Transcription
Stroke Systems of Care: A Stroke Preventionand Treatment Strategy for DelawareGRAY MATTERSA Report of the Delaware Stroke Task ForceJanuary 2007The Delaware Stroke Task Force is a Sub-Committee of the Delaware HealthCare Commission‘s Chronic Illness & Disease Management Task Force
Delaware Stroke Task Force Members & ContributorsThe Honorable Bethany Hall-Long, State RepresentativeThe Honorable Patty Blevins, State SenatorThe Honorable Pam Maier, State RepresentativeThe Honorable Dorinda Connor, State SenatorThe Honorable Vance Funk, Mayor of NewarkPaula Roy, Executive Director, Delaware Health Care CommissionMichell Fulmer, Delaware Dietetic Association, Primordial & Prevention Sub-Committee ChairSteven Blessing, EMS Director, State of DelawareLee Dresser, MD, Acute & Sub-Acute Treatment Sub-Committee ChairJohn Scholz, University of Delaware, Rehabilitation Sub-Committee ChairAlisa Olshefsky, Division of Public Health, Continuous Quality Improvement Sub-Committee ChairMary Kate McLaughlin, Office of the GovernorRob Rosenbaum, MDJoseph Letnaunchyn, President, Delaware Healthcare AssociationSpiros Mantzavinos, Christiana Care Health SystemBeth Mineo Mollica, Delaware Assistive Technology InitiativePaul Silverman, Division of Public HealthDr. Anthony Munson, Neurology Associates, P.A.Joe Fitzgerald, New Castle County Chamber of CommerceGlen Luedtke, Sussex CountyJoel Rutenberg, MDDr. Herman Ellis, State of DelawareYrene Waldron, Executive Director, Delaware Healthcare Facilities AssociationSuzanne Raab Long, Delaware Healthcare AssociationMichael Duva, Delaware Healthcare AssociationWendy Gainor, Medical Society of DelawareBetsy Wheeler, President, Wheeler & Associates Management Service, Inc.Colin Faulkner, Director, Kent County Department of Public SafetySharon Anderson, Christiana Care Health SystemMoonyeen Klopfenstein, RN, Christiana Care Health SystemAngel Dewey, Bayhealth Medical CenterWilliam Rosenfeld, Bayhealth Medical CenterLynn Toth, Beebe Medical CenterSarah CarmodyDiane Hainsworth, Division of Public HealthGary FaderKathy Curtis, Christiana Care Health SystemShirley Moran, Christiana Care Health SystemPaula Savini, Quality Insights of DelawareEdward Sobel, DORuth HansenElyce TavaniPriscilla MurphyKristi Walters, Wheeler & Associates Management Service, Inc.Brenda Grassett, Delaware Technical & Community CollegeEvelyn Hayes, University of DelawareMaria Matos, Latin American Community CenterMichele Szymborski, NemoursDawn McHughRobin Roth2
Ellen BarkerMarlyn Marvel, Delaware Health Care CommissionSarah McCloskey, Delaware Health Care CommissionLinda G. Johnson, Delaware Health Care CommissionDavid Frazer, American Heart Association & American Stroke AssociationJanice Parker, American Heart Association & American Stroke AssociationPatty Cannon, American Heart Association & American Stroke Association3
CONTENTSEXECUTIVE SUMMARY Critical Findings Delaware Hospital Survey Results Recommendations Performance Measures610111215INTRODUCTION17MEDICAL & ECONOMIC CONSEQUENCES of STROKE Incidence and Death Rates Economic Costs Nature and Types of Stroke Consequences of Stroke Right Hemisphere Strokes Left Hemisphere Strokes Nonspecific Effects1718192121212222RISK FACTORS22TREATMENT AND REHABILITATION Treatment for Ischemic Stroke Treatment for Hemorrhagic Stroke Rehabilitation Clinical Flow Diagram for Stroke Rehabilitation24252527STROKE ORGANIZATIONS Professionalo National Stroke Project Public and Volunteero American Stroke Association (ASA)o National Stroke Association (NSA)o National Stroke Council (NSC) Government - Federal National Institute of Neurological Disorders and Stroke (NINDS) State of Delawareo Delaware Stroke Initiativeo Delaware Health Care Commissiono Delaware Division of Public Health (DHSS)28282828282929292930303030STROKE OFFICE MACRO PERSPECTIVE Administrative Approaches3131PREVENTION RECOMMENDATIONS Reducing Risk Factors, Morbidity and Mortality Access to Best Preventive Practices Research and Information313132324
ACUTE CARE RECOMMENDATIONS Acute Care Goal Stroke Response Plan Treatment Structure Promoting Improved Care3434343435REHABILITATION RECOMMENDATIONS Continuity of Care Access to Appropriate Care Evidence-Based Standards for Rehabilitation Plans Standards for Unaccredited Facilities3535363636FUNDING SOURCES Proposed STOP Act CDC Chronic Disease Prevention Health Programs Tobacco Settlement Act Additional Funding Sources3737373939GLOSSARY40APPENDICES Appendix 1: CDC Report Appendix 2: Sub-Committee Notes: Prevention & Primordial Care Appendix 3: Sub-Committee Notes: Notification & Response of EMS Appendix 4: Sub-Committee Notes: Acute & Sub-Acute Stroke Careo Delaware Hospital Survey Results Appendix 5: Sub-Committee Notes: Rehabilitation of Stroke Survivors Appendix 6: Sub-Committee Notes: Continuous Quality Improvement Appendix 7: Ohio Plan Appendix 8: Pennsylvania Proposal Appendix 9: National Healthcare Quality Report State Snapshot 2005 Appendix 10: Dr. Robert Rosenbaum Power Point Presentation Appendix 11: Paul Silverman Power Point Presentation Appendix 12: Steven Blessing Power Point Presentation Appendix 13: American Heart Association 2006 Stroke At-a-Glance4142464955566066687073* Appendices 10 – 13 are available electronically upon request. For more information, contactthe Health Care Commission at (302) 672-5187.5
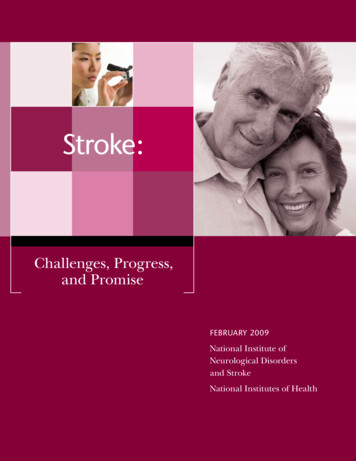
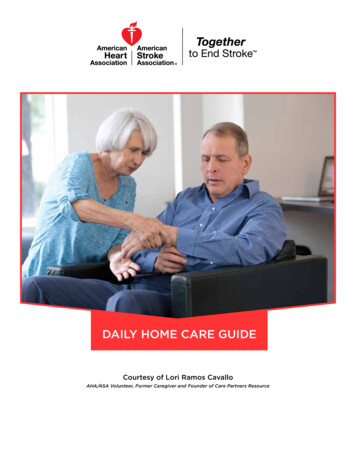
EXECUTIVE SUMMARYLeading Cause of DeathStroke is among the most serious public health challenges facing the State of Delaware andthe United States. Sometimes referred to as a brain attack, stroke is the third leading causeof death and a leading cause of adult disability. This devastating illness is a particularlysevere problem in Delaware. The U.S. Census Bureau reports Delaware’s population ofcitizens who are 65 years-old and older is greater than the national average, 13.1% inDelaware versus 12.4% in the United States, and the incident rate for Stroke increase withage, as illustrated in Table 1 below:Table 1. Delaware Health and Social Services, Division of Public HealthNumber and Rate of Delaware ResidentDischarges due to Cerebrovascular Disease:Delaware, 2004All agesAll Races 1515-4445-6465 es are crude and age-specific rates, per 10,000 population. In 2004, females of bothraces had higher hospitalization rates than males. Hospitalization rates for stroke are verysimilar across race and sex categories, but they differ a great deal between age groups, withthe 65 group having the highest rate of discharges. ALOS refers to the average length ofstay at the hospital in days.6
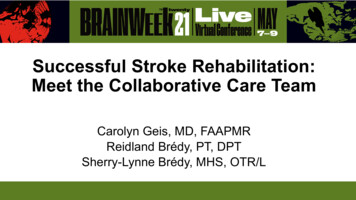
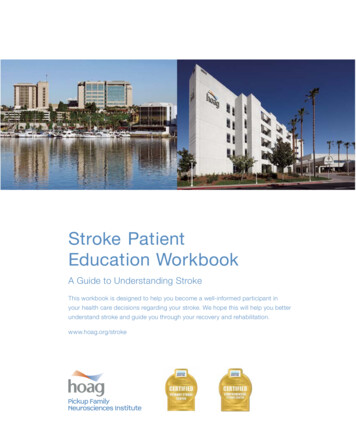
LEADING CAUSE OF DISABILITYStroke is the 3rd leading cause of death and a leading cause of disability. In addition to thesocial policy and public health implications, there is a significant negative economic impact tothe patient, their families and the entire spectrum of the health care delivery system.Table 2. Delaware Health and Social Services, Division of Public HealthPercent Distribution of StrokeHospitalizations by Length of StayDelaware, selected years, 1994-2004100%ALOS 7.8daysALOS 6.1daysALOS 5.8daysALOS 5.6days15 days90%8-14 days80%70%4-7 days60%50%40%3 days or less30%20%10%0%1994199720012004Discharge YearThe average length of stay (ALOS) decreased 29.1%, from 7.8 in 1994 to 5.6 in 2004. Thedecrease in ALOS was accompanied by a shift in the distribution of length of stay towardshorter hospital stays. In 2004, the average charge for a stroke hospitalization was 15,607.00.As the population of Delaware continues to age, the incidence of Stroke and the resultingnumber of death and disabilities are likely to increase.RESPONSE TO STROKEThe first maxim among professionals who face the challenge of stroke is this: The best wayto treat a stroke is to prevent it. A new Stroke Office, Vascular Disease Unit would greatlyassist in the implementation of preventive efforts that address the specific requirements ofunderserved urban and rural populations. In addition, they can ensure that preventive effortsare tailored to the cultural backgrounds and other characteristics of the public intended to beserved. Currently, 32 states and the District of Columbia receive CDC funding for State Heart7
Disease and Stroke Prevention Programs, 19 as capacity building programs and 14 as basicimplementation programs. Delaware does not currently receive CDC funding for this type ofprogram. A primary recommendation of this report is to have Delaware apply for the CDCfunding.In 1998, the U.S. Congress first provided funding for CDC to initiate a national, state-basedheart disease and stroke prevention program with funding for eight states that includedcapacity building criteria, such as:Develop and update a comprehensive state plan for heart disease and strokeprevention by developing heart-healthy policies, changing physical and socialenvironments and eliminating disparities (e.g., those based on geography, gender,race or ethnicity, or income)Increase awareness of the signs and symptoms of heart attack and strokePromote enhanced policies for treating stroke as an acute emergencyThe next essential component of a comprehensive stroke treatment and prevention system isan acute care structure that takes the maximum realistic advantage of the new therapies andresponds to the need to administer treatment within three hours of onset.Finally, the stroke program must address the needs of stroke survivors. Many survivorsneed extensive rehabilitation services, and the earlier the services are provided, the morelikely the patient can preserve function and maintain independence.CURRENT DELAWARE STROKE STRATEGIESDelaware is fortunate to have several excellent strategies in place to address the challenge ofstroke with considerable success. These diligent efforts occur in both the private and publicsectors by professionals and volunteers who deserve our gratitude and support. Some of theoutstanding success has been demonstrated through hospital and physician collaborations,Delaware Department of Health and Social Services, Delaware Health Care Commission,Delaware Emergency Management Services (EMS), Volunteer Fire and Ambulance entities,Delaware Stroke Initiative, American Heart Association and American Stroke Association, justto name a few.Of all the tremendous efforts to create statewide stroke initiatives, Delaware’s EMS hasexcelled in developing best practice standards that include, but are not limited to:All dispatchers must be certified Emergency Medical Dispatchers (EMDs).All 911 call centers are required to use the Priority Medical Dispatch System (PMDS)Paramedics in Delaware MUST attend state approved continuing education programs.Transport to the nearest appropriate CT-capable medical facility without delayHowever, more must be done to establish consistent, evidence-based standards across thespectrum of stroke education, treatment and rehabilitation for all the citizens and visitors toDelaware.In addition to its high incidence and devastating effects, two other factors have causedgreater attention to be paid to stroke. Recent advances in treatment, including the emergence8
of thrombolytic drug therapies (such as tPA), have made it possible to limit the damagecaused by some strokes. However, these therapies must be administered rapidly after theonset of symptoms to be effective, usually within the first critical three hours. Consequently,the stroke care community must develop a new approach to the structure of stroke treatmentand must educate the public about the need to treat stroke as an immediate medicalemergency.A second factor is proposed federal legislation called the Stroke Treatment and OngoingPrevention (STOP) Act that would provide block grant funding for stroke prevention andtreatment. The legislation contemplates a phased in appropriation rising from 50 to 125million, contingent in later years on matching state appropriations. If this legislation isenacted, Delaware will need to have a stroke prevention, treatment and rehabilitationstructure in place to qualify for federal funding. However, even if the federal STOP STROKEACT does not provide funding, the need to address Stroke Care System in Delaware mustnot be forgotten.HISTORYDelaware Health Care Commission assembled the Delaware Stroke Task Force at therequest of four distinguished members of Delaware’s General Assembly: RepresentativeBethany Hall-Long, Representative Pam Maier, Senator Patricia Blevins, and SenatorDorinda Connor.Their request, dated December 5, 2005, was addressed to the Delaware Health CareCommission, and stated the following, “Given the impact of stroke in Delaware, we believe itwould be appropriate to develop a stroke system of care in Delaware through the ChronicIllness and Disease Management Task Force (Task Force) or Health Care Commission.Other states have created – through legislation – Stroke Task Forces to develop statewidestroke systems of care. We believe it is not necessary to pursue a legislatively created stroketask force to develop statewide stroke systems but rather work through this existing TaskForce and/or Health Care Commission. The Task Force’s charge and recommendationsmake the Task Force an appropriate body to develop a statewide stroke system.”In response, the Delaware Health Care Commission and the Chronic Illness and DiseaseManagement Task Force created the Delaware Stroke Task Force to explore the currentenvironment, identify potential areas of excellence as well as gaps in stroke care systems,and make recommendations to develop and improve Delaware’s statewide stroke systems.The Stroke Task Force included experts in various related fields from all three counties todraw upon their knowledge and experience working together to improve Delaware’s responseto stroke. They divided into five sub-committees, focused on specific aspects of the strokecare systems: Primordial & Primary Prevention; Emergency Medical Services; Acute & SubAcute Stroke Care; Rehabilitation; and Continuous Quality Improvements. Theirrecommendations are set forth in this report and their critical findings are briefly summarizedbelow.The report includes a summary of data relating to stroke incidence and death rates, data onrisk factors affecting stroke, a description of current stroke care systems in Delaware and avision for improving the outcomes for stroke victims.9
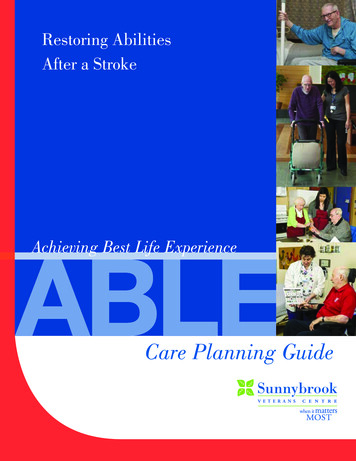
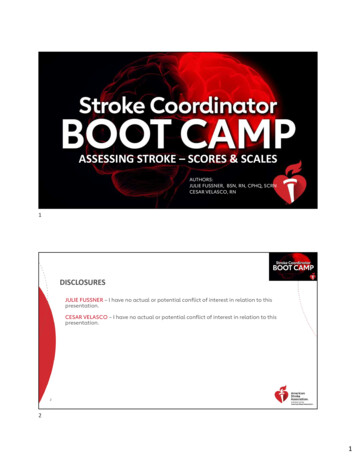
Critical Findings:2.5% of Delaware adults say they have been told they had a stroke.Estimated 15,560 living Delaware adults who report having had a stroke.There were differences in the death rates due to stroke and trends among the threecounties (New Castle, Kent, and Sussex).Mortality rates due to stroke were relatively higher in Kent than in New Castle andSussex during the period 1989 to 2000.Mortality rates continued to decline in the Kent and Sussex counties, while in the NewCastle county there was a decline during the period from 1989 until 1997, increasedslightly after that and assumed a plateau until 2003.Among Delaware adults who report having had a stroke, 25% said they were currentsmokers. Another 32.8% reported being former smokers.42% of stroke victims in the survey said they had never smoked compared with 50% ofpeople who did not have a stroke.The smoking link may be more dramatic than it seems: because smoking-relateddeaths from heart disease tend to occur at younger ages than strokes, many smokersmay have died earlier from other diseases – e.g. heart attacks, emphysema, or lungcancer.Among Delaware adults who are obese, about twice as many reported having astroke.Among Delaware adults who have diabetes, the relationship is even more dramatic.Only 2.5% of adults without diabetes reported having a stroke. However, 10.1% ofdiabetics reported having a stroke (and 9.3% of pre-diabetics)During 2005, paramedics in Delaware treated and transported,ooooo6453 patients with head injury592 patients with non-hypoglycemic altered mental status1206 patients with seizures, 176 (15%) were treated for epileptic status.1160 patients with stroke1233 patients with syncope (temporary loss of consciousness)Sub-Committee NotesComplete sub-committee notes are included as appendices to this report. Also included areextensive reports and data on each stage of stroke treatment, compiled from various sources,including but not limited to Emergency Medical Services Office, Division of Public Health,Chronic Disease Bureau, Delaware Health Care Association, Delaware Health CareCommission, American Stroke Association, a division of American Heart Association and theDelaware Stroke Coalition.Delaware Hospital Survey Results:One of the recommendations from the sub-committee on Acute and Sub-Acute Care is toconduct a comprehensive analysis of Delaware’s stroke system capacity. A preliminarysurvey was administered in October 2006 to all of the hospitals in Delaware to assess basicstroke treatment capabilities for the purpose of this report. The results have been providedby the Delaware Healthcare Association and may be found on Page 11.10
Is aneurosurgeonavailable atyourhospital?Neurologiston-call24-hours aday to treatpatients?Does hospitalhave writtenguidelines forevaluationandtreatment ofstroke?Estimatednumber ofstrokepatientsseen in2005Wilming.NONONONOYESYESYESNOVery rare difficult toestimateDoverNONOYESNOYESNOYESNO152NOYESNO61- over 6monthperiodBayhealth Kent GeneralHospitalYESNOCurrentlydeveloping- Have achampion &membersestablished and arewriting protocolsYESYESYESNOYESIn process ofestablishingnew SYESYESYES200BeebeMedicalCenterLewesNONOCCHS 2 –ChristianaHospitalStantonNOIn-house CTtech until 1am,then on-call techwith a 30 minuteavailabilityYESCCHS WilmingtonHospitalWilming. Wilming.MilfordAI DuPontChildren’sHospitalBayhealth MilfordHospitalSt. tients peryearYES –SeafordNanticokeMemorialHospital10-15 newNONOYESYESWilming.VeteransAffairsHospital2Is computedtomography(CT Scan) ofthe headavailable 24hours a day?CityDelawareHospitalName 11Does hospitalhave a StrokeTeam?Is TPAavailablefortreatment?Is there awrittenprotocol fortreatment ofstroke withTPA?Doeshospitalhave aStrokeUnit?YESYESYESYESSurvey results provided by Delaware Healthcare Association (November 2006)CCHS Christiana Care Health SystemAlsodeveloped anexpeditedprotocol for itsuse in stroke &potential TPAYESYES - for TPAcandidatesYES27010011
RECOMMENDATIONS FOR DELAWARE STROKE SYSTEM OF CARERECOMMENDATIONS AT-A-GLANCE:Stroke Office and Stroke CoordinatorData Sharing & Stroke RegistryPreventionPublic Awareness & Education CampaignResearch & Continuing EducationStatewide StandardsOptimal Patient Care: from onset of symptoms to rehabilitationFundingPerformance MeasuresPRIORITY RECOMMENDATIONS:(For full sub-committee reports, see appendices beginning on Page 38.)Stroke Office Creation of a Stroke Office within a Vascular Disease administrative unit under theBureau of Chronic Disease, Division of Public Health that would be responsible forvascular diseases, including cardiovascular disease and stroke, which could performthe functions recommended in this report. Potential funding sources include StateMaster Tobacco Settlement funds, grants from the Centers for Disease Control &Prevention (CDC), and funding made available pending the passage of the federalStop Stroke Act. Because of the particular urgency of stroke as a public health problem in Delaware, aStroke Office should be established with the specific purpose to coordinate statewideefforts for stroke prevention, treatment, and rehabilitation programs, disseminate bestpractices and other information, and conduct research. The Office should be led by aStroke Coordinator and guided by a representative multidisciplinary advisorycommittee. Adequate resources should be committed to enable the Office to leadDelaware's response to stroke.Data Sharing & Stroke Registry Assess the collection, analysis and use of existing data and enhance data sharingopportunities to facilitate medical research related to stroke prevention/treatment andto develop best practices. The Stroke Coordinator would act as a catalyst to moveDelaware toward the long-term goal of developing a Stroke Registry to track all phasesof stroke care as well as long-term patient outcome data by exploring current andfuture data sharing systems, including but not limited to the Delaware HealthInformation Network (DHIN) statewide clinical information sharing utility.12
Prevention (Activities to be functions of the new Stroke Office)1. Make available to health professionals the best practices for preventive care andestablish a clearinghouse for stroke research and information. Explore methods toincrease stroke screenings and public education about stroke through partnering withorganizations such as the Delaware Stroke Initiative.2. Promote screening and education about blood pressure, cholesterol, blood sugar, andrisk factors (smoking, diabetes, etc.) to all primary care and non-traditional primarycare providers, such as OB-GYN, nurse practitioners, community health clinics, etc.3. Study strategies for expanding the availability of insurance coverage for diagnosticservices and preventive care for stroke, as well as education of insurance companiesregarding the cost effectiveness of providing coverage for preventive treatments, suchas nutritional counseling and increased physical activity.Public Awareness & Education Campaign Establish educational programs to raise awareness of the signs and symptoms ofstroke. Emphasize the recognition of risk factors (hypertension, smoking, highcholesterol, diabetes, and drug use) to help increase early preventive interventions.o Use a variety of media outlets in English and Spanish, targeting diverseaudiences (urban/rural, gender, age, race/ethnicity, etc.)o Include stroke resource guides, smoking cessation materials, and obesityprevention/healthy eating techniqueso Inform potential victims, their caregivers, first responders and acute/sub-acutemedical professionals to: Recognize signs/symptoms of stroke; Treat stroke and TIA (mini-stroke) as medical emergencies; Obtain immediate medical assistance using 9-1-1, recognizing that a3-hour window of opportunity exists for critical treatment.Notification & Response of Emergency Medical Services1. Implement a data exchange system between the Delaware Office of EmergencyMedical Services (OEMS- within the Division of Public Health) and hospital emergencydepartments to track outcomes for stroke survivors. Close the data gap.2. Continue the use of a uniform pre-hospital screening/rapid detection tool byemergency first responders. Routinely evaluate available tools to determine theoptimal means of conducting pre-hospital screening with methods that representcurrent research and positive patient outcomes.3. Enhance education and certification of emergency medical dispatchers & emergencymedical services personnel. Develop alternative delivery methods to accommodatethe volunteers’ schedules such as on-line or off-site trainings, i.e. videos, DVDs, etc.13
Acute Care & Sub-Acute Care1. Conduct a comprehensive, in-depth study of Delaware’s stroke system capacity,including emergency departments, acute and sub-acute care providers, specialists,etc. Assess the capability of existing health care facilities (treatment options,equipment, space, staffing, etc.). Based on the assessment, share findings withemergency medical services, neurologists and hospitals to formulate a statewide planto allow optimal triage and treatment of stroke survivors.2. Explore transfer options to respond to strokes that are beyond a facility’s capability totreat. Evaluate options for emergency evaluation, triage and transfer of patientsamong in-state facilities as well as out-of-state transfers for patients requiringspecialized care available only at tertiary medical centers.3. Establish a long-term goal of improving acute care capacity such that no Delawareresident lives more than one hour away from a health care facility with capability ofproviding high quality treatment for acute strokes.4. Establish quality initiatives and continue to promote best practice models to expeditediagnosis and care, utilizing evidence-based guidelines developed by nationalorganizations and in cooperation with the Medical Society of Delaware. Continue toresearch acute therapy options, post treatment interventions, and the feasibility of newtreatment modalities as they become available.Rehabilitation1. Determine and document which pathway of care provides the greatest likelihood ofimproved function in individuals post-stroke. It is critical that stroke survivors’ functionalprogress be accurately tracked as they move through the health care system and todifferent treatment settings so that the most optimal pathway for particular levels ofinitial impairment and function can be identified. This initiative relies on the use ofinformation collected by a cardiac and stroke event registry using industry standards totrack survivors’ recovery and progress. Also, consider collecting data from the ActivityMeasure for Post-acute Care (AMPAC), based on International Classification ofFunction (ICF) standards, for survivors at each point along a given treatment pathway.2. Promote awareness and utilization of evidence-based rehabilitation guidelines bymaking continuing education opportunities and professional journals on strokerehabilitation more accessible to rehabilitation therapists.3. Increase the supply of occupational and speech therapy professionals in more remoteregions of the state where patients often have to wait up to a month or more beforeobtaining access to these disciplines because of the shortage of these healthprofessionals in the state.4. Research and explore opportunities with major insurance carriers operating within theState of Delaware regarding the possibility of allocating some of their end-of-yearreserve for stroke care as a carve-out diagnosis and encourage them to help collectdata on the AMPAC on patients insured by them. In addition, perform acomprehensive study of insurance coverage for rehabilitation to inform carriers of thetypes of coverage and benefits that can reduce over-utilization of nursing homes.14
5. Communicate with Delaware’s Congressional Delegation and State leaders regardingpotential impact of the Centers for Medicare & Medicaid Services recent call for ademonstration project that will develop and assess the effectiveness of post-acutecare assessment instruments, to ensure that Delaware is well positioned to participatein the pilot demonstration.FUNDINGImplementing these recommendations will require a substantial commitment of financialresources. In the present constrained fiscal environment, a variety of funding sources mustbe tapped to support a major initiative such as that outlined in this report, including creation ofpublic-private partnerships. In addition to the proposed federal STOP Stroke Act, anotherpotential source of funding may be through special appropriated funds possibly madeavailable through an increase in tobacco excise tax and/or a dedicated lottery. The StrokeOffice would be responsible for seeking funding opportunities through appropriatefoundations and medical charities. An immediate goal is to prepare Delaware’s applicationfor CDC funding, as described on page 9 of this report.The Stroke Task Force believes that directing funds and efforts toward enhancing strokeprevention and care will produce a return on investment by helping more Delawareansachieve longer, healthier lives, free of the tragic effects of stroke that darken the lives of ourcitizens and families. In addition, Delaware’s health care economic burden will be decreasedin direct correlation with a decrease in stroke incidence.PERFORMANCE MEASURESA stroke system should strive to optimize the overall effectiveness of the system and each ofits individual components. This goal should be accomplished by identifying performancemeasures for each component and for the system function as a whole (both process andoutcome measures) and by employing Continuous Quality Improvement (CQI) strategies incollaboration with key stakeholders. Both process and outcome measures will be developedto measure implementation of services, linkages among key stroke system components,obstacles to care, potential gaps, and most importantly - patient outcomes. (Measures arelisted on the following page.)15
-6Performance MeasuresStroke Plan ComponentPrimordial and primarypreventionMeasure TypeProcessMeasure Description Primordial and primarypreventionProcess Reach of distribution of new strokeprevention strategiesNumber of providers aware of emergingstroke prevention strategiesNumber of providers implementing in asystematic way the emerging strategies(pre/post intervention)Reach of community education activities,especially among at-risk populationsPercent change in knowledge andattitudes about the causes, signs andsymptoms of stroke among samplepopulationPrimordial and primarypreventionOutcome Number of deaths averted due to earlysign/symptom awarenessNotification of EmergencyMedical ServicesProcess Development of data exchange systembetween EMS and hospitals (yes/no)Data quality as measured by inter or intrarater reliability assessmentTime to CT capable emergency room Notification of EmergencyMedical ServicesOutcome Increase # of stroke victims who present inER Dept. w/in 3 hours of symptom onsetAcute and sub-acute stroketreatm
the stroke care community must develop a new approach to the structure of stroke treatment and must educate the public about the need to treat stroke as an immediate medical emergency. A second factor is proposed federal legislation