of 30 and 45 years. Penetrance is100%, there is no cure, and the progress of the disease isrelentless, leading to a terminal state of helplessness. Notherapy can significantly alter the natural progression of thedisease, and there are no states of remission. Death occurstypically 12 to 15 years after the onset of the involuntary,jerky movements. NONMENDELIAN INHERITANCESome clinical presentations do not fit the classical patterns ofmendelian inheritance and represent examples of nontraditionalor nonmendelian inheritance (see Box 3-1). These includetriplet repeats, genomic imprinting, mosaicism, and mitochondrial inheritance.Triplet RepeatsThe expansion of short tandem arrays of di- and trinucleotidesfrom a few copies to thousands of copies demonstrates a newtype of mutation with the potential of having profoundeffects on the phenotype of offspring through an unusualmode of inheritance. First demonstrated with fragile Xsyndrome, the expansion of triplet repeats is found in severalneurologic disorders. The expansion probably occurs as a resultof faulty mismatch repair or unequal recombination in a regionof instability. The proximity of the region of instability to anallele is of paramount importance. Trinucleotide repeats canbe found in any region of gene anatomy: the 5′-untranslatedpromoter region, an exon, an intron, or the 3′ untranslatedregion of the gene. Interestingly, trinucleotide expansions inany of these regions can also result in disease (Table 3-3). Theeffects of location may result in a loss of function, as seen withfragile X syndrome. A gain of function is seen with amplification of CAG, resulting in polyglutamine tracts that causeneurotoxicity in several other neurodegenerative diseases.Finally, RNA can be detrimentally affected if the expansionoccurs within a noncoding region. In myotonic dystrophy, theexpanded transcript is unable to bind RNA proteins correctlyfor splicing and remains localized in the nucleus (see Chapter 8).During normal replication, when the double helix separates into small, single-stranded regions, secondary structurescan form with complementary and repeated sequences.Thesestructures, represented as loops and hairpins, hinder theTABLE 3-3. Neurologic Disease Due to Triplet Repeat AmplificationL
shown in Table 3-1. These mechanisms are independent of mode of inheritance. Autosomal Dominant Inheritance Mendelian inheritance is classified as autosomal dominant, autosomal recessive, and X-linked (Box 3-1).A diagram repre-senting family relationships is called a pedigree and can be informative about inherited characteristics. Figure 3-1 shows