Transcription
Supplementary AppendixThis appendix has been provided by the authors to give readers additional information about their work.Supplement to: Foà R, Bassan R, Vitale A, et al. Dasatinib–blinatumomab for Ph-positive acute lymphoblasticleukemia in adults. N Engl J Med 2020;383:1613-23. DOI: 10.1056/NEJMoa2016272
SUPPLEMENTARY APPENDIXPageList of participating centers and investigators2Supplementary Methods4Supplementary Results8Supplementary Figures9- Figure S1. Treatment scheme9- Figure S2. Heat map of additional copy number aberrations10- Figure S3. Molecular clearance among p190 and p210 and p190/p210 patients11- Figure S4. DFS according to molecular response (A) and fusion type (B)12- Figure S5. Tregs cell percentages from paired samples measured before and duringblinatumomab treatment13Supplementary Tables14- Table S1. Sequences of primers used for the amplification of ABL1 KD mutations14- Table S2. Adverse events documented in the trial15References161
List of participating centers and investigatorsCenter086 - Ospedale dell’Angelo and Ospedale SS Giovanni ePaolo, Venice014 - Division of Hematology, Cardarelli Hospital,Naples028 - Division of Hematology, Department ofTranslational and Precision Medicine, SapienzaUniversity of Rome005 - Azienda Socio-Sanitaria Territoriale PapaGiovanni XXIII, Bergamo115 - Division of Hematology, Department ofTranslational Medicine, University of Eastern Piedmont,Novara019 - AO Ospedali Riuniti Villa Sofia Cervello Palermo024 - Department of Hematology, Ospedale Civile,Pescara043 - Department of Medicine, Section of Hematology,University of Verona045 -UOC Oncoematologia, Fondazione IRCCS Ca’Granda Ospedale Maggiore Policlinico di Milano,Università degli Studi di Milano004 - AOU consorziale Policlinico - Bari - UOEmatologia con Trapianto022 - AO di Perugia - Ospedale S. Maria dellaMisericordia - Ematologia e Trapianto Midollo Osseo044 - AOU San Luigi Gonzaga - SCDU EmatologiaGenerale e Oncoematologia133 - ASL Lecce - Ospedale ‘V. Fazzi’ - UO Ematologia170 - Ospedale Mauriziano Umberto I - Torino - SCDUEmatologia008 - CTC U.O di Ematologia con Trapianto di MidolloOsseo – Catania010 - AOU Careggi - Firenze - SOD Ematologia026 - Grande Ospedale Metropolitano ‘BianchiMelacrino-Morelli’ - Reggio Calabria - UOC Ematologia027 - Fondazione Policlinico Universitario AgostinoGemelli IRCCS - Roma - Area ematologica038 - AOU di Parma - SC Ematologia e Centro TrapiantiMidollo Osseo051 - IRCCS Ospedale S. Raffaele - Milano - UOOncoematologia055 - ASST degli Spedali Civili di Brescia - UOEmatologia087 - AUSL della Romagna - Ospedale ‘Santa Mariadelle Croci’ - Ravenna - Ematologia090 - Istituto clinico Humanitas - Rozzano - UOOncologia Medica ed Ematologia2PIRenato BassanFelicetto FerraraRobin Foà/Sabina ChiarettiAlessandro RambaldiGianluca GaidanoFrancesco FabbianoNicola Di Bartolomeo/Massimiliano BonifacioNicola FracchiollaFrancesco AlbanoBrunangelo FaliniGiovanna Rege CambrinNicola Di RenzoAlessandro CignettiFrancesco Di RaimondoAlberto BosiBruno MartinoSimona SicaMonica CrugnolaFabio CiceriErika BorlenghiMichela RondoniMatteo Della Porta
101 - ASL Salerno - Presidio Ospedaliero Tortora PaganiCatello Califano– Ematologia105 - AO Complesso Ospedaliero San GiovanniLaura CudilloAddolorata - Roma - UOC Ematologia301 - Hematology, Department of Biomedicine andAdriano VendittiPrevention, University Tor Vergata, Rome3
SUPPLEMENTARY METHODSRNA isolation and cDNA synthesisRNA extraction was performed from centrally prepared aliquots of cell dilutions lysed and homogenizedin guanydium isothiocyanate. At diagnosis, total RNA was extracted by columns following the instructionof the RNeasy Mini Kit (Quiagen, Hilden, Germany). During minimal residual disease monitoring, totalRNA was extracted by the automated Maxwell Instrument using the Total RNA Purification Kit (PromegaCorporation, Madison, WI). cDNA synthesis was performed using the SSIV Vilo Mastermix W/ez DNAse(Invitrogen, Carlsbad, CA) at diagnosis and by the Superscript Vilo CDNA Synthesis Kit (Invitrogen) forMRD monitoring samples.Multiplex-PCR at diagnosisAt diagnosis, a multiplex RT-PCR with a nested approach designed to detect the most common ALL fusiongenes - TCF3-PBX1, ETV6-RUNX1, SIL-TAL, NUP98-RAP1GDS1, SET-NUP214, BCR-ABL1 p190 (e1a2)and p210 (e13a2, e14a2), KMT2A/AFF1 (alias MLL-AF4) and KMT2A/MLLT1 (alias MLL-ENL) - wascarried out.1Q-RT-PCR for minimal residual disease monitoringThe number of BCR-ABL1 copies and the result interpretation were determined according to the“Standardization and consensus guidelines for minimal residual disease assessment in Philadelphia-positiveacute lymphoblastic leukemia by real-time quantitative reverse transcriptase”, the method developed by theEuro-MRD Consortium.2,3 All Q-RT-PCR reactions were performed on a 7500 fast ABI platform (LifeTechnologies, Carlsbad, CA). The number of amplification cycles was set at 50. Moreover, a commonthreshold set at 0.1 was selected in order to remain within the exponential phase. In determining the integrityof RNA, the criteria for excluding RNA samples was established as an ABL1 copy number 10000 fornegative samples and 1000 for those positive and quantifiable. The number of BCR-ABL1 copies wasnormalized with respect to the number of ABL1 copies and expressed as the number of BCR-ABL1/ABL1copies x 102.The quantity range was defined by the lowest dilution of standards with a reproducible Delta-CT of allreplicates ( 1.5 CT), a specific amplification (determined by shape and multicomponent graph), a meanCT value within 2.6-4.0 CT for a one log difference and 0.5-1.5 CT for two fold dilutions.Minimal residual disease-positive samples outside the quantitative range were scored as positivenonquantifiable. The sensitivity of the assay was defined as the lowest dilution of standards positive with aspecific amplification curve.2,34
All experiments were carried out in triplicate, with appropriate negative controls and a control that includeda mixture of all reagents without RNA, to rule out the possibility of cDNA contamination of RNA samples.Mutation analysis by Sanger sequencingBCR-ABL1 kinase domain (KD) mutation analysis was performed by Sanger sequencing (SS) in patientswith a MRD increase or at hematologic relapse. For ABL1 KD amplification, a nested-PCR approach wasused.4 The first amplification step was performed using 3 µL of cDNA and the following primers (TableS1): fwd-BCR-p210 (located on BCR mRNA exons 12/13) or fwd-BCR-p190 (located on BCR mRNA exon1a) and a rev common-ABL1 (located on ABL1 mRNA exon 8). This procedure ensured that the wild-type,non-rearranged ABL1 transcript was not analyzed. An initial denaturation step of 10 min at 95 C wasfollowed by an amplification for 35 cycles (denaturation for 30 s at 94 C, annealing for 1 min at 60 C,extension for 1 min at 72 C) and final extension for 10 min at 72 C. In the second amplification step, 2 µLof the first PCR product was then performed with 2 internal primer pairs: fwd-B-ABL1/Rev-B-ABL1 andfwd-C-ABL1/Rev-C-ABL1. In this way, the ABL1 kinase domain was divided into two partially overlappingfragments: fragment B (393 bp, spanning codons 206-335) and fragment C (482 bp, spanning codons 262421). For the second amplification step, the following PCR conditions were used: initial denaturation of 10min at 95 C, amplification for 30 cycles (denaturation for 30 sec at 94 C, annealing for 1 min at 58 C,extension for 1 min at 72 C), and final extension for 10 min at 72 C.All PCR experiments were performed in a 25 µL final volume containing 0.5U of AmpliTaq Gold(Invitrogen), 10X PCR Gold buffer (Invitrogen), 2.5 mM MgCl2 solution (Invitrogen), 2.5 mM each dNTP(Invitrogen), 25 pmoles of each primer for the first amplification step and 50 pmoles of each primer for thesecond amplification step.Specificity and efficiency of the amplification reactions were checked by electrophoresis of a 10 µL aliquoton ethidium bromide-stained 1.5% agarose gel.Copy number aberration analysisThe copy number status of IKZF1, CDKN2A or CDKN2B, PAX5, ETV6, EBF1 and BTG1 was investigatedby multiplex ligation-dependent probe amplification (MLPA) using the Salsa MLPA P335 ALL IKZF1 kit(MRC-Holland, Amsterdam, The Netherlands) and following the manufacturer’s instructions. This kitcontains probes for selected B-cell development and differentiation genes, and permits to detectabnormalities with a sensitivity of 20-30%. The full list and location of the MLPA probes are available atthe MRC Holland website (http://www.mrc-holland.com). One hundred ng of gDNA extracted from BMsamples of the patients were used, and gDNA extracted from 10 healthy donors was used as wild-typecontrol, at least 3 per experiment. Amplicons were separated on an ABI-Prism 3130 sequencer and analyzed5
by GeneMapper 4.0 software (Applied Biosystem, Life Technologies, Foster City, CA). The detection ofabnormal copy number values was performed using the Coffalyser.Net software and the manufacturer’sinstructions (www.coffalyser.net).Immunologic compartment evaluationA total of 197 samples of fresh PB were evaluated in a longitudinal analysis on paired samples from 43patients. Forty-three samples were collected prior to blinatumomab treatment (pre-blina), 38 after the firstcycle (1st blina), 40 after the second cycle (2nd blina), 29 after the third cycle (3rd blina), 25 after the fourthcycle (4th blina) and 22 after the fifth cycle (5th blina). To follow intra-individual variations, the T and NKcell compartments were investigated in a complete longitudinal analysis of 17 patients evaluated prior toblinatumomab treatment and at all time points.PB mononuclear cells were obtained by centrifugation on Ficoll-Histopaque (Axis-Shield, Oslo, Norway);for surface marker analysis, cells were incubated at room temperature for 30 min with the followingmonoclonal antibodies: CD45RA, CD45R0, CD3, CD4, CD8, CD16, CD56, CD57, CD62L, CD69 (allfrom Becton Dickinson [BD] Biosciences, San Josè, CA).To assess the presence of regulatory T (Tregs) cells (defined by the combined expression of CD3, CD4,CD25 and FoxP3), cells were stained with the following monoclonal antibodies: CD25-FITC, CD4-PerCPand CD3-APC, and then fixed and permeabilized (FIX and PERM kit BD) and stained with anti-humanFOXP3-PE (BD). For each analysis, 100000 events were acquired, and analyzed using the FACSDivasoftware (BD). Data were checked for normality with the Kolmogorov-Smirnov test. Due to non-parametricdata distribution, comparisons of continuous parameter in different groups were evaluated by Wilcoxonsigned rank test for paired samples as indicated. Data are reported as median percentages.Statistical analysisThe study was designed to evaluate the activity of dasatinib plus 2 cycles of blinatumomab in obtaining amolecular response in adult Ph ALL, considering the null hypothesis - 40% of patients (based on data ofthe historical control group - the GIMEMA LAL1509 protocol5) and the alternative hypothesis, fixed at60%, with a 90% power and a 5% significance level using a single stage phase II design. If the total numberof patients achieving a molecular response was at least 29, the primary endpoint was considered reached.Categorical data are presented as frequencies and percentages. For continuous data, median and ranges arepresented. Overall survival was calculated from the date of treatment start for all patients while diseasefree survival and cumulative incidence of relapse were calculated from the end of induction (day 85) forpatients in complete hematologic remission. The cumulative incidence of relapse was calculated using thecumulative incidence method, with death in complete hematologic remission being a competing risk. The6
median follow-up for survival was calculated using the reverse Kaplan-Meier (K-M) estimate and thedistribution of time-to-event endpoints (overall survival and disease-free survival) was estimated using theK-M method and differences between groups were analyzed using two-sided log-rank tests. K-M rates at 1year with 95% confidence interval are reported. Hazard ratios with a 95% confidence interval wereestimated using the Cox proportional model.All above analyses were performed to evaluate: (1) molecular response status (molecular responders vs nomolecular responders), (2) presence of additional genomic deletions (IKZF1 plus PAX5 and or CDKN2Aor CDKN2B vs no IKZF1 or IKZF1 alone), (3) type of fusion protein (p190 vs p210).95% confidence intervals were not adjusted for multiple comparisons and should not be used to inferdefinitive treatment effects. All analyses were performed using the SAS (version 9.4) and R (R Foundationfor Statistical Computing, Vienna, Austria) system software. Study data were collected and managed usingthe REDCap electronic data capture tools hosted at the GIMEMA Foundation.6,77
SUPPLEMENTARY RESULTSPatients’ flow after inductionReasons for discontinuation were as follows: 1 death in complete hematologic remission before startingblinatumomab; 1 excessive toxicity and 1 relapse due to a major protocol violation (delay in blinatumomabadministration) between the end of the induction and the 1st cycle of blinatumomab; 1 nodal relapse and 1medical decision (the patient was allocated to an allogeneic transplant between the 1st and 2nd cycle ofblinatumomab; 9 protocol completions (6 patients were allografted) and 2 relapses (1 nodal, 1 at the centralnervous system (CNS)) between the 2nd and 3rd cycle of blinatumomab; 7 protocol completions (7 patientsunderwent an allogeneic transplantation) and 1 CNS relapse between the 3rd and 4th cycle of blinatumomab;7 protocol completions (4 patients were allografted) between the 4th and 5th cycle. Finally, 29 patientsunderwent 5 cycles of blinatumomab and 5 of them were allografted (Figure 1).Adverse eventsA total of 60 adverse events, regardless of the grade, in 28 distinct patients were recorded (Table S2). Themost frequent were represented by persistent fever occurring in 12 patients; 8 adverse events were sustainedby infections, particularly CMV infections or reactivation (6 and 1, respectively). Finally, 8 neurologicadverse events were reported, all reversible.None of the material in the Supplementary Appendix is under copyright by a third party.8
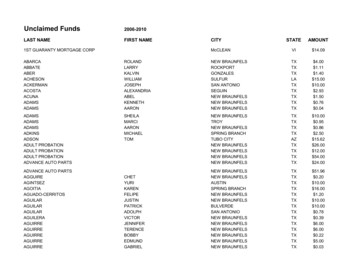
SUPPLEMENTARY FIGURESFigure S1. Treatment scheme.9
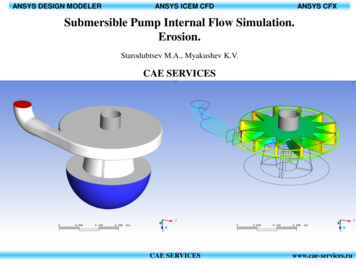
Figure S2. Heat map of additional copy number aberrations.10
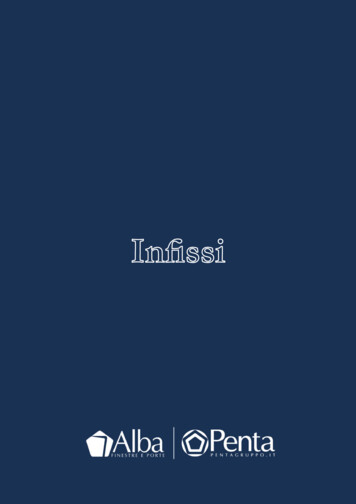
Figure S3. Molecular clearance among p190 and p210 and p190/p210 patients.11
Figure S4. DFS according to molecular response (A) and fusion type (B).12
Figure S5. Tregs cell percentages from paired samples measured before and during blinatumomabtreatment.13
SUPPLEMENTARY TABLESTable S1. Sequences of primers used for the amplification of ABL1 KD mutations. Primer positions areprovided, according to GenBank mRNA sequences X02596 (for BCR) and X16416 (for ABL1).Primer nameFwd-BCR-P210Fwd-BCR-P190Rev Sequence 5’à 3’PositionsGAGCAGCAGAAGAAGAAGTGTTTCA BCR, exons12/13(nt 3075-3096)GACTGCAGCTCCAATGAGAACBCR, exon 1(nt 1479-1499)CTCTAGCAGCTCATACACCTGGABL1, exon 8(nt 1485-1506)CATCATTTCAACGGTGGCCGACABL1, exon 4(nt 748-768)GTTGCACTCCCTCAGGTAGTCABL1, exon6(nt 1120-1140)GAAGAAATACAGCCTGACGGTGABL1, exon 4(nt 930-951)AGACGTCGGACTTGATGGAGAAABL1, exon 7(nt 1393-1414)14Amplicon (length)b3a2 (1476bp)b2a2 (1401bp)e1a2 (759bp)B (393bp)C (485bp)
Table S2. Adverse events documented in the trial.Adverse eventsGeneral disorders andadministration site .112.1511.1.312611112Neurologic signs niaConfusional stateAnemiaNeutropeniaAlanine tamyltransferaseincrease.1.12Hepatic function abnormalDiarrhoeaVomiting.21111.1.1213Atrial .112.11.1.1AstheniaPeripheral edemaPyrexiaCytomegalovirus infectionCytomegalovirus viremiaInfectionPneumoniaAphasiaIntracranial hemorrhageNervous system disordersBlood and lymphatic systemdisordersHepatobiliary disordersGastrointestinal disordersInjury poisoning andprocedural complicationsCardiac disordersImmune system disordersInfusion related reactionReproductive system and breast Testicular oedemadisordersTesticular painHypoxiaRespiratory thoracic andmediastinal disordersSkin and subcutaneous tissuedisordersPleural effusionPulmonary arterialhypertensionMaculovesicular rash15
REFERENCES1. Elia L, Mancini M, Moleti L, et al. A multiplex reverse transcriptase-polymerase chain reaction strategyfor the diagnostic molecular screening of chimeric genes: a clinical evaluation on 170 patients withacute lymphoblastic leukemia. Haematologica 2003;88:275-279.2. Van der Velden, Cazzaniga G, Schrauder A, et al. Analysis of minimal residual disease by Ig/TCR generearrangements: guidelines for interpretation of real-time quantitative PCR data. Leukemia2007;21:604-611.3. Pfeifer H, Cazzaniga G, van der Velden VHJ, et al. Standardisation and consensus guidelines forminimal residual disease assessment in Philadelphia-positive acute lymphoblastic leukemia (Ph ALL)by real-time quantitative reverse transcriptase PCR of e1a2 BCR-ABL1. Leukemia 2019;33:1910-1922.4. Soverini S, Martinelli G, Amabile M, et al. Denaturing-HPLC-based assay for detection of ABLmutations in chronic myeloid leukemia patients resistant to Imatinib. Clin Chem2004;50:1205-1213.5. Chiaretti S, Vitale A, Elia L, et al. Multicenter total therapy GIMEMA LAL 1509 protocol for de novoadult Ph acute lymphoblastic leukemia (ALL) patients. Updated results and refined genetic-basedprognostic stratification. Blood 2015;126:81.6. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap) – A metadata-drivenmethodology and workflow process for providing translational research informatics support. J BiomedInform 2009;42:377-381.7. Harris PA, Taylor R, Minor BL, et al. The REDCap Consortium, The REDCap consortium: buildingan international community of software partners. J Biomed Inform 2019;95:103208.16
Euro-MRD Consortium.2,3 All Q-RT-PCR reactions were performed on a 7500 fast ABI . Amplicons were separated on an ABI-Prism 3130 sequencer and analyzed . 6 by GeneMapper 4.0 software (Applied .