Transcription
Presentation Handouts(9205-QE)SBB/BB Exam ReviewOctober 7, 2012 8:30 AM - 12:00 PM
Event Faculty ListEvent Title: 9205-QE: SBB/BB Exam ReviewEvent Date: Sunday, October 7, 2012Event Time: 8:30 AM to 12:00 PMDirector/Moderator/SpeakerLeeAnn Walker, MEd, MT(ASCP)SBBDirector, Red Cell Bulk SupplyImmucor, Inc.lwalker@immucor.comDisclosures: YesSpeakerWilliam Turcan, BS, MT(ASCP)SBBProgram Director, U. S. Army Blood BankFellowshipWalter Reed Army Medical Centerwilliam.turcan@med.navy.milDisclosures: NoSpeakerStacey Alvey, MEd, MT(ASCP)SBBManager, Clinical AffairsOrtho Clinical DiagnosticsSAlvey@its.jnj.comDisclosures: Yes
06/11/2012SBB/BB Exam ReviewThe SBB and BB ExamsRequirementsContentCompetenciesLeeAnn Walker, MEd, MT(ASCP)SBBImmucor, Inc.Norcross, GAASCP Exam Requirements Refer to ASCP website (www.ascp.org) forspecific requirements– Click on Board of Certification– Then US Certification– Numerous options to select more about thatlater Wealth of information available there!SBB Exam Requirements: 4 eligibility routes Most common:– Route 1 Bachelor’s degree with required courses Successful completion of CAAHEP-accredited SBB programwithin last 5 years– Route 2 MT/MLS(ASCP) or BB(ASCP) Bachelor’s degree– Course requirements met through MT/BB certification 3 yrs full-time BB experience within last 10 years after degree Must be attained with pathologist oversight1
06/11/2012BB Exam Requirements: 5 eligibility routes Most common– Route 1 MT/MLS(ASCP) and Bachelor’s degree– Route 2 Bachelor’s degree in appropriate field with requiredcourses 1 yr full-time BB experience within last 10 years– Must be attained with pathologist oversightExperience Requirements Serologic Testing– ABO, Rh Typing– Antibody detection and identification– Cross matching– Tests for other blood group antigens– Direct antiglobulin testsExperience Requirements Routine Problem Solving– Transfusion reactions– Immune hemolytic anemias– Hemolytic disease of the newborn– Rh immune globulin evaluation2
06/11/2012Experience Requirements Quality Control/Quality Assurance Laboratory Operations Donor Blood– Donor selection, preparation and collection– Processing and confirmation testing– Component preparation for storage andadministrationCompetencies Knowledge of advanced principles Technical skills Problem Solving & Analytical DecisionMaking Communication Teaching & Training Responsibilities Supervision & ManagementExam Category PercentagesSubtestBBBlood Products12%SBB10%Blood Group Systems15%17%Immunology8%6%Laboratory ology33%22%Transfusion Practice12%18%3
06/11/2012Additional information Available on ASCP website (www.ascp.org)– Click on Board of Certification / US Certification – Content outline– Reading list Exam Day Results and Certificate US MilitarySBB/BB Exam ReviewBlood GroupsStacey A. Alvey, MEd, MT(ASCP)SBBOrtho Clinical DiagnosticsPart of the Johnson & Johnson Family ofCompaniesRaritan, NJMost ImportantRead and know: Technical Manual Standards CAUTION4
06/11/2012GeneralAntigens GeneticsBiochemistryNull phenotypeEffect of chemicalsPrevalenceGeneralAntigens, cont. Racial variation Cord cell expression Soluble antigensGeneralAntibodies Characteristic reactivityTechniques for detection/confirmationHTRHDFN5
06/11/2012ABO Gene interaction - A, B, H, SeAntigen structureImmunodominant sugarsSubgroup characteristicsCauses of ABO discrepanciesResolution of ABO discrepanciesSoluble antigenImportant lectinsMNS 5 terminal amino acids for M and Nspecificity Prevalence in both White and Blackpopulations Chemical treatment Hybrid SGPsP and Globoside Soluble antigen Autoanti-P and PCH Anti-PP1Pk and spontaneous abortion6
06/11/2012Rh Rh complex Types of Weak D Inheritance of Rhnull– Lack LW and Fy5 Prevalence of 5 major antigens Antigens associated with D variantsRh Compound antigens/antibodiesAnti-G adsorption/elutionStandards for D typingHTRHDFNKell Gene interactionRacial differencesChemical treatmentKEL3 in cis positionMcLeod phenotype7
06/11/2012Lewis Soluble antigen Antigen structure Gene interaction - Le, H, SeDuffy Racial differencesChemical treatmentAnti-Fy3 vs Anti-Fy5Association with Malarial resistanceKidd Inheritance for Jk(a-b-) Jk(a-b-) resistant to lysis in 2M urea Jk(a-b-) population8
06/11/2012OtherLutheran Lu(a-b-) inheritance Lu linkage to Se Association with ALGOtherLW Association with DCord cell expressionDistinction from DAbsence on RhnullOtherI System/Collection Soluble antigen Adult and cord cell expression Disease associations9
06/11/2012Other DiegoCartwrightSciannaDombrockColtonIndianXgHigh Incidence AntigensProblem solving Phenotype clues Chemical treatment Ethnicity of antibody maker Source of units for transfusion HDFNFormer HTLA Chido/Rogers– Chemical treatment– Soluble antigen– C4 coated cells Knops– Located on CR1– Ethnicity of antibody maker– Soluble antigen10
06/11/2012Former HTLA Dombrock– Gya and Hy Cost JMH– Chemical treatmentSBB/BB Exam ReviewMethodsStacey A. Alvey, MEd, MT(ASCP)SBBOrtho Clinical DiagnosticsPart of the Johnson & Johnson Family ofCompaniesRaritan, NJGeneral Read Technical Manual MethodsSection Principle of Method Interpretation of Method Applications of Method Limitations of Method11
06/11/2012Antigen/Antibody Reactions Agglutination– Stages– Factors affecting agglutination Hemolysis Precipitation– Applications– Double diffusionAntigen/Antibody Reactions Complement Fixation ELISA– Direct assay– Competitive assay RIAFlow Cytometry Principle Gating Applications– Define cell markers– Detect minor cell populations– Antigen zygosity12
06/11/2012Red Cell Survival Applications Monocyte Monolayer Assay– Principle In vivo crossmatch– PrincipleAdsorption Types Variables– Temperature, incubation time, etc. Applications– Remove autoantibody– Separate multiple antibodies– Confirm antigen or antibody specificityElution Principle Types– Optimal recovery– Limitations Applications– Investigate positive DAT– Remove antibody for phenotyping13
06/11/2012Titration Be able to interpret a titration scheme Be careful about phenotypes of cellsused Know how to score Applications– Prenatal studies– Antibody identification– Separate antibody specificitiesNeutralizations Principle Look for Dilutional Control Sources and specificity of solublesubstances– ABH– Lewis– P1– Sda– Ch/RgCell Separations Applications Microhematocrit– Principle– Limitations Hypotonic Wash– Principle– Sickle cell disease14
06/11/2012Chloroquine Diphosphate Applications– Dissociate antibody from red cells– Denature Bg and HLA-related antigens Limitations– Complement not removed– Some antigens weakened with prolongedexposureAntilymphocyte Globulin Made from horse serumInterferes with DAT and IATRelation to Lu(a-b-)Know how to resolveEnzymes One stage vs two stage Standardization procedure– Method– Interpretation Effect on various antigens15
06/11/2012Sulfhydral Reagents AET, DTT, 2ME Principle Applications– Antigen– Antibody - know how to interpret serumtreatment (look for dilutional control)Enhancement Techniques Strengths and weakness of eachLISSPEGPolybreneBovine AlbuminNon-Traditional Techniquesfor AntibodyDetection/Identification Column Agglutination Technology– Principle– Unique components of system Solid Phase Red Cell Adherence– Principle– Unique components of system16
06/11/2012Other Donath-Landsteiner Test– Diagnosis of PCH– Method and interpretation Tests for PNH– Sucrose lysis– Ham’s testPolymerase Chain Reaction (PCR) andTranscription-Mediated Amplification(TMA) Principle Procedure Applications– PCR used for DNA amplification– TMA used for RNA amplificationSBB/BB Exam ReviewBlood DonorsLeeAnn Walker, MEd, MT(ASCP)SBBImmucor, Inc.Norcross, GA17
06/11/2012Donor Identification Identification Donor Education and Consent Donor Qualifications– review most current edition of StandardsAutologous Qualifications Physicians order Hgb 11 g/dl or Hct 33% Collected 72 hours before surgery ortransfusion Deferred if there is a risk of bacteremiaApheresis Qualifications Same requirements as allogeneic donors withthe exception of donation interval Infrequent donor– donates no more than once every 4 weeks Frequent donor– donates more frequently than once every 4 weeks max of twice / 7 day period at least 2 days between donations18
06/11/2012Plasmapheresis Frequent or InfrequentCytapheresis Frequent or InfrequentNot to exceed 24 donations / yearRegular testing for cytopeniaMonitor red cell loss and defer appropriatelyPlateletpheresis Frequent donors must have a plateletcount performed before beginning theprocedure and have a count 150,000– pre procedure plt count not required forinfrequent donors– post procedure plt count may be used toqualify the donor for the next procedureTwo-unit Red Cell Apheresis Hgb / Hct and weight according to FDAcleared device Generally: Donor Hct not 30% or Hgb not 10g/dl aftervolume replacement19
06/11/2012Unit Identification Numeric or alphanumberic system fortraceabilityPhlebotomy and Collection ofSamples Clean site to reduce bacterial contaminationAnticoagulated blood in segmentsMatching ID on unit, donor form, and samplesWear gloves when collecting autologous donorsPost -Phlebotomy Care Apply firm pressure Remain reclined until released Give the following instructions:––––––eat and drink before leavingdo not leave until releaseddrink a lot of fluid over the next few daysavoid alcohol until after a good mealdo not smoke for 30 minutesif phlebotomy site begins to bleed, raise arm and applypressure– lie or sit down if feel faint or dizzy– return to blood bank if symptoms persist– remove bandage after a few hoursAdverse Donor Reactions GeneralFaintingNausea and VomitingTwitching or muscle spasmsHematoma during or after phlebotomyConvulsionsSerious cardiac difficultiesRecord all incidents20
06/11/2012SBB/BB Exam ReviewBlood Components Preparation and StorageLeeAnn Walker, MEd, MT(ASCP)SBBImmucor, Inc.Norcross, GAAnticoagulants Prevent clotting and maintain cell viability andfunction during storage––––Dextrose: supports ATP generationAdenine: provides substrate for ATP synthesisSodium biphosphate: controls the pHCitrate: prevents coagulation 21 day storage CPD, CP2D 35 day storage CPDA-1 42 day storage– AS-1 (Adsol), AS-3 (Nutricel), AS-5 (Optisol)Red Cell Components Whole blood (1-6oC)Red Blood Cells (1-6oC)Frozen Red blood Cells (-65oC or colder)Rejuvenated RBCs (1-6oC)Deglycerolized RBCs (1-6oC up to 24 hours)Washed RBCs (1-6oC up to 24 hours)Pre-storage RBCs LeukoreducedLow Volume RBCsApheresis RBCsIntraoperative RBCs21
06/11/2012Plasma Components Fresh Frozen PlasmaThawed PlasmaPlasma Frozen Within 24 hours of collectionPlasma and Liquid PlasmaPlasma Cryoprecipitate ReducedSolvent/Detergent-Treated Pooled PlasmaDonor Retested Plasma“Linked” FFPRecovered PlasmaCryoprecipitatePlatelets Platelet Concentrates Platelet - Apheresis Modifications of olume-reducedAliquotsWashedFrozenGranulocytes Usually collected by apheresis Buffy coat harvest Yield must be a minimum of 1.0 x 1010granulocytes Transfuse as soon as possible aftercollection22
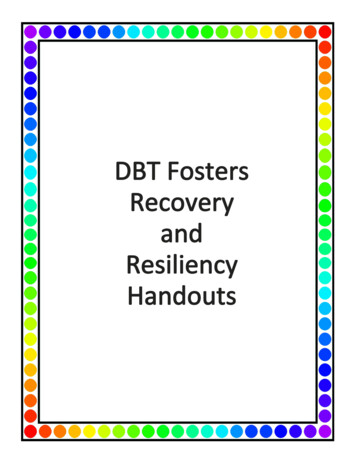
06/11/2012Component Modifications CMV-negative– reduces the risk of CMV transmission– leukoreduced may be an alternative Irradiated– prevents T lymphocyte proliferation; theprimary cause of GVHDEffects of Storage on BloodComponents 2,3 DPG levels ATP K Oxygen Dissociation Curve Based on affinities of tissues for oxygen Relationship between pO2 and O2 saturationof HGB pO2 : oxygen pressure of tissues p50 : pO2 level at which HGB is 50% saturated A normal p50 corresponds to 25 pO2 p50 right shift; more oxygen released p50 left shift; less oxygen is released23
06/11/2012Oxygen Dissociation CurveSBB/BB Exam ReviewDonor Testing,Transfusion TransmittedDisease Testing & Re-entryLeeAnn Walker, MEd, MT(ASCP)SBBImmucor, Inc.Norcross, GAGeneral Requirements ABO and Rh Antibody Screen– with history of transfusion or pregnancy ALT– not required by the FDA or AABB– plasma sales for further manufacturing24
06/11/2012General Requirements (cont.) HBsAgAnti-HBcAnti-HCVHCV-RNA (NAT)Anti-HIV-1/2HIV-1 RNA (NAT)Anti-HTLV-I/IIWNV RNASyphilisAntibodies to Trypanosoma cruziBacterial Detection (platelets)(tested once)Hepatitis B Infection Anti-HBs and Anti-HBc persist afterrecovery and indicate immunity HBsAg and Anti-HBc persist in chroniccarriers while Anti-HBs is absentInvalidation of Test Results Faulty equipment, improper procedure,compromised reagents and/or Internal control results do not meetpackage insert acceptance criteria– all results, reactive and non-reactive, must berejected– all specimens must be tested in a new runwhich becomes the test of record25
06/11/2012Acceptable Test Results No error in test performance Internal batch controls are acceptable– remains test of record– reactive results must be retested in duplicate,per manufacturer’s instructionsExternal Controls Purchased commercially Used for surveillance of test performance Tested the same as donor samples Non-reactive test results can beinvalidated based on the external controlsbut if all other manufacturer’s guidelineswere followed, external controls cannotbe used to invalidate reactive test resultsSupplemental and ConfirmatoryTests Neutralization: HBsAg and HIV-1AgWestern Blot: Anti-HIVRIBA: Anti-HCVAnti-HTLV confirmation26
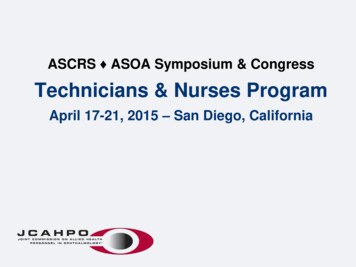
06/11/2012Re-entry AlgorithmHTLV Testing Indefinite deferral:– 2 or more reactive HTLV EIA screening assays– 1 reactive HTLV EIA screen and 1 reactive HTLVEIA by second manufacturer 8-week eligible:– 1
Event Title: 9205-QE: SBB/BB Exam Review Event Date: Sunday, October 7, 2012 Event Time: 8:30 AM to 12:00 PM Director/Moderator/Speaker LeeAnn Walker, MEd, MT(ASCP)SBB Director, Red Cell Bulk Supply Immucor, Inc. lwalker@immucor.com Disclosures: Yes Speaker Stacey Alvey, MEd, MT(ASCP)SBB Manager, Clinical Affairs Ortho Clinical Diagnostics SAlvey@its.jnj.com Disclosures: