Transcription
8/29/2013WelcomePlease stand by. We will begin shortly.Needs Assessment: Tobacco DependenceEducation in Graduate Psychiatric Nursingand Pharmacy SchoolsWednesday, August 28, 2013 · 1pm Eastern Time (75 minutes)Needs Assessment: Tobacco DependenceEducation in Graduate Psychiatric Nursingand Pharmacy SchoolsWebinar objectives Provide an overview of tobacco use among personsexperiencing psychiatric and substance use disorders Assess the state of tobacco dependence education fortraining psychiatric nurses and psychiatric pharmacistsin the United States Identify at least three available resources to helppsychiatric nurses, psychiatric pharmacists, and otherproviders help patients quit smoking1
8/29/2013ModeratorCatherine Saucedo Deputy Director,Smoking Cessation LeadershipCenter, University of California,San Franciscocsaucedo@medicine.ucsf.eduAgenda Welcome– Catherine Saucedo, Deputy Director, SCLC, moderator Overview– Judith J. Prochaska, PhD, MPH Presentations– Karen S. Hudmon, DrPH, MS, RPh– Daryl Sharp, PhD, PMHCNS-BC, NPP– Susan W. Blaakman, PhD RN NPP-BC– Rhonda Schwindt, DNP, RN Questions and Answers Closing RemarksDisclosure: Faculty speaker, moderator, and planning committee members have disclosed no financial interest/arrangement or affiliation with any commercial companieswho have provided products or services relating to their presentation or commercial support for this continuing medical education activity.2
8/29/2013Housekeeping All participants will be in listen only mode. Please make sure your speakers are on and adjustthe volume accordingly. If you do not have speakers, please request thedial-in via the chat box. This webinar is being recorded and will be availableon the SCLC website, along with the slides. Send questions to the chat box at any time for thepresenters.Needs Assessment: Tobacco DependenceEducation in Graduate Psychiatric Nursingand Pharmacy SchoolsPresenters Judith J. Prochaska, PhD, MPH, Associate Professor of Medicine, StanfordPrevention Research Center, Department of Medicine, Stanford University Karen S. Hudmon, DrPH, MS, RPh, Professor and Associate Head for Operations,Department of Pharmacy Practice, Purdue University College of Pharmacy Daryl Sharp, PhD, PMHCNS-BC, NPP, Associate Dean for Faculty Development &Diversity in the School of Nursing, Professor of Clinical Nursing & in the Center forCommunity Health, University of Rochester Susan W. Blaakman, PhD RN NPP-BC, Associate Professor of Clinical Nursing,Specialty Director, Family PMHNP Program, University of Rochester Rhonda Schwindt, DNP, RN, Clinical Assistant Professor, Department ofCommunity & Health School of Nursing, Indiana University3
8/29/2013Today’s speakerJudith J. Prochaska, PhD, MPH Associate Professor of Medicine, StanfordPrevention Research Center, Departmentof Medicine, Stanford UniversityAttention to Tobacco inPsychiatric Practice & Training:What is Needed?Judith J. Prochaska, PhD, MPHAssociate Professor of MedicineStanford Prevention Research Center4
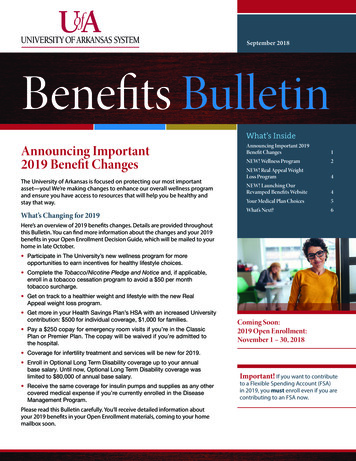
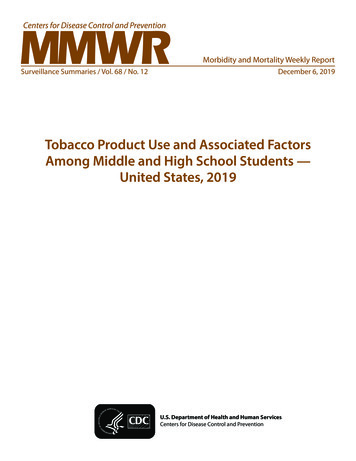
8/29/2013TRENDS in ADULT SMOKING,by SEX: U.S., 1955–20116050Male19% of adults arecurrent smokers4031.7%Percent30Female2021.6%18.3%18.8%US RegisteredNursesUS 319871991199516.5%1999200320072011Year70% want to quitGraph provided by the Centers for Disease Control and Prevention. 1955 Current PopulationSurvey; 1965–2010 NHIS. Estimates since 1992 include some-day smoking.SMOKING PREVALENCE byPSYCHIATRIC DIAGNOSISPanic DisorderPTSD100%41.0% Overall90%GADDysthymia80%70%Major Depression60%Bipolar Disorder50%30%Nonaffect Psychosis34.8%40%ASPD22.5%Alcohol Abuse/Dep20%10%Drug abuse/dep0%NoneHistoryActiveNational Comorbidity Survey 1991-1992Source: Lasser et al., 2000 JAMA5
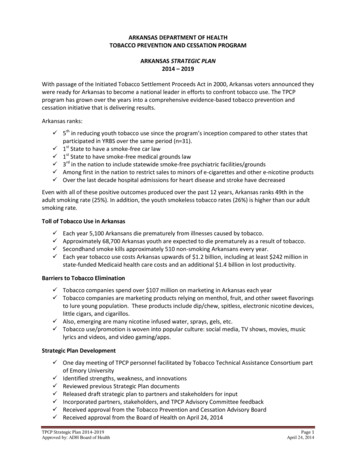
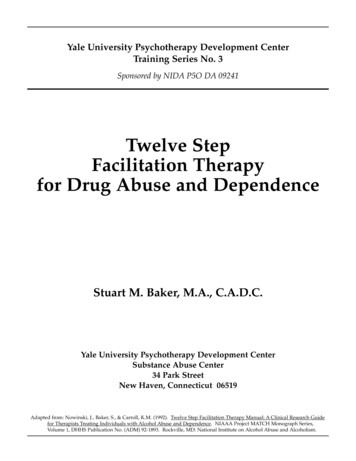
8/29/2013SMOKING & MENTAL ILLNESS:1991-92, 2000-01, 2001-03, 2009-112000‐20012001‐20032009‐2011% Current Smokers1991‐1992National ComorbiditySurvey, Lasser et al.JAMA 2000Healthcare forCommunities surveyOng et al. AJPH 2010National Survey ofAmerican Life, Hickmanet al. NTR 2010CDC Vital SignsMMWR, 2012SMOKING in PSYCHIATRY:ADULTS in SAN FRANCISCO, CACigarettes/dayM(SD)County Psych Inpatient60%45% 21 (15)Private Psych Inpatient28%Private Psych OutpatientSF Adults17 (12)14%15Acton, Prochaska, Kaplan, Small & Hall. (2001) Addict BehavBenowitz, Schultz, Haller, et al. (2010) Am J EpiProchaska, Gill, & Hall. (2004) Psychiatric Services6
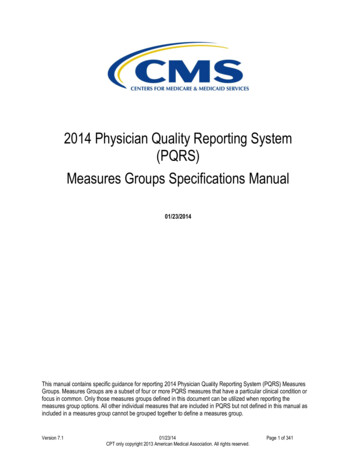
8/29/2013Tobacco Kills Individuals with mental illness die, on average, 25 yearsprematurely (Colton & Manderscheid, 2006) elevated risk for respiratory and cardiovasculardiseases and cancer, compared to age-matchedcontrols (Brown et al., 2000; Bruce et al., 1994; Dalton et al., 2002;Himelhoch et al., 2004; Lichtermann et al., 2001; Sokal, 2004). Current tobacco use is predictive of future suicidalbehavior, independent of depressive symptoms, priorsuicidal acts, and other substance use (Breslau et al., 2005;Oquendo et al., 2004, Potkin et al., 2003).COMPARATIVE CAUSES of ANNUALDEATHS in the UNITED STATES450400Individuals withmental illness orsubstance usedisorders350300250200150100500AIDSObesity AlcoholMotor Homicide Drug Suicide SmokingVehicleInducedSource: CDC7
8/29/2013PHARMACOKINETIC DRUGINTERACTIONS with SMOKINGDrugs that may have a decreased effect due to inductionof CYP1A2: CaffeineClozapine (Clozaril )Fluvoxamine (Luvox )Haloperidol (Haldol )Olanzapine (Zyprexa )Phenothiazines (Thorazine,Trilafon, Prolixin, etc.) Propanolol Tertiary TCAs / cyclobenzaprine(Flexaril ) Thiothixene (Navane ) Other medications: estradiol, mexiletene,naproxen, phenacetin, riluzole, ropinirole,tacrine, theophyline, verapamil, r-warfarin(less active), zolmitriptanSmoking cessation may reverse the effect.MAJOR TARGET MARKET Estimates that 44% to 46%of cigarettes consumed inUS by smokers withpsychiatric or addictivedisorders (Lasser, 2000;Grant, 2002) 175 billion cigarettes and 39 billion in annualtobacco sales (USDA, 2004)8
8/29/20131951ENVIRONMENTSELF‐MEDICATION BELIEFS9
8/29/2013Department of Health, Education, and WelfareNational Institute of Mental HealthWashington, DCAugust 4, 1980I am writing to request a donation ofcigarettes for long-term psychiatric patients because of recent changes in the DHHSregulations, Saint Elizabeth Hospital can nolonger purchase cigarettes for them.I am therefore requesting a donation ofapproximately 5,000 cigarettes a week (8 perday for each of the 100 patients without funds).LD 463 - An Act to Exempt SubstanceAbuse and Psychiatric Patients from theProhibition against Smoking in Hospitals10
8/29/2013HOSPITAL SMOKING BANSJCAHO ultimately “yielded to massivepressure from mental patients and theirfamilies, relaxing a policy that called onhospitals to ban smoking.”TOBACCO BANS & STATE PSYCHIATRICHOSPITALS (2005-2011)NASMHPD Surveys 2005-201111
8/29/2013SMOKING BAN TREATMENT Langley Porter, 100% smokefree since 1988 N 100 smokers 70% used NRT during hospitalization 1 patient had tobacco on their treatment plan 2 were advised to quit smoking 3 received a DSM-IV diagnosis of Nicotine Dependence orWithdrawal 4 were provided NRT at dischargeProchaska, Fletcher, Hall & Hall (2006). Am J AddictionsRETURN to SMOKING: SMOKE-FREEACUTE PSYCH HOSPITALFREE NRT1‐800‐QuitNowProchaska, Fletcher, Hall & Hall (2006). Am J Addictions12
8/29/20132006 AAMC Practice Survey: Psychiatrists 62% Ask about tobacco & Advise to quit 44% Assess readiness to quit 13-23% Assist NRT (23%), other Rx (20%), cessation materials (13%) 14% Arrange follow up 11% Refer to othersPsychiatrists least likely to address tobacco use withtheir patients relative to other specialties (familymedicine, internal medicine, OB/GYN)SMOKERS with BIPOLAR DISORDER:ONLINE SURVEY (N 685) Few reported a psychiatrist (27%), therapist(18%), or case manager (6%) ever advisedthem to quit smokingSeveral reported discouragement toquit from mental health providersProchaska, Reyes, Schroeder, et al. (2011). Bipolar Disorders13
8/29/2013Top Barriers to Treating Tobacco2006 AAMC Survey with 701 Psychiatrists 89% -- Patients not motivated to quit 83% -- More acute problems to address 80% -- Few cessation programs available 75% -- Patients usually fail to quit 72% -- Other practice priorities 65% -- Staff are unfamiliar with tobacco treatments 61% -- Limited time with patients 58% -- Lack of provider knowledge in tobacco cessationJust as Ready to Quit Smoking as theGeneral PopulationIntend to quit in next 6 moGeneral Population40%General Psych Outpts43%(Acton et al., 2001 Addict Bx)Depressed Outpatients(Prochaska et al., 2004, Drug Alc Dep)Psych. InpatientsIntend to quit in next 30 days20%28%55%24%41%24%(Prochaska et al., 2006, Am J Addict)Methadone Clients48%22%(Nahvi et al., 2006, Addict Bx)0%20%40%60%80%100%* No relationship between psychiatric symptom severity and readiness to quit14
8/29/2013TREATING DEPRESSED OUTPATIENTS &PSYCHIATRIC INPATIENTS Efficacious for smokerswith clinical depressionComparison of Stage- Tailored Trials(N 322)18 month abstinence rates Efficacious for smokers30%hospitalized for severe24.6%23%mental illness (N 224)20.4%20% 19.1% Comparable quitting to15%16%general population8%7.7% No harm to mental healthrecovery0%Inpt Psych Depress Outpt Gen Pop Comparable effects in aControlInterventiondiverse sample (N 100)Hall et al. (2006) AJPH; Prochaska et al. (2008) AJPH; Prochaska et al. (2013) AJPHAddressing Barriers toTreating Tobacco in Psychiatry Psychiatric patients are motivated to quit smoking Tobacco use is deadly and relevant to psychiatric care Cessation programs and brief referrals are available Psychiatric patients can quit smoking and without harmto their mental health recovery or sobriety Training programs exist, are being disseminated, andhave been well received15
8/29/2013Today’s speakerKaren S. Hudmon, DrPH, MS, RPh Professor and Associate Head forOperations, Department of PharmacyPractice, College of Pharmacy,Purdue UniversityKaren S. Hudmon, Dr.P.H., M.S., R.Ph.Professor, Purdue University College of PharmacyResearch Affiliate, Yale University School of Public HealthAssistant Clinical Professor, UCSF School of Pharmacy16
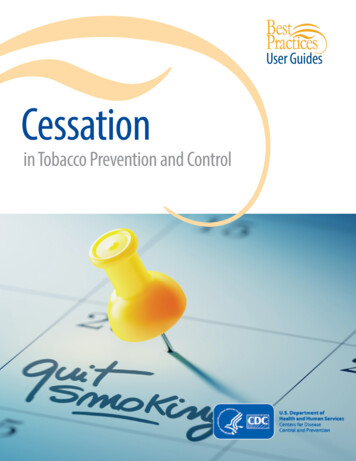
8/29/2013Estimated abstinenceAt 5 monthsn 29 studies2.2(1.5,3.2)1.7(1.3,2.1)1.01.1(0.9,1.3)Type of clinicianFiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. 2008 Update.USDHHS, PHS, 2008.17
8/29/2013 Do nothingMinimal intervention Ask, Advise, ReferThe 5 A’s approach Comprehensive tobacco cessationcounseling, with follow-upAre clinicians trained to help patients quit smoking?Are clinicians interested in helping patients quit smoking?Tobacco Content inPharmacy School Curricula National survey, 98.8% response (n 82)Median, 170 total min of required tobacco contentduring 3-5 years of pharmacy trainingMost heavily emphasized topics: Aids for Quitting Assisting Patients with Quitting Pharmacology of Nicotine & Principles of Addiction Drug Interactions with SmokingHudmon et al. Tobacco education in U.S. schools of pharmacy.Nicotine & Tobacco Research 2005;7:225-232.18
8/29/2013 Fewer than 9% have received formal training88% are interested in receiving training93% believe it will improve the quality oftheir counseling70% believe it will increase the numberpatients whom they counselTraining is associated with counseling.Self-efficacy is more important than training.Hudmon et al. Patient Education & Counseling, 2006.19
8/29/2013http://rxforchange.ucsf.eduRx for Change:Faculty Participant bilityfor integrationComprehensivenessof contentComprehensiveAppropriateness ofAppropriatenessteaching methodsConfidence in skillsfor teachingRxFCConfidencein skills ------- 67.1% ------ Likelihood ofLikelihoodadoption inofupcomingadoptionyr0%20%40%60%80%100%Percent of total responsesN 191 faculty20
8/29/2013 69 of 85 schools implemented (81%)Median, 270 minutes of tobacco education 100 minutes (59%) over baseline (2001-02)Nearly 8,000 students were exposed to all orportions of the program89% integrated the program materials intothe core (required) curriculumPharmacy is the only discipline that has attemptedsystematic, nationwide integration of tobacco educationin the core curriculum.Versions available: 5 A's (comprehensive counseling) Ask-Advise-Refer (brief counseling) Psychiatry Cancer Care Providers Cardiology Providers Mental Health Peer Counselors Surgical Providers97 new users register on the site each month.Users represent 46 countries and all 50 U.S. states.21
8/29/2013Versions available: 5 A's (comprehensive counseling) Ask-Advise-Refer (brief counseling) Psychiatry Cancer Care Providers Cardiology Providers Mental Health Peer Counselors Surgical Providers97 new users register on the site each month.Users represent 46 countries and all 50 U.S. states.22
8/29/2013Pharmacy: UCSF/PurdueNursing: Georgetown Univ. (Janie Heath)Psychiatry: Western U.S. (Jodi Prochaska)Baseline surveys: Physician Assistant programs Respiratory Care programs GlaxoSmithKline Dental schools, health systems, other Many other initiatives have focused on licensed clinicians. Provide widespread access to evidencebased training tools for all disciplines Health professional studentsLicensed clinicians Updated frequently Available at no cost Remain free of pharmaceutical industryinfluence and bias 1999 - ?23
8/29/2013Today’s speakerDaryl Sharp, PhD, PMHCNS-BC, NPP Associate Dean for Faculty Development &Diversity in the School of Nursing, Professorof Clinical Nursing & in the Center forCommunity Health, University of RochesterToday’s speakerSusan W. Blaakman, PhD, RN NPP-BC Associate Professor of Clinical Nursing,Specialty Director, Family PMHNP Program,University of Rochester24
8/29/2013Today’s speakerRhonda Schwindt, DNP, RN Clinical Assistant Professor, Department ofCommunity & Health School of Nursing,Indiana University“Needs Assessment: Tobacco DependenceEducation in Graduate Psychiatric Nursingand Pharmacy Schools”August 28, 201325
8/29/2013State of Tobacco DependenceEducation in Nursing CurriculaUniversity of Rochester:Daryl Sharp & Susan BlaakmanIndiana University:Rhonda SchwindtDrs. Sharp, Blaakman & Schwindt have no conflicts of interest to disclose.THANK YOU!!! SCLC for sponsoringthis webinar today. All of you for joining usin this conversation, sowe can learn more fromyou about where to gofrom here to improveformal tobaccodependence education.26
8/29/2013Objectives Review the literature pertinent to tobacco education andnursing curricula Describe national tobacco dependence survey data(American Psychiatric Nurses Association, 2008 and2012) Identify probable reasons behind why there is so littletobacco dependence content in PMH nursing curricula Engage webinar participants in discussionLITERATURE REVIEWTobacco Education & Nursing Curricula Most BSN nursing programs devote less than 2 hours of teaching timeto tobacco use & dependence (many offer less than 1 hour)(Heath &Crowell, 2007; Sarna et al., 2009; Sharp, Blaakman et al., 2009). Few offer material on clinical cessation techniques or require anyclinical experience (Hornberger & Edwards, 2004; Wewers, Kidd, Ambruster, & Sarna, 2004;Sarna et al., 2009) Rarely a required component of nursing curricula (Heath & Crowell, 2007;Sarna et al., 2009; Sharp, Blaakman et al., 2009). Mental health professionals (including psychiatric nurses) report thattheir educational programs did not prepare them to provide tobaccotreatment (Williams et al., 2009). Nurses that are less knowledgeable are less confident and thus lessmotivated to intervene with their clients who smoke (Sharp, Blaakman et al., 2009). Educational programs offer an ideal time to provide training in tobaccodependence treatment (Clark, McCann, Rowe, & Lazenbatt, 2004).27
8/29/2013LITERATURE REVIEWKnowledge, Attitudes, & Practices Vast majority of nurses do not engage in tobacco cessation interventions & fewconsider it a priority (Sharp, Blaakman et al., 2009).Nurses at all practice levels frequently fail to progress beyond advising theirclients to quit and few offer any advice to their clients who smoke (Fiore et al.,2008). Psychiatric nurses with higher levels of self-reported confidence and motivationare more likely to engage in cessation interventions &/or refer their clients tocessation resources (Sharp, Blaakman et al., 2009).Tobacco education holds forth the promise of short-term positive effects(lack oflong-term follow-up) (Kelley et al., 2006; Sheffer et al., 2010; J. Williams et al., 2009)Absence of standardized format or curriculum for training healthcare providers(Barta & Stacy, 2005; Kelley et al., 2006; Kerr et al., 2011; Prochaska et al., 2008; Sheffer et al., 2010;Sohn et al., 2011; Williams, J. M., et al., 2009).APNA Tobacco Dependence Survey2008 & 2012 Design: Cross sectional analysis of 29-itemonline survey; 40-items in 2012 Sample: APNA members accessible by email Measures: Anonymous, Survey Monkey– 10-15 minute completion time– 2008, 2 email reminders;– 2012, 3 email reminders Member Bridge/conference(Sharp, Blaakman et al., 2009)28
8/29/2013200820124000 emailed; 1365 responded 7500 emailed; 1061 responded– 31.6% response rate– 14% response rate45% 20 yrs PMH RN;17.2% 5 yrs45% 20 yrs PMH RN;24% 5 yrs35% BSN; 54.5% MS;9.6% PhD/DNP22% BSN; 53% MS;12% PhD/DNP/DNSc23% Staff RN; 32.4% APN;17.3% Faculty28% Staff RN; 47% APN;23% Faculty42.8% Inpatient; 33%Outpatient; 17.3% Faculty42% Inpatient; 32% Outpatient;11% College/University(Sharp, Blaakman et al., 2009)(*data not yet published)Nurses’ Smoking Status2008201229
8/29/2013Smoke-Free Workplace20082012Necessary Part of Recovery from MI orAddictive Disorders?2008201230
8/29/2013Hours Spent on Tobacco Dependence:Undergraduate Curricula20082012Hours Spent on Tobacco Dependence:Graduate Curricula2008201231
8/29/2013Tobacco Dependence Training2012Brief Interventions by Nurses2008201232
8/29/2013Intensive Interventions by Nurses20082012*Findings/Implications Nurses reported relatively high knowledge(meds, counseling, resources) but lackedconfidence in ability to help & in clients’ abilitiesto reduce/quit smoking Nurses asked & advised but did not consistentlyrefer or provide intensive interventions Nurses less likely to intervene if not confident*(Sharp, Blaakman et al., 2009)33
8/29/2013Findings/Implications Tobacco dependence education including strategies toenhance motivation needed to enhance nurses’efficacy/confidence Respondents more likely interested in topic but ¼ did notrate it as a work priority Per NASMHPD (Mauer, 2008): Cardiac deathsoutnumber suicides among those with mental illnessbut smoking assessment/intervention less likely tobe routine(Sharp, Blaakman et al., 2009)Findings/Implications Increasing value of tobacco dependence interventions isvital to support wellness/recovery & denormalizationefforts Workplace values impact nurses We must work collaboratively to strengthen ourintervention skills and public voices to advocate forsmoking cessation among ourselves & thoseentrusted to our care(Sharp, Blaakman et al., 2009)34
8/29/2013Why so little TD content in graduatePMH nursing curricula? Too much other content to cover Not required on certification exams Not adequately linked to master’s essentials,NONPF NP core competencies, NLN nurseeducator core competencies, PMHNP scope& standards Faculty underskilled to teach Is this right? What is missing? How do we address?Priorities/Future DirectionsFocus on nursing education:What do YOU think ?35
8/29/2013What we can do “If we are going to be part of the solution, wehave to let go of the idea that change doesn’thappen unless we’re around to see it.” “We matter and we don’t; what each of us doesmay not seem like much, because in importantways, it isn’t much. But when many people dothis work together they can form a critical massthat is anything but insignificant, especially in thelong run.”(Johnson, 2006, p.131-132)Questions and answers Feel free to submitquestions via thechat box36
8/29/2013Contact SCLCfor technical assistanceThanks to the support of SAMHSA,free CME/CEUs of up to 1.25 creditsare available to all attendees.Instructions will be emailed after thewebinar.Visit us online http://smokingcessationleadership.ucsf.eduCall us toll-free 1-877-509-3786Closing remarks Please help us by completing the postwebinar survey. Thank you for your continued efforts tocombat tobacco. Stayed tuned for SCLC’s next webinaron Tuesday, September 24th at 2pm ET,“8 and Counting: SAMHSA State Summitsfor Smoking Cessation Foster Change.”37
8/29/2013Poll Questions1.Are you a faculty member at:A graduate psychiatric nursing programPsychiatric residency programSchool of pharmacyOther:Not a faculty member2.Total Number4112813Total %11%3%32%21%34%About how many hours of tobacco cessation training does your program provide?0 hours1-2 hours3-4 hours5-6 hoursMore than 6 hoursTotal Number1016469Total %22%36%9%13%20%Poll Questions3.Do you cover pharmacotherapy for treating tobacco dependence in your curriculum?YesNo4.Total Number3513Total %73%27%Do you cover counseling re: tobacco dependence treatment in your curriculum?YesNoTotal Number347Total %83%17%38
8/29/2013Poll Questions5.What do you perceive to be the primary barrier to implementing tobacco education atyour institution?Faculty is very busy and pulled in several directionsFinding class time to incorporate the trainingOrganization of the material and the time and resources to incorporate it into the curriculumProgram evaluationUnsure at this timeOther6.Total Number61673136Total %12%31%14%6%25%12%How interested would you be in having your school participate in a dissemination grant toincrease attention to tobacco use in psychiatry training programs?Count me in!A littleNot sureNot veryNot at allTotal Number2210913Total %49%22%20%2%7%39
ADULTS in SAN FRANCISCO, CA 60% 14% 28% 45% SF Adults Private Psych Outpatient Private Psych Inpatient County Psych Inpatient Acton, Prochaska, Kaplan, Sma ll & Hall. (2001) Addict Behav Benowitz, Schultz, Haller, et al. (2010) Am J Epi Prochaska, Gill, & Hall. (2004) Psychiatric Services Cigarettes/day M(SD) 21 (15) 17 (12) 15