Transcription
PRIVATEPAYOROUTLOOKKELLI BACK, ATTORNEY AND APMA CONSULTANT
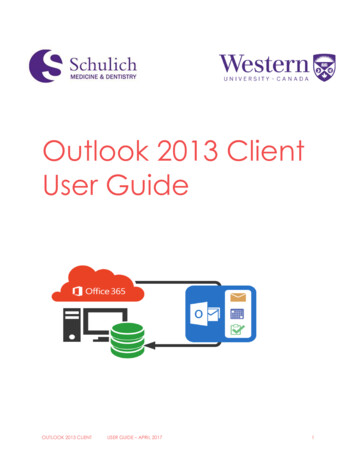
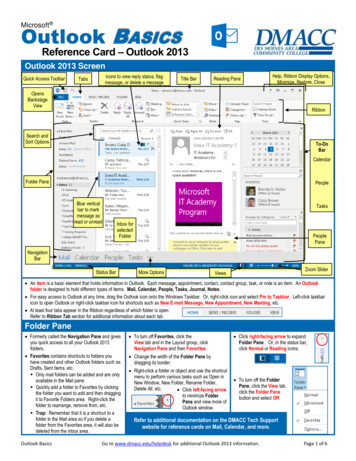
Insurance Coverage bySource (2015) Employer Group – 49% Non-group (individual and association) – 7% Medicaid – 20% (includes dual eligibles) Medicare – 14% (excludes dual eligibles) Other Public – 2% (Includes military and veterans) Uninsured – 9%
Marketplace Stability Congressional Budget Office determined that theindividual market is currently stable due tosubsidies. According to ASPE individual buying throughexchange has an average of 30 plan choices. CBO determined that the individual market wouldalso be stable under AHCA because of shifts ininsured and rearranged tax credits. Employer group market remains stable.
April 4, 2017 ACARulemaking Shortens the annual open enrollment period for 2018 toalign with Medicare and the private market. The next openenrollment period will start on November 1, 2017, and runthrough December 15, 2017, encouraging individuals toenroll in coverage prior to the beginning of the year. Requires individuals to submit supporting documentationfor special enrollment periods and ensures that only thosewho are eligible are able to enroll. Allows issuers to require individuals to pay back past duepremiums before enrolling into a plan with the same issuer.This is intended to address gaming and encourageindividuals to maintain continuous coverage.
April 4, 2017 ACARulemaking Allows issuers additional actuarial value flexibility todevelop more choices with lower premium options forconsumers, and to continue offering existing plans. Thecurrent nominal actuarial values are 90%, 80%, 70%, and60% for platinum, gold, silver, and bronze, respectively, andplans are currently allowed to deviate from these nominalvalues by a de minimis range of 2%. The rule would allowplans to deviate below the nominal AV by 4% or above thenominal AV by 2%. Eliminates duplicative review of network adequacy by thefederal government. The rule returns oversight of networkadequacy to states that are best positioned to evaluatenetwork adequacy.
Private Market Trends Continuing trend to provider consolidation. Big health systems accept risk; determine how toincentivize pay providers.
Physician Payment byPrivate Health Plans Continuing to adopt value-based paymentmechanisms. Seeing it increasingly funded by MLR savings andpaid out based on quality. Primary Care remainsthe focus, with certain exceptions for inpatientfacilities. One study shows that in 2011 46% of paymentarrangements had a value based feature –expected to increase to 75% by 2017. Medicare Advantage plans are contracting with“ACOs.”
Other MarketplaceInnovations Movement around rewards and incentives forinsured individuals. In some case requires significant health caredata.
Medicare AdvantageIssues Provider Payment Coverage Obligations Appeals Demonstrations SNPs?
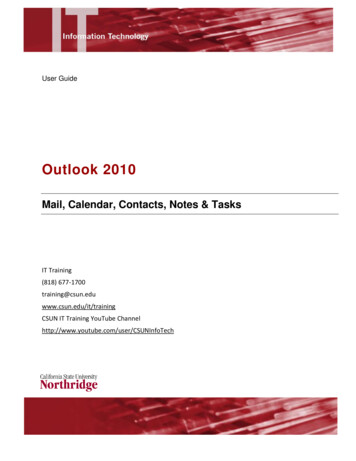
Medicare AdvantageMarket Snapshot In 2016, 31% of beneficiaries enrolled in MA plans. 2,034 Medicare Advantage plans are availablenationwide for individual enrollment in 2017 (relativelystable since 2011). HMOs represent 2/3s of these plans. 238 plans exited the market in 2016 – mainly low enrollmentplans. 271 plans were offered for the first time in 2017. Half of the 271 new Medicare Advantage plans in 2017 areoffered by UnitedHealthcare, Aetna, and BlueCross BlueShieldplans. UnitedHealthcare alone accounts for about one-quarter of allnew Medicare Advantage plans. Aetna and Humana together account for another onequarter of new plans.New organizations offered plans in nine states: California,Illinois, Iowa, Georgia, Florida, Mississippi, North Dakota,Pennsylvania, and South Carolina.
Medicare AdvantageMarket Snapshot In 2016, 7 organizations and their affiliatesaccounted for almost three-quarters of allenrollment: UnitedHealthcare, Humana, BlueCross and Blue Shield (BCBS) affiliated companies(including Anthem BCBS plans), KaiserPermanente, Aetna, Cigna, and Wellcare. These companies and affiliates account for 64percent of the plans being offered in 2017. United Healthcare and Humana are the biggestplayer by far. (39% of total MA enrollment in 2016)
Medicare Advantage CMS to offer plans “more flexibility.” Issuedrequest for information in most recent Call Letter. Key enforcement and scrutiny area has beennetwork adequacy. CMS has specifically asked whether there shouldbe different network adequacy standards forSNPs.
Medicare AdvantageProvider Payment Contracted Providers: Paid in accordance withtheir contract. CMS will generally not getinvolved in coverage disputes betweencontracted providers and MAOs. MAOs are notobligated to recognize the same modifiers orotherwise pay in the same manner as FFS if theircontract allows it. Such disputes, however, may be resolved in statecourts.Contracted Providers: Must be paid the sameamounts they would have received under FFSMedicare. Certain exceptions for some deemed providers.
Medicare AdvantageProvider Payment Contracting Provider Payment is only regulatedby Physician Incentive Payment (PIP) rules: Physicians/Physician groups may not be put at“substantial financial risk” for services they do notpersonally provide (referral services). Exception forpatient panel size 25,000. Example: A podiatrist could receive full capitation(100% risk) for services the podiatrist or podiatristgroup furnishes. Example 2: A PCP could NOT be eligible for abonus payment over 33 percent of potentialpayments minus the bonus if it is based on utilizationof hospitals and specialists.
Medicare AdvantageCoverage rules MA plans must cover all services covered under MedicareFFS plus any supplemental benefits they file in their bid. MA plans must generally follow the LCD for the place inwhich the service was provided and all NCDs. Exception: MA plans that include multiple local coveragepolicy areas in their service area may adopt a uniformcoverage policy, under which the MAO applies to planenrollees in all areas uniformly the coverage policy that isthe most beneficial to MA enrollees. Uniform Local coverage policies must be approved byCMS and information on the selected local coveragepolicy must be made readily available, including throughthe Internet, to enrollees and health care providers.
Medicare AdvantageCoverage rules Plans can put into place utilization requirementsnot used under Medicare FFS, such as anobligation to show medical necessity or priorauthorization requirements. What does “covered” mean? Does not mean provider must be paid as under FFS. Does not necessarily mean provider must be paidseparately for the service. Means that the beneficiary may obtain the servicefor the cost sharing amount set forth in the Evidenceof Coverage.
Medicare Advantageappeals rules Contracted providers: Use plan’s internal appealsprocess. Plans free to develop process. Notregulated. Processes vary greatly. Non-contracted providers: Must sign a waiver ofbeneficiary liability in order to appeal. Ist level appeal is to plan. However, if plan affirms itsdecision in whole or part, it is forwarded to anindependent CMS contractor (Maximus) withoutfurther action by the provider. 2nd level appeal to Administrative Law Judgeavailable (must meet amount in controversythreshold). 3rd level appeal to MAC
Medicare Advantageappeals rules Non-contract Provider Payment Disputes: Wherethe issue is solely whether the provider receivedthe amount of payment due under Medicare FFSdue to: Miscalculation Downcoding Never includes medical necessity issues. Plan internal appeals process would apply.
Special Needs PlansOpportunities? I-SNP, C-SNP Model of Care More small, locally based plans (exception, CareImprovement Plus, owned by United). Sometimes provider-based (particularly I-SNPs).
New MA Demonstration - ValueBased Insurance Design StartsJanuary 1, 2017 and runs 5 years 7test states available for the demo in 2017 were:Arizona, Indiana, Iowa, Massachusetts, Oregon,Pennsylvania, and Tennessee. 11plans in 4 states (CT, PA, IN, MA) applied andwere accepted for 2017 For2018, plans in Alabama, Michigan and Texascan participate
2017 plans Indiana University Health Plans Highmark Choice Company Pittsburgh, PA Tufts Associated HMO Watertown, MA Aetna Health Inc. Hartford, CT Geisinger Health Plan Danville, PA UPMC Health Network, Inc. Pittsburgh, PA Keystone Health Plan East, Inc. Philadelphia, PA Fallon Community Health Plan Worcester, MA Healthassurance Hartford, CT BCBS of Massachusetts HMO Blue
Value Based InsuranceDesign Createsrule.an exception to the uniformity of benefits Allowsfor varied plan benefit design for enrollees withthe following conditions diabetes, COPD, CHF, PastStroke, hypertension, coronary artery disease, or mooddisorders Changesto benefit design made may includereduced cost-sharing and/or offering additionalservices to targeted enrollees. ReducedCost Sharing for High-Value Services;Reduced Cost Sharing for High-Value Providers;Reduced Cost Sharing for Enrollees Participating inDisease Management or Related Programs; Coverageof Additional Supplemental Benefits
Non-discrimination:An Update
Fox-Quamme, Hess, Redfield, Chapman, and Clark, v.Health Net Health Plan Of Oregon, Inc., and AmericanSpecialty Health Group, Inc. July7, 2015 – the first lawsuit citing Section 2706 ofthe ACA was filed. OregonAssociation of Naturopathic Physicians(OANP) participated in filing a class action suit infederal court against the Health Net Health Plan ofOregon and its contracted benefits providerAmerican Specialty Health (ASH), alleging “unlawfuland discriminatory practices.” Asinitially filed Plaintiffs were 2 naturopathicdoctors and 3 patients. OANP was not a namedparty.
Fox-Quamme, Hess, Redfield, Chapman, andClark, v. Health Net Health Plan Of Oregon, Inc.,and American Specialty Health Group, Inc. Thediscriminatory Health Net/ASH practices cited inthe lawsuit include: anannual limit on the number of reimbursable visits tonaturopathic physician; therequirement of a Medical Necessity Review form, thatother providers are not required to provide; a 1,500 maximum reimbursable cap for the use ofnaturopathic medical services; alimitation on certain types of medical care performed bynaturopathic physicians that are within their scope ofpractice including, but not limited to, the delivery ofpreventative services; and, reimbursingnaturopathic doctors at up to 80% less thanother providers for the same service rather than varyingreimbursement rates based on objective quality orperformance measures.
Fox-Quamme, Hess, Redfield, Chapman, andClark, v. Health Net Health Plan Of Oregon, Inc.,and American Specialty Health Group, Inc. THREE CLAIMS FOR RELIEF – (1) Defendants actions resulted in reduced benefits toPlaintiffs and members of the Class, including deniedservices and reduced access to care. Patient plaintiffsand the class are entitled to recover benefits owed, toenforce their rights under the Plans, and to clarify rights tofuture benefits. They are also entitled to attorney fees. (2) Defendants retained funds that should have beenreimbursed to NDs, and, in some cases, to the patientplaintiffs and Class. Defendants have also profited fromreduced access to medical care caused by theirdiscriminatory practices. Patient plaintiffs and the class areentitled to equitable relief, including an injunctionprohibiting Defendant from discriminating against NDs withrespect to participation under the Plans or coverage ofservices provided under the Plans, and attorney fees.
Fox-Quamme, Hess, Redfield, Chapman, andClark, v. Health Net Health Plan Of Oregon, Inc.,and American Specialty Health Group, Inc. (3) Plaintiffs seek a declaration by this Court thatDefendants cannot discriminate against NDs withrespect to participation under the Plans orcoverage of services provided under the Plans.
Fox-Quamme, Hess, Redfield, Chapman, andClark, v. Health Net Health Plan Of Oregon, Inc.,and American Specialty Health Group, Inc.The class action sought several remedies, including:(1) reimbursement to individuals who have beendenied benefits under their Health Net healthinsurance plans;(2) repayment of profits retained by Health Net as aresult of its discriminatory practices;(3) enforcement of non-discriminatory practices inthe future; and, a court order for Health Net and ASHthat clarifies which of their practices are unlawfullydiscriminatory.
Fox-Quamme, Hess, Redfield, Chapman, andClark, v. Health Net Health Plan Of Oregon, Inc.,and American Specialty Health Group, Inc. HealthNet filed a motion to dismiss Motion was partially granted. Judge dismissed thefirst complaint without prejudice and directedOANP to file an amended complaint. OANP filed an amended complaint. Judge dismissed the third claim stating that onlypatients harmed (not providers) can seek redressunder ERISA. In April, case was dismissed. Merits were neverconsidered. Patient plaintiff could not showenough harm to have standing.
Fox-Quamme, Hess, Redfield, Chapman, andClark, v. Health Net Health Plan Of Oregon, Inc.,and American Specialty Health Group, Inc. To mitigate damages, Plaintiff agreed not toappeal the dismissal. Lessons learned: Case must be brought under ERISA Physicians don’t have standing under ERISA Finding the right patients is the hurdle. Must be ableto show damages. No way to address pay disparity through patients.
Dominion PathologyLabs v. Anthem DominionVa., Inc.Pathology Labs., P.C. v. Anthem Health Plans of Plaintiffis three-physician practice that provides biopsydiagnostic services. Anthem unilaterally cut payment forservices by 60%. Physicians negotiated with Anthem andentered an agreement, but also sued. Theybring the section 2706 anti-discrimination claims as abreach of contract claim. Both parties and the Court haveagreed there is no private right of action under section 2706. Itwas removed from Federal Court to State Court with adetermination that there was no significant question ofFederal law. Courtrecently denied a motion to dismiss, but upheldAnthem’s right to terminate its contract with the group.
Questions?
In 2016, 31% of beneficiaries enrolled in MA plans. 2,034 Medicare Advantage plans are available nationwide for individual enrollment in 2017 (relatively stable since 2011). HMOs represent 2/3s of these plans. 238 plans exited the market in 2016 - mainly low enrollment plans. 271 plans were offered for the first time in 2017.