Transcription
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Higher Levels Of Care:General Inpatient Care, ContinuousCare & RespiteSubscriber Audio ConferenceSeptember 2013The Plan for Today1.Identify the regulatory requirements forgeneral inpatient, respite, andcontinuous home care levels2.Apply documentation principles tosupport the general inpatient andcontinuous home care levels of care3.Recognize what monitors and audits ahospice should have in place All Rights ReservedHospice Fundamentals. 20131
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Levels of Care (LOC)Medicare pays the hospice a per diem rate based onone of four levels of care Routine Home Care Inpatient Respite Care General Inpatient Care Continuous Home CareLevel of care determination Made by the hospice interdisciplinary team (IDG) Reevaluated by the IDG on a regular basis to assureappropriateness Requires a change to the plan of care (POC)A View of the Regulations All Rights ReservedHospice Fundamentals. 20132
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Respite Short-term inpatient care to provide relief tothe family members or other persons caringfor the individual May be provided only on an occasional basis May not be reimbursed for more than fiveconsecutive days at a time May not be provided to residents of a nursingfacility§418.204 Special Coverage RequirementsRespite – Where? Medicare-certified hospice that has inpatient facility Medicare-certified hospital Medicare or Medicaid certified nursing facility Must be able to provide 24-hour nursing servicesthat meet nursing needs of all patients Furnished according to the patient’s POC Patient must receive all nursing services as prescribed Must be kept comfortable, clean, well-groomed, andprotected from accident, Injury, and infectionQDoes the facility have to have RN coverage 24 hours / day?ANot according to Medicare but dependent on individual stateregulations All Rights ReservedHospice Fundamentals. 20133
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013General Inpatient Care (GIP) A day in which a patient receives hospice inpatientcare for procedures necessary for pain control oracute or chronic symptom management that cannotfeasibly be provided in other settings Where Contracted hospital Contracted skilled nursing facility (Medicarecertified) Hospice inpatient facility – you own or contract(Medicare-certified) Facility must have RN 24 hours/day who providesdirect careGeneral Inpatient Clarification Final Rule CMS-1539 effective August 2007 Clarifications GIP should only be used based on the patient condition When an individual’s pain and symptoms must be closelymonitored or the intensity of interventions that are requiredcannot be provided in any other settings GIP can not be used due to caregiver breakdown Advised respite should be used in these circumstances (respitecannot be used for residents of a nursing facility)FY 2008 Wage Index Final RuleCMS-1539effective August 20078 All Rights ReservedHospice Fundamentals. 20134
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013General Inpatient Care The decision to change a patient’s care to thegeneral inpatient (GIP) level is based on theclinical condition of the individual General inpatient care requires thedocumentation of an acute change in thepatient’s condition, requiring aggressive,intensive treatment for the management ofsymptoms Why was the hospice unable to manage thesymptoms at the current level of care?General Inpatient CareIntensity of care directed towards paincontrol and symptom management thatcannot be managed in any other setting Close monitoring of pain and symptoms Level of care needed to manage pain andsymptoms is the basis for the GIP level of care “procedures necessary for pain control oracute or chronic symptom management”§418.202(e) All Rights ReservedHospice Fundamentals. 20135
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013General Inpatient CareGeneral inpatient care under the hospice benefitis not equivalent to a hospital level of care underthe Medicare hospital benefit A brief period of general inpatient care may beneeded in some cases when a patient elects thehospice benefit at the end of a covered hospital stay Patient continues to need pain control or symptommanagement Cannot feasibly provide in other settings while thepatient prepares to receive home careGIP Level of Care in a Contracted Facility Hospice maintains professional managementof the patient Documentation by hospice staff should reflect thatmanagement Should illustrate the coordination of care betweenthe hospice and the contracted facility providing GIPlevel of care On discharge – need either a dischargesummary or copy of the facility clinical record Includes residents of NF All Rights ReservedHospice Fundamentals. 20136
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Discharge Criteria from GIP Medical reasons for admission havestabilized Re-established family support systemDischarge planning starts on admissionand is reviewed daily What is Plan A? What is Plan B?Continuous Home CarePeriods of crisis Nursing care may be covered on a continuous basis for asmuch as 24 hours a day during periods of crisis asnecessary to maintain an individual at home Either homemaker or home health aide (also known ashospice aide) services or both may be covered on a 24hour continuous basis during periods of crisis but careduring these periods must be predominantly nursing A period of crisis is a period in which a patient requirescontinuous care, of which more than half is nursing care, toachieve palliation or management of acute medicalsymptoms and only as necessary to maintain the patient athome§ 418.204Special coverage requirements nursing care All Rights ReservedHospice Fundamentals. 20137
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Continuous Home Care Payment for continuous home care may bemade for up to 24 hours/day Requires a minimum of eight hours of careduring a 24-hour period that begins andends at midnight More than half of the care in any 24-hourperiod must be provided by a RN orLPN/LVN Billable time stops when patient diesContinuous Home Care All hospice aide or homemaker hours must beincluded in the computation May not “discount” any portion of the hours in order to meetthe requirement that the care be predominantly nursing care Only direct patient care during the period of crisis Cannot count time waiting for the patient to arrive Post mortem care does not count towards hours to meet therequirements Modification of the plan of care and supervision of aides doesnot qualify as direct care nor would it qualify as necessitatingthe services of more than one provider Care does not need to be continuous All Rights ReservedHospice Fundamentals. 20138
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Counting Continuous Care Hours CHC billing should reflect direct patient careduring a period of crisis It does not reflect time related to staff working hours,time taken for meal breaks, time used for educatingstaff, time used to report etc. Continuous care hours are counted in 15minute increments Rounding to the next whole hour is not permitted Units should only be rounded to the nearestincrementOverlapping of Hours May be circumstances when patient's needsrequires more than one covered discipline at atime Results in an overlapping of hours between the nurseand hospice aide. Overlapping hours are counted separately Ensure that these direct patient care servicesare clearly documented and are reasonable andnecessary Would be an unusual circumstance All Rights ReservedHospice Fundamentals. 20139
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Continuous Home Care Nursing care Skilled observation and monitoring when necessary Skilled care needed to control pain and other symptoms If a patient’s caregiver has been providing a skilledlevel of care and the caregiver is unwilling or unableto continue providing care; may precipitate a period ofcrisis because the skills of a nurse may be needed toreplace the services that had been provided by thecaregiver May be provided to beneficiaries residing in nursingfacilitiesCHC for Patients in NFs Documentation not only reflects care providedby hospice staff but also care provided by NFstaff Include copy of NF MAR to reflectmedications administered during the period ofcrisis if hospice staff not administering Documentation includes care coordinationwith NF staff All Rights ReservedHospice Fundamentals. 201310
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013CHC Documentation Must clearly support the reason (orcrisis) and the need to intervene Must illustrate hour by hour, day by day What services provided Patient’s condition/response to care Type of personnel providing careNeed for Higher Level of Care Guidelines / reasons for CHC are basicallythe same as for GIP level of care CHC is an attempt to solve / manage thecrisis while allowing the patient to remain athome GIP is for when an inpatient level of care isneed to solve / manage the crisis for thosewho cannot or do not wish to remain athome All Rights ReservedHospice Fundamentals. 201311
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013What Is Defined as a Crisis? Palliation / management of acute medical symptoms Observation and monitoring to control pain and otheracute symptoms Require predominantly nursing care Actively dying? Must be a clinical need for services,such as pain control Caregiver breakdown? Must have a skilled nursingneed going unmet because the caregiver is unwillingor unable to provide the skilled nursing carePsychological and Social ProblemsQuestions to ask & responses to document What is the specific patient care need goingunmet as a result of the caregiver crisis? Why can’t it be managed in the home? Does the patient need placement in afacility?Does the documentation tell the story? All Rights ReservedHospice Fundamentals. 201312
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013The Role of the IDG GIP & CHC are primarily focused on skillednursing needs to met the unmet needs of thepatient However . The services of SWs and chaplains are expected toincrease during these periods of crisis SW and chaplain continue to address the psychosocial /spiritual issues which may have escalated depending onthe crisis Assessments and plan of care Determine if the family will be able to care for the patientat home when the crisis is overCues for Need of Higher Level of Care Increase calls to the office for help Difficulty managing symptoms withintermittent visits Increase in after hours calls Statements of wanting to go to the hospitalor to call 911 Caregiver’s anxieties and fears escalatingto where no longer can provide skilled care All Rights ReservedHospice Fundamentals. 201313
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013So, How Does Documentation Fit InWith All of This?Admitting Documentation What is the clinical need precipitated by thecrisis Document failed interventions in the othersetting (home, NF, ALF, etc.) Reasons why new interventions can’t beprovided in the other setting Why the family can no longer provide the care For patients in contract GIP in NF, how will theNF care be different? More intense?Paint the picture why management in theircurrent environment is not realistic All Rights ReservedHospice Fundamentals. 201314
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Documentation of GIP & CHC LOCs Should Answer these questions Why here? What is happening that can’t be managed in the home or atcurrent level in facility setting? Reflect a more intensive level of care – should notread the same as routine home care notes Expect to see Medication adjustments or other stabilization treatments Measures being taken to resolve the reason for admission orcontinued stay Supporting documentation that the family / NF cannot provideneeded careDaily DocumentationShould include What is the reason for level of care now (today) Assessment of signs and symptoms Medication changes, titration, patient response ADL needs and dependency Vital signs Caregiver teaching Discharge planningPaint the picture of the patient and patient needsas identified on the Plan of Care All Rights ReservedHospice Fundamentals. 201315
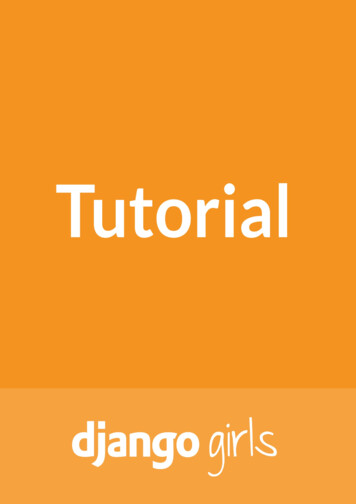
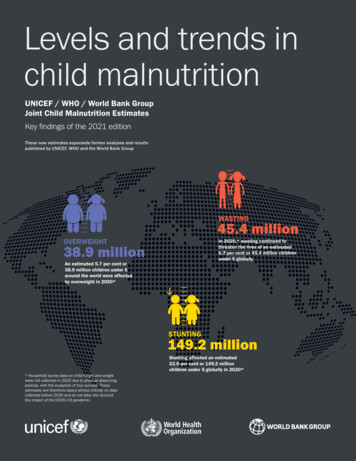
Documentation of Symptom ManagementPain Control1. At home, pain was out ofcontrol despite medicationchanges2. Through and complete painassessment(s)3. Medication adjustments,interventions and response;route, titration, use of PRNs,frequency4. Use of any complimentarytherapies and responseRespiratory Distress1. Breath sounds / or lack of2. Uncontrolled secretions /frequent need forsuctioning3. Severity of dyspnea4. Associated tachypnea5. Cough with evidence ofsymptoms such as anorexia,nausea, vomiting,exhaustion, rib fracture,musculoskeletal pain6. Anxiety level7. Difficulty sleeping /sleeping position8. Restlessness9. Elevation of head of bed10. Inability to complete asentence without gasping11. SVN treatmentsNausea/Vomiting/Diarrhea1. Nausea / diarrheaintractable at home withcurrent antiemetic / anti‐diarrhea regime2. Assessment of nausea,diarrhea and interventions3. Frequency, amount, type ofemesis or diarrhea4. Complaints of nauseawithout emesis5. Effects of diarrhea on skinintegrity6. Hydration statusFamily Caregiving Teaching1. Caregiver need to learn newmodality2. Caregiver willingness tolearn3. Modifications to plan ofcare to adapt into a homesetting4. Actual caregiver teachingprovided and level ofunderstandingImminent Death1. Terminal restlessnessa. Agitationb. Deliriumc. Hallucinations2. Clinical signs and symptomsof imminent death3. Inability for family to copewith the patient dying athomea. Psychologicalinterventionsb. SpiritualinterventionsWound Care1. Type of wounda. Painfulb. Malodorousc. Disfiguring2. Frequent dressing changes3. Description of wound4. Medication(s) required priorto dressing changes5. Dressing changes and othertreatments6. Patient’s response totreatments, dressingchangesAgitation1. Description of patientbehaviors2. Need for presence tocontrol3. Effect of agitation onpatient and family4. Amount, frequency, andeffectiveness of medicationrequired to control agitationAscites1. Respiratory compromise2. Diuretic history andresponse3. Response to paracentesis (ifapplicable)4. Abdominal girth5. Other edemaFluid Overload1. Position of patient2. Oxygen needs3. Amount of dyspnea4. Edema (amount andlocation)5. Difficulty sleeping at night6. Cardiac statusInsomnia1. Lowered pain threshold2. Sleep patterns3. Assessment of psychosocialhistoryHospice Fundamentals Subscriber AudioconferenceHigher Levels of Care: GIP, Continuous Care & Respite All Rights Reserved Hospice Fundamentals 2013September 2013
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Monitoring & AuditingProcesses to MonitorReview of clinical notes to supportlevel of care Crisis management Documentation supports ongoingneed All Rights ReservedHospice Fundamentals. 201316
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Processes to MonitorIDG updates the POC when change level of care From RHC to CHC From RHC to GIP From CHC to RHC From GIP to RHCCHC Processes to Monitor Continuous home care log Time patient staff began care Time patient died Clinical notes Hourly documentation present Verify logs to documentation for accuracy oftimes Predominantly nursing care (RN/LPN) All Rights ReservedHospice Fundamentals. 201317
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013Summary – Key Concepts CHC § 418.204 – Special coverage requirements Nursing care may be covered on a continuousbasis for as much as 24 hours a day duringperiods of crisis as necessary to maintain anindividual at home A period of crisis is a period in which a patientrequires continuous care, of which more than halfis nursing care, to achieve palliation ormanagement of acute medical symptoms andonly as necessary to maintain the patient at homeSummary – Key Concepts – GIP §418.108 – Short – term inpatient care Meant to be short term Medicare Benefit Manual clearly states thatcare under GIP must be care that “cannotfeasibly be provided in other settings” Documentation must demonstrate why carecannot be provided at “home” All Rights ReservedHospice Fundamentals. 201318
www.hospicefundamentals.comHospice Fundamentals Subscriber WebinarSeptember 2013To Contact UsWe are here for you!!!Info@HospiceFundamentals.comSusan Balfour(919) 491-0699Susan@HospiceFundamentals.comRoseanne harlene Ross602-740-0783Charlene@HospiceFundmentals.com All Rights ReservedHospice Fundamentals. 201319
Continuous Home Care Payment for continuous home care may be made for up to 24 hours/day Requires a minimum of eight hours of care during a 24-hour period that begins and ends at midnight More than half of the care in any 24-hour period must be provided by a RN or LPN/LVN Billable time stops when patient dies Continuous Home CareFile Size: 209KB