Transcription
Tennessee Annual Stroke Registry 2019.VAm .encanHeartAssoc,at onencanStrokeAssocla11onlife is why·
ACKNOWLEDGEMENTSEast Tennessee State UniversityCollege of Public HealthRandy Wykoff, MD, MPH & TMDean of the College of Public HealthDepartment of Biostatistics and EpidemiologyMegan Quinn, DrPH, MSc.Tennessee Stroke Registry ManagerKelsi McKamey, BATennessee Stroke Registry Graduate AssistantAmerican Heart Association/American Stroke AssociationKaley Pelton, MPH, RT(R)Director, Quality & Systems Improvement, Greater Southeast Affiliate2
TABLE OF CONTENTSAcknowledgements 2Executive Summary 4Map of Certified Stroke Centers with 30, 60, and 90 Minute Service Areas Error!Bookmark not defined.List of Certified Stroke Centers by Certification 5Overview of Certified Stroke Centers 7Stroke Centers by Tennessee Department of Health (TDH) Region and Metro Counties 72019 Tennessee Stroke Registry Data and Interpretation 8Variable Descriptions 9Diagnosis 11Gender Distributions 12Age Distributions 13Race 15Co-morbidities 16Arrival Mode 17Last Known Well to Arrival times 19Last Known Well to IV r-tPA Initiation 20Insurance status 22Quality Measures 23Time to Intravenous Thrombolytic Therapy 25Reasons for no IV rt-PA 27Reasons for Delay of IV rt-PA Beyond 60 Minutes 28Modified Rankin Scale at Discharge 29Complication Types 31Initial Exam findings 32Average Length of Stay 33GTWTG/PAA Defect Free 33CDC/COV Defect Free 34Limitations to data presented in this report 35How To Participate in GWTG-Stroke 36References 373
EXECUTIVE SUMMARYThe Tennessee Stroke Registry (TSR) was created in 2009 through the TennesseeStroke Registry Act of 2008. In July 2017, the legislation was updated with Tennessee HouseBill 123, requiring all certified comprehensive and primary stroke centers in Tennessee toshare their data with the TSR in order to improve stroke care in the state. The bill requiresdata to be provided from hospitals on a quarterly basis through the American HeartAssociation’s Patient Management Tool , provided by the Quintiles Real World & LatePhase Research. This report provides a summary of the TSR data, obtained throughQuintiles software, for January through December 2019. Analyzed in this report areaggregate data from the 39 hospitals that reported to the Tennessee Stroke Registry during2019, along with observations on 2018 data.4
List of Certified Stroke Centers by CertificationJoint Commission Certified Hospitals*CertificationAcute Stroke Ready HospitalAcute Stroke Ready HospitalAcute Stroke Ready HospitalAcute Stroke Ready HospitalAcute Stroke Ready HospitalAcute Stroke Ready HospitalAcute Stroke Ready HospitalAdvanced Comprehensive StrokeCenterAdvanced Comprehensive StrokeCenterAdvanced Comprehensive StrokeCenterAdvanced Comprehensive StrokeCenterAdvanced Comprehensive StrokeCenterAdvanced Comprehensive StrokeCenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterOrganization NameClaiborne Medical CenterCampbell County HMA, LLCMountain States Health AllianceBallad Health dba Sycamore Shoals HospitalMetro Knoxville HMA LLCJefferson County HMA, LLCTennova Newport Medical CenterCityTazewellLa FolletteJohnson CityElizabethtonPowellJefferson CityNewportTriStar Skyline Medical CenterNashvilleBallad Health**Johnson CityFort Sanders Regional Medical CenterKnoxvilleSaint Thomas West HospitalNashvilleVanderbilt University Medical CenterNashvilleThe University of Tennessee Medical CenterLeConte Medical CenterJackson-Madison County General HospitalAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterTriStar Hendersonville Medical CenterVanderbilt Wilson County HospitalSumner Regional Medical Center, LLCRoane Medical CenterBristol Regional Medical CenterTriStar Summit Medical CenterMemorial Health Care System, Inc.Parkridge Medical Center, Inc.Maury Regional HospitalCookeville Regional Medical CenterCumberland Medical CenterFort Loudoun Medical CenterBlount Memorial Hospital, Inc.Baptist Memorial Hospital - MemphisMorristown-Hamblen Hospital AssociationSaint Thomas Rutherford HospitalSaint Thomas Midtown HospitalMethodist Medical Center of Oak RidgeNorthCrest Medical CenterParkwest Medical CenterMetro Knoxville HMA noogaColumbiaCookevilleCrossvilleLenoir eOak RidgeSpringfieldKnoxvillePowell
Advanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Primary Stroke CenterAdvanced Thrombectomy CapableStroke CtrStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationStroke RehabilitationWellmont Health SystemTriStar Centennial Medical CenterTriStar Southern Hills Medical CenterTriStar Horizon Medical CenterTriStar StoneCrest Medical CenterSaint Francis Hospital - rtlettSaint Francis Hospital-MemphisSiskin Hospital for Physical RehabilitationEncompass Health Rehabilitation Hospital ofKingsport, LLCRebound, LLCTriStar Horizon Medical CenterEncompass Health Rehabilitation Hospital ofMemphisEncompass Health CorporationEncompass Health Methodist RehabilitationHospital, LPWest Tennessee Rehabilitation Hospital, LLCWest Tennessee Rehabilitation Hospital, LLCEncompass Health Rehabilitation Hospital ofFranklin, LLCQuillen Rehabilitation Hospital of Johnson nson City*This list was last updated on April 7, 2020. The most up-to-date listing of certified stroke centers canbe found on The Joint Commission website or American Heart/American Stroke Association website.**Includes Ballad Health, Johnson City Medical Center and Ballad Health Holston Valley MedicalCenterDNV-GL Certified Hospitals*Organization NameCityCountyErlanger Health SystemMethodist Le BonheurMethodist Medical Center,NorthMethodist Medical tification programAdvanced Comprehensive StrokeCenterAdvanced Primary Stroke CenterMemphisShelbyAdvanced Primary Stroke CenterMemphisShelbyMethodist University HospitalMemphisShelbyAdvanced Primary Stroke CenterAdvanced Comprehensive StrokeCenter*This list was last updated on April 26, 2020. The most up-to-date listing of stroke certification of these hospitalscan be found on the Methodist Le Bonheur Healthcare website: /neurology-neurosurgery/stroke-center/.6
OVERVIEW OF CERTIFIED STROKECENTERSStroke Centers by Tennessee Department of Health (TDH) Region andMetro ,arlotteGreenvillekColumbiaAtlantaBirminghamMap of TDH Regions7Northeast and Sullivan Metro:Southwest, and Shelby and Madison Metro:Ballad HealthBaptist Memorial HospitalBristol Regional Medical CenterJackson-Madison County GeneralHolston Valley Medical CenterHospitalJohnson City Medical CenterMethodist University HospitalsSycamore Shoals HospitalSaint Francis Hospital BartlettEast and Knox Metro:Saint Francis Hospital MemphisBlount Memorial HospitalMid-Cumberland and Davidson Metro:Campbell County HMA, LLCNorthCrest Medical CenterFort Sanders Regional Medical CenterMorristown-Hamblen HospitalFort Loudon Medical CenterAssociationJefferson County HMA, LLCRoane Medical CenterParkwest Medical CenterSouthern Hills Medical CenterLeConte Medical CenterSt. Thomas Midtown HospitalMethodist Medical Center Oak RidgeSt. Thomas Rutherford HospitalNewport Medical CenterSt. Thomas WestNorth Knoxville Medical Center (Tennova)StoneCrest Medical CenterTurkey Creek Medical (Tennova)Sumner Regional Medical CenterUniversity of Tennessee Medical CenterTennova Healthcare-LebanonSoutheast and Hamilton Metro:TriStar Centennial Medical CenterErlanger Health SystemTriStar Hendersonville MedicalMemorial Healthcare SystemCenterParkridge Medical CenterTriStar Horizon Medical CenterSouth-Central:Tristar Skyline Medical CenterMaury Regional HospitalTriStar Summit Medical CenterVanderbilt University Medical CenterUpper-Cumberland:Cookeville Regional Medical Center
2019 TENNESSEE STROKE REGISTRYDATA AND INTERPRETATIONThe following charts and tables represent aggregate data from the 39 hospitalsreporting to the Tennessee Stroke Registry in 2018 through 2019 with data from January toDecember of each year. All cases of strokes are reported including transient ischemic attack(TIA) patients, unless otherwise stated. Data were obtained from Quintiles on April 1, 2020.Illustrations are made on similarities and differences between 2018 and 2019 data.8
Variable Descriptions*MeasureNumeratorAgePatients in specific age groupsCo-morbiditiesTransportation timesNIHSS reportedTime to IntravenousThrombolytic TherapyReasons for no IV-rtPAReasons for no IV-rtPAbeyond 60 minModified Rankin Scale atdischargeComplication types9Patients with co-morbidityDenominatorPatients with a diagnosis ofIschemic stroke, TIA,Subarachnoid hemorrhage, orIntracerebral hemorrhageAll patientsPatients arriving in time intervalPatients with a diagnosis ofIschemic stroke, TIA,Subarachnoid hemorrhage,Intracerebral hemorrhage, orStroke not otherwise specifiedNIH Stroke scale performed as Patients with a diagnosis ofpart of initial evaluation ANDIschemic stroke or Stroke notTotal Score is reportedotherwise specifiedPatients in time intervals based Patients with a primary strokeon time from patient arrival atdiagnosis of ischemic strokethe ED to time of administration who received IV t-PA at myof IV t-PAhospitalPatients with a primary strokePatients in exclusion criteriadiagnosis of ischemic strokegroupwho arrived at the ED 270minutes after the onset ofstroke symptoms and hadreason(s) why IV t-PA was notstarted at my hospitalPatients with a primary strokePatients grouped by reasondiagnosis of ischemic stroke inwhom IV tPA was initiatedgreater than 60 minutes afterhospital arrivalPatients with a diagnosis ofPatients in each ModifiedIschemic Stroke orRankin Scale at dischargeSubarachnoid Hemorrhage orvalueIntracerebral Hemorrhage orStroke not otherwise specifiedPatients with a primary strokePatients in each of the 4diagnosis of ischemic strokecombination groups (therapywho received IV t-PA or intrareceived versus complicationarterial thrombolytic therapy atexperienced)my hospitalInitial exam findingsPatients grouped by examfindingLength of stayPatients grouped by stroketypePatients with a diagnosis ofIschemic Stroke or TIA orSubarachnoid Hemorrhage orIntracerebral Hemorrhage orStroke not otherwise specifiedAll patients
GWTG/PAA Defect FreeAll patients which wereincluded in the numeratorfor all of the measures thatthey were not excluded fromAll patients which are includedin the denominator for at leastone of these measures: CDC/COV Defect FreeAll patients which wereincluded in the numeratorfor all of the measures thatthey were not excluded fromIV rt-PA 2 HourEarly AntithromboticsVTE Prophylaxis (forpatients discharged on orafter 4/7/2012)DVT Prophylaxis (GWTGHistoric) (for patientsdischarged before4/7/2012)Antithrombotics*Anticoag for AF*LDL 100 or ND-Statin *Smoking CessationAll patients which are includedin the denominator for at leastone of these measures: IV rt-PA 2 HourEarly AntithromboticsVTE ProphylaxisAntithromboticsAnticoag for AFLDL 100 or NDSmoking CessationDysphagia ScreenStroke EducationRehabilitation Considered*Percentages in graphs are based on the number of cases per year, unless otherwise specified10
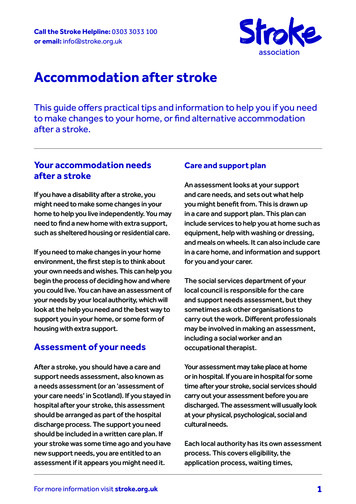
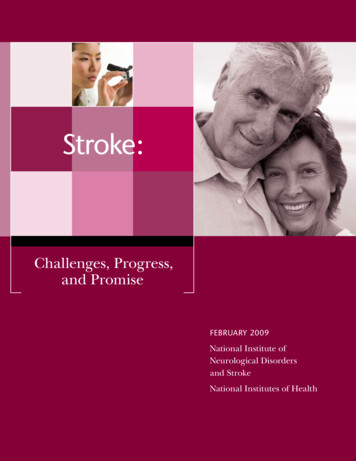
DiagnosisStroke Diagnosis 2019 (n 14908)69%Ischemic stroke8%5%Transient ischemic attack( 24 hours)Subarachnoid Hemorrhage12%Intracerebral HemorrhageFigure 1. Distribution of stroke diagnosis in 2019.Overall, the patterns and distributions for 2019 are similar to what was seen inprevious years. The total number of stroke cases reported for 2019 was 14,908. The mostcommon cases were ischemic strokes at 10,315 (69%) of strokes reported to the registry.Hemorrhagic strokes, which include subarachnoid hemorrhage (SAH), and intracerebralhemorrhage (ICH) together composed 17% of cases. There were 1,848 ICH, 699 SAH, and1,199 transient ischemic attacks reported.11
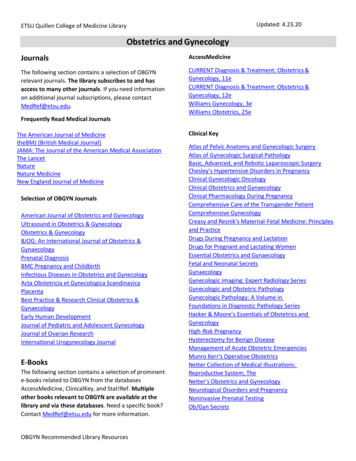
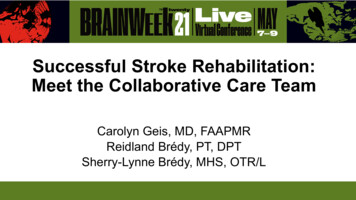
Gender DistributionsGender Distribution Across Stroke Types for 2019 and 2018 Male Female100%90%80%47%48%49%49%70%65%64%35%36%SAH 2019(n 699)SAH 2018(n 617)54%55%46%45%TIA 2019(n 1199)TIA 2018(n 814)60%50%40%30%53%52%51%51%20%10%0%ICH 2019(n 1848)ICH 2018(n 1716)Ischemic 2019 Ischemic(n 10312) 2018(n 9124)Figure 3. Distribution of stroke by gender in 2019 and 2018.Gender distributions were consistent with data from 2019, with similar percentages ofmale and female cases for ischemic stroke, and slightly higher percentages of female casesfor TIA (54% versus 46%) and similar proportions of male and female cases of ICH (52%versus 48%). The gender differences in strokes were more pronounced for subarachnoidhemorrhage than they were in 2018, but the difference between 2018 and 2019 was notsignificant (z -1.279, p .201).12
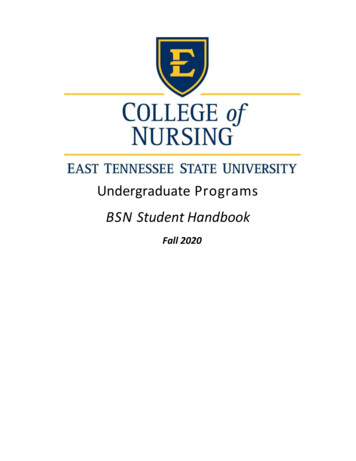
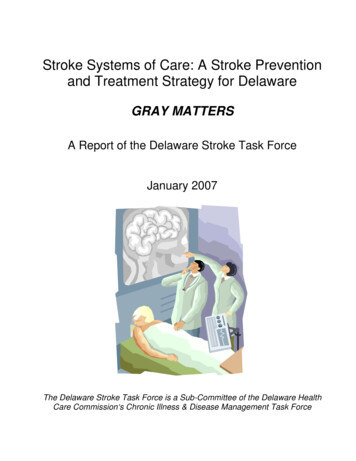
Age DistributionsAge Distribution AmongIschemic Stroke Patients(n 10315)Age Distribution Among TIApatientsn 119918 - 456%18 - 457% 8511% 8511%46 - 6534%66 - 8549%66 - 8554%Age Distribution among SAHPatients(n 699) 855%66 - 8532%r18 - 4518%46 - 6545%Figure 4. Age distribution for all stroke types in 2019.1346 - 6528%Age Distribution Among ICHPatients(n 1848)18 - 459% 858%66 - 8548%46 - 6535%
Average Ages of Stroke Subtypes /- 1 Standard Deviation807060504030201067.668.1696066.4All strokeIschemicTIASAHICH0 2019Figure 5. Distribution of mean age and one standard deviation of stroke patients for all stroketypes in 2019.SAH cases had a younger mean age (60.0) than other types of stroke. The mostcommon age group experiencing ischemic strokes were those from ages 66-85, with 48% ofall cases in this bracket. This pattern was similar for all stroke types except SAH, where 48%of cases occurred in those ages 46-65.14
RaceRace Ischemic Strokesn 10315Race SAHn icity1%Black19%White80%Race ICHn te82%Asian1%Race TIAn Figure 6. Race distribution of stroke patients aged 18 and older for all stroke types in 2019.15
Co-morbiditiesTop 7 Co-morbidities Among Stroke Patients, 2018 and 2019 2018 (n 12632) 2019 (n 14770)77% 76%39% 40%34% 32%24% 25%HypertensionDyslipidemiaDiabetes MellitusPrevious Stroke23% 23%23% 23%SmokerCAD/Prior MI25%20%Obesity/OverweightFigure 7. Most common comorbidities for all stroke types in from 2018-2019.The top three co-morbidities among stroke patients in 2019 were hypertension (76%),dyslipidemia (40%), and diabetes mellitus (32%). More patients had a medical history ofobesity in 2019 than in previous years, with a prevalence rate of 25% in reported cases in2019 compared to 20% in 2018.16
Arrival ModeArrival Mode Among IschemicStroke Patientsn 10016Arrival Mode Among SAH StrokePatientsn 690Transferfrom otherhospital25%EMS fromhome/scenePrivate42%transport/taxi/other fromhomes/scene33%MobileStrokeUnit0%Arrival Mode Among ICH StrokePatientsn 1824Arrival Mode Among TIAPatientsn 1185EMS fromhome/scene30%Privatetransport/taxi/other fromhomes/scene14%Figure 8. Arrival mode for all stroke types in 2019.17Privatetransport/taxi/other fromhomes/scene13%Transferfrom otherhospital6%EMS fromhome/scene45%Transferfrom otherhospital41%Transferfrom otherhospital56%EMS fromhome/scene30%Privatetransport/taxi/other fromhomes/scene64%MobileStrokeUnit0%
Arrival Mode forAll Stroke Types 2019Mobile StrokeUnit0.2%Transfer from otherhospital26.6%EMS from home/scene41.0%Private transport/taxi/other fromhomes/scene32.2%Figure 9. Arrival mode for all stroke types in 2019.The most common mode of arrival for all strokes in 2019 was via Emergency MedicalServices (EMS) transport, with 41% of patients arriving in this manner. There was a slightlydifferent distribution of arrival mode among the stroke types, with the majority of TIA patients(32%) arriving via private transport and the majority of hemorrhagic stroke patients arrivingfrom another hospital. 48 ischemic stroke patients, two TIA and eight ICH patients arrived viaMobile Stroke Unit in 2019.18
Last Known Well to Arrival timesTime From Last Know Well to 7%5%5%8%18%13%15%Private transport/taxi/other fromhome/scene (n 4509)EMS from home/scene (n 5729)0% 0-60 min. 61-120 min. 121-180 min. 181-300 min. 300Figure 10. Last Known Well (LKW) to arrival times for all stroke types in 2019. LKW to arrivaltime is defined as the amount of time between when the patient first began experiencingstroke symptoms and their arrival at the hospital.Overall, private transport observes longer transportation times from home/scene incomparison to Emergency Medical Services (EMS) transport. Most patients arrived at thehospital in over 300 minutes via private transportation (73%), while only 53% of patients viaEMS services arrived in that time frame. Meanwhile, 15% of patients arrive to the hospital viaEMS services in less than 60 minutes.19
Last Known Well to IV r-tPA InitiationLast Known Well to IV r-tPA Initiation by Mode %40%30%42%38%4%7%EMS (n 1183)Private transport/taxi/other (n 395)20%10%0% 0-60 min. 61-120 min. 121-180 min. 181-270 min. 270Figure 11. Comparison LKW to initiation of IV r-tPA times transportation type in 2019.20
Last Known Well to IV r-tPA Initiation 2018-2019100%90%3%4%21%19%33%31%40%40%4%6%2018 (n 1338)2019 (n 1663)80%70%60%50%40%30%20%10%0% 0-60 min. 61-120 min. 121-180 min. 181-270 min. 270Figure 12. LKW to initiation of IV r-tPA times for all stroke types from 2018-2019.Of those arriving via EMS services 77.8% received treatment with tissue plasminogenactivator (IV r-tPA) within three hours compared to only 71.2% of patients arriving via privatetransport. This is important to note as three hours is generally the cutoff point for initiation ofIV r-tPA. IV r-tPA is the FDA-approved treatment for ischemic strokes.121
Insurance statusInsurance Status 2018 (n 12755) 2019 (n %Self-payFigure 13. Insurance status of patients in 2019.The majority of stroke patients had Medicare, but less than year 2018 past years with59% of patients paying with Medicare in 2018 compared with 56% in 2019. This reflects thatthe most common age group experiencing strokes are those from ages 66-85, the groupmost likely to have Medicare insurance.22
Quality MeasuresThe GWTG-Stroke program requires the following consensus measure. Descriptions are fromthe Patient Management Tool program, Quintiles. Dysphagia Screen: Percent of stroke patients who undergo screening for dysphagiawith an evidence-based bedside testing protocol approved by the hospital before beinggiven any food, fluids, or medication by mouth. Stroke Education: Percent of patients with stroke or TIA or their caregivers who weregiven education and/or educational materials during the hospital stay addressing ALLof the following: personal risk factors for stroke, warning signs for stroke, activation ofemergency medical system, need for follow-up after discharge, and medicationsprescribed. Rehabilitation Considered: Percent of patients with stroke who were assessed forrehabilitation services. Time to Intravenous Thrombolytic Therapy - 60 min: Percent of acute ischemicstroke patients receiving intravenous tissue plasminogen activator (tPA) therapy duringthe hospital stay who have a time from hospital arrival to initiation of thrombolytictherapy administration (door-to-needle time) of 60 minutes or less. LDL Documented: Percent of ischemic stroke or TIA patients with a documentedLipid profile. Intensive Statin Therapy: Percent of Ischemic stroke and TIA patients who aredischarged with Intensive Statin Therapy. IV rt-PA Arrive by 3.5 Hours, Treat by 4.5 Hours: Percent of acute ischemic strokepatients who arrive at the hospital within 210 minutes (3.5 hours) of time last knownwell and for whom IV t-PA was initiated at this hospital within 270 minutes (4.5 hours)of time last known well. NIHSS Reported: Percent of ischemic stroke and stroke not otherwise specifiedpatients with a score reported for NIH Stroke Scale (Initial)23
Quality measure20182019Dysphagia screen88.80%86.00%Intensive statin therapy80.20%89.50%IV rt-PA arrive by 3.5 hour, treat by 4.5 hour86.60%91.70%LDL documented94.60%94.80%NIHSS reported94.90%95.40%Rehabilitation considered99.10%99.40%Stroke education96.90%95.00%Time to intravenous thrombolytic therapy - 60 min90.20%88.80%Table 1. Percent of patients receiving quality measure in 2018 & 2019.There was an increase in stroke patients who were discharged with intensive statintherapy, from 80.2% in 2018 to 89.50 in 2019). In IV r-tPA treatment, there were morepatients who arrived by 3.5 hours and were treated by 4.5 hours in 2019 than in previousyears, with 91.7% of patients in 2019. There was a decrease in patients receiving intravenousthrombolytic therapy in 60 minutes or less, this occurring in 90.2% of patients in 2018 and88.80 of patients in 2019.24
Time to Intravenous Thrombolytic TherapyTime to Intravenous Thrombolytic Therapy 2018-2019100%2.36%1.98%7.18%8.67%61%58%30%30%2018 (n 1059)2019 (n 1315)90%80%70%60%50%40%30%20%10%0% 0-30 min. 31-60 min. 61-90 min. 90 min.Figure 14. Time to intravenous thrombolytic therapy from 2018-2019.25
Time to Intravenous Thrombolytic Therapy 10%11%0%Private transport/taxi/other from home/scene(n 301)EMS from home/scene (n 995) 0-30 min. 31-60 min. 61-90 min. 90 min.Figure 15. Comparison of times to intravenous thrombolytic therapy by transportation type in2019.IV t-PA was initiated within 60 minutes in 2019, at 93%. Compared to transport via EMSservices, arriving via private transport experience slightly slower times with 87% of patientsreceiving treatment in an hour versus 94.2% who arrived via EMS.26
Reasons for no IV rt-PATop Reasons for no IV rt-PA Initiation 2019n 131129%26%14%6%tPA outsidehospMild strokeAge Over 806%Acute bleeding Anticoagulantdiathesisuse7%Recent IC orspinal surgery8%UTD eligibilityFigure 16. Top seven reasons in 2019 for no IV rt-PA initiation.The percentages in the chart above represent the number of times the reason waslisted as to why IV rt-PA was not initiated, out of patients with a primary stroke diagnosis ofischemic stroke who arrived at the ED 270 minutes after the onset of stroke symptoms andhad reason(s) why IV t-PA was not started. The top reasons for no IV rt-PA initiation in 2019,in order of highest proportion of patients to lowest, were because the stroke was too mild, IVor IA tPA was given outside the hospital, acute bleeding diathesis, UTD eligibility, Recent ICor spinal surgery, and age over 80 and anticoagulant use.27
Reasons for Delay of IV rt-PA Beyond 60 MinutesReasons for IV rt-PA Initiation Beyond 60 Minutes 2019n 304 2019 (n 304)38%28%14%7%Care-team unable todetermine eligibilityHypertensionFurther diagnosticevaluation5%Management ofconcomitant emergentconditionsPatient refusalFigure 17. Top four reasons in 2019 for IV rt-PA initiation beyond 60 mins.The percentages above represent patients with a primary stroke diagnosis of ischemicstroke in whom IV tPA was initiated greater than 60 minutes after hospital arrival The mostcommon reason for delay in IV rt-PA beyond 60 minutes was that care-team was unable todetermine the eligibility of the patient, composing 38% of delays in 2019.28
Modified Rankin Scale at DischargeModified Rankin Scale at Discharge 2019(n 11292) 2019 (n 11292)16%13%11%11%11%9%4%0123456Figure 18. Modified Rankin Scale at Discharge 2019.75% of patients had their Modified Rankin Scale at discharge documented in 2019, anincrease from previous years (see figure 19). The Modified Rankin Scale ranges from 0-6,with the following designations for values: 0 - No symptoms at all 1 - No significant disability despite symptoms: Able to carry out all usual activities 2 - Slight disability 3 - Moderate disability: Requiring some help but able to walk without assistance 4 - Moderate to severe disability: Unable to walk without assistance and unable toattend to own bodily needs without assistance 5 - Severe disability: Bedridden, incontinent and requiring constant nursing care andattention 296 - Death
Modified Rankin Scale at Discharge Documented 2018-2019 2018 (n 10422) 2019 (n 11292)75%73%Documented mRS at dischargeFigure 19. Percentage of patients with Modified Rankin Scale documented from 2018-2019.30
Complication TypesComplications Among Stroke Patients 2018 201955%54%55%45%18%12%6%IV t-PA & SymptomaticIntracranial HemorrhageIntra-arterial &IV t-PA & Life-threatening,Symptomatic Intracranialserious systemic hemHemorrhage7%Intra-arterial & LifethreateningFigure 20. Complications found in IV rt-PA from 2018-2019.The most common type of complication for IV-tPA in 2019 was Intra-arterial andSymptomatic Intracranial Hemorrhage at 55%. This means that out of all patients with aprimary stroke diagnosis of ischemic stroke who received IV t-PA or intra-arterial thrombolytictherapy, most complications were an Intra-arterial and Symptomatic Intracranial Hemorrhage.There is no increase in this type of complication from 2018 to 2019.31
Initial Exam findingsInitial Exam Findings 2019 2019 (n 13963)54%36%39%21%3%Weakness/ParesisAltered Level ofConsciousnessAphasia/LanguageDisturbanceOther neurologicalsymptomsNo neurologicalsigns/symptomsFigure 21. Initial exam findings in 2019.The two most common findings in initial exam of patients in 2019 wereweakness/paresis (54%) and neurological symptoms other than altered level ofconsciousness and aphasia (39).32
Average Length of StayAverage Length of Stay 201911.98.45.85.44.03.62.4All barachnoid IntracerebralHemorrhage HemorrhageStroke ofUncertainTypeNo nlyFigure 22. Average length of stay in 2019.The type of stroke with the longest length of hospital stay (LOS) was SAH at about 12days, and the shortest LOS was TIA at about 2 and a half days.GTWTG/PAA Defect FreePercentage GWTG/PAADefect Free 2019(n 11836)NotDefectFree5%Defect Free95%Figure 23. Percent of patients who received defect-free care according to GWTG standards.33
CDC/COV Defect FreePercentage CDC/COV Defect Free 2019n 12586Not DefectFree18%Defect Free82%Figure 24. Percent of patients who received defect-free care according to Center for DiseaseControl (CDC) standards.34
LIMITATIONS TO DATA PRESENTED INTHIS REPORTData reported are based on the data provided to the Tennessee Stroke Registry fromreporting hospitals and may not be inclusive of all strokes in the state of Tennessee. Data arecombined for all hospitals and are reported in aggregate.35
HOW TO PARTICIPATE IN GWTG-STROKEAccording to Tennessee House Bill 123, all certified comprehensive and primarystroke centers in Tennessee are required to submit their data to the TSR in order toimprove stroke care in the state. The bill requires data to be provided from hospitals ona quarterly basis. Additional information is available on the TSR website, as well as theHospital Participation form and the Amendment to Hospital Participation Form:https://www.etsu.edu/cph/biostat epidemiology/tnstroke.php.The local GWTG contact is Kayley Pelton, who can assist hospitals in enrolling inGWTG-Stroke and the Tennessee Stroke Registry.Local GWTG Representative:Kaley Pelton, MPH, RT(R)Director, Quality & Systems
College of Public Health Randy Wykoff, MD, MPH & TM Dean of the College of Public Health Department of Biostatistics and Epidemiology Megan Quinn, DrPH, MSc. Tennessee Stroke Registry Manager Kelsi McKamey, BA Tennessee Stroke Registry Graduate Assistant American Heart Association/American Stroke Association Kaley Pelton, MPH, RT(R)