Transcription
TENNESSEE PERINATAL CARE SYSTEMGUIDELINES FOR REGIONALIZATION,HOSPITAL CARE LEVELS,STAFFING AND FACILITIES(Ninth Edition)Effective October 14, 2020Tennessee Department of HealthDivision of Family Health and WellnessBill LeeGovernorLisa Piercey, MD, MBA, FAAPCommissioner
TENNESSEE PERINATAL CARE SYSTEMGUIDELINES FOR REGIONALIZATION,HOSPITAL CARE LEVELS,STAFFING AND FACILITIES(Ninth Edition)Prepared by theWorkgroup on Regionalization Guidelines Revision and thePerinatal Advisory CommitteeWeb h-program-areas/mch/mch-prp.html(Under Program Areas/Maternal and Child Health/Perinatal Regionalization)
PERINATAL REGIONALIZATION IN TENNESSEEBackground/HistoryEfforts to implement a regionalized approach to perinatal care in Tennessee date back to the1970’s, at which time many national studies, including the landmark National March of Dimesdocument entitled “Toward Improving the Outcome of Pregnancy”, revealed that a coordinatedsystem of health care, outreach, and professional education could improve perinatal outcomesand lower infant mortality.In 1974, a “Neonatal Law” was passed (T.C.A. § 68-1-801-804) to establish the High-RiskNewborn Program at the four existing NICUs in Memphis, Nashville, Chattanooga and Knoxville.In 1977, the law appropriated state funds as well as expanded the program to include high-riskobstetrics and thereby created the Tennessee Perinatal Care System, establishing a PerinatalCenter within each of the four (4) designated regions. A fifth Center was established in JohnsonCity in 1986.Perinatal RegionsEach perinatal region is comprised of a group of contiguous counties. The perinatal regions andcounties are listed on page 6 of this document. Each region contains one Perinatal Center, whichhas been so designated by the Commissioner of the Tennessee Department of Health and iscapable of providing Level III or Level IV obstetric and neonatal care. The Regional PerinatalCenters are:West Tennessee Regional Perinatal CenterRegional Medical Center at Regional One HealthMemphis, TennesseeMiddle Tennessee Regional Perinatal CenterVanderbilt University Medical Center/Monroe Carrell, Jr. Children’s Hospital at VanderbiltNashville, TennesseeSoutheast Tennessee Regional Perinatal CenterErlanger Health System/T.C. Thompson Children’s Hospital at ErlangerChattanooga, TennesseeEast Tennessee Regional Perinatal CenterThe University of Tennessee Medical Center at KnoxvilleKnoxville, TennesseeNortheast Tennessee Regional Perinatal CenterJohnson City Medical Center/Niswonger Children’s HospitalJohnson City, TennesseePurpose and Responsibilities of Tennessee’s Regionalization SystemThe Perinatal Care System is a statewide infrastructure for the diagnosis and treatment of highrisk pregnant women, fetuses and neonates if no other appropriate facility is available to managetheir significant condition(s), regardless of financial status. All activities are in compliance with
medical and operation standards and the guidelines as set out in the Tennessee Perinatal CenterCare Systems Guidelines for Regionalization, Hospital Care Levels, Staffing and Facilities, latestedition; Tennessee Perinatal Care System Guidelines for Transportation, latest edition;Tennessee Perinatal Care System Educational Objectives for Nurses Levels I, II, III, IV, NeonatalTransport Nurses, latest edition; Tennessee Perinatal Care System Educational Objective inMedicine for Perinatal Social Workers, latest edition; and Tennessee Perinatal Care SystemGuidelines on Equipment, Supplies and Training for Emergency Medical Services and EmergencyDepartment Staff, latest edition.While the five (5) Regional Perinatal Centers operate within a designated hospital or university,the program is a standalone entity which provides: 24-hour consultation and referral for facilities and for health care providers within therespective perinatal regionProfessional education for providers (nurses, midwives, nurse practitioners, physicians,respiratory therapists, social workers, paramedics, etc.) within the regionMaternal and neonatal transportSite visits, upon request, to provide consultation regarding physical facilities, staffing, andpolicies and procedures at hospitals within the regionPost-discharge maternal follow-up and post-discharge neonatal follow-upMeasuring and monitoring maternal and newborn outcomes for the regionMaintain ongoing relationships with regional providers, prenatal facilities and hospitalsIndirectly, the system impacts all mothers and babies in Tennessee by assuring that health careproviders are educated on high risk perinatal care and have a system of consultation available tothem. In FY 2020 (July 1, 2019 – June 30, 2020), Tennessee’s Regional Perinatal Centersprovided direct care for 5,077 high-risk neonates and 18,820 high-risk maternal patients.All obstetric and neonatal-related activities within the Regional Perinatal Center should occurunder the direction of a board-certified maternal fetal medicine specialist and a board-certifiedneonatologist, respectively. There should also, at a minimum, be one (1) obstetric and one (1)neonatal outreach educator/coordinator on-staff. It is also advisable to have an individual on staffto monitor expenditures and track contract services and deliverables. Staff of the Centers do notprovide direct care; and therefore, should not be considered a part of a specific department withinthe direct services arm of the hospital/facility. The Regional Perinatal Center Co-directors areresponsible for the staff hired to carry out the scope of services of the contract and for followingall of the guidelines established for the Tennessee Perinatal Care System.Perinatal Advisory CommitteeThe Perinatal Advisory Committee was established by statute (T.C.A. §68-1-803-804) and existsas a consultative body to advise the Department of Health in administration and implementationof the regionalization system across Tennessee. The Committee is comprised of twenty-one (21)members as designated in statute, including the obstetric and neonatal directors of the fiveRegional Perinatal Centers, private sector providers, hospital administrators, medical schoolrepresentation, nurses working in perinatal medicine, and consumer and public healthrepresentatives. The committee is required to meet at least once annually. Committee membersas well as invited experts are also instrumental in ensuring that the program’s detailed Guidelinesand other perinatal documents/guidelines/educational objectives remain current and are updated
every five years, a practice that has occurred since the first set of Guidelines was published in1978.FundingThe Division of TennCare oversees all contractual arrangements for this program, and theTennessee Department of Health, Division of Family Health and Wellness, is responsible for theprovision of technical assistance, the coordination of programmatic activities, and convening thePerinatal Advisory Committee. Each designated hospital/university accepts funds on behalf of theRegional Perinatal Center. The Centers are supported by funds from TennCare, Tennessee’sMedicaid Plan with the Centers for Medicare & Medicaid Services, and state appropriations.Specific state appropriations were made available in 2016 to expand outreach education, andeach Center was provided additional funds strictly for this purpose as outlined by the contract.ResourcesThe Perinatal Regionalization Program has a variety of resources available, including copies ofthe latest editions of the Guidelines, a Perinatal Regionalization Fact Sheet, and a highlight videowhich may be accessed by visiting the website: mch-prp.html/.
PERINATAL ADVISORY COMMITTEEMATERNAL LEVELS WORK GROUP1David Adair, MD, Chattanooga, ObstetricsTimothy Canavan, MD, Johnson City, ObstetricsCatherine (Kitty) Cashion, RN-BC, MSN, Memphis, ObstetricsJane Anna Cummings, RN, BSN, Savannah, ObstetricsRhonda Crossett, RNC-OB, MSN, Paris, ObstetricsW. Michael DeVoe, MD, Johnson City, NeonatalRamasubbareddy Dhanireddy, MD, Memphis, NeonatalSusan Drummond, RN, MSN, Nashville, ObstetricsLusia Filetti, MD, Covington, ObstetricsMelissa Gammons, BSN, RN, MBA, Jackson, ObstetricsConnie Graves, MD, Nashville, ObstetricsPatti Jacobs, RNC, BSN, Johnson City, ObstetricsTraci Josephsen, RN, MSN, Chattanooga, ObstetricsGwinnett Ladson, MD, NashvilleCheryl Major, RNC, BSN, Nashville, NeonatalRebecca Martens, RN, MSN, NP-C, Chattanooga, ObstetricsDennis McWenney, MD, Nashville, ObstetricsKimberly Strickland, BSN, RNC-OB, Covington, ObstetricsGilbert Thayer, MD, Savannah, ObstetricsCraig Towers, MD, Knoxville, ObstetricsSelman Welt, MD, Johnson City, ObstetricsZachary Young-Lutz, RN, BSN, Knoxville, Obstetrics1A work group was convened in August 2020 to make updates to the obstetrics sections consistent with thosepublished in the ACOG/SMFM Levels of Maternal Care Consensus, August 2019. Members who assisted with thisproject were added to the existing work group list from the 8th edition since no significant changes were made tothe neonatal sections.
PERINATAL ADVISORY COMMITTEE(As of October 2020)MembersMorgan McDonald, MD, ChairTimothy Canavan, MD, Johnson CityMary Catherine (Kitty) Cashion, RN-BC, MSN, MemphisEtoi Garrison, MD, NashvilleMark Gaylord, MD, KnoxvilleSusan Hall Guttentag, MD, NashvilleShawn Hollinger, MD, Johnson CityJoseph Kipikasa, MD, ChattanoogaPaul Korth, CookevilleMary Lee Lemley, RN, MSN, NashvilleGiancarlo Mari, MD, MemphisAmber Price, DNP, CNM, NashvilleMarilyn Robinson, MD, MemphisAnuj Sinha, DO, ChattanoogaGrant Studebaker, MD, JacksonAjay Talati, MD, MemphisLenita Thibault, MD, KingsportCraig Towers, MD, KnoxvilleKevin Visconti, MD Johnson CityLeah Williamson, Cordova
TABLE OF CONTENTSPreface . 1Introduction . 2Regional Perinatal Centers . 4Summary of Perinatal Service Levels . 9Birth Center Facilities . 13Level I Facilities . 19Level II Facilities - Obstetrics . 29Level II Facilities - Neonatal . 37Level III Facilities - Obstetrics . 44Level III Facilities - Neonatal . 52Level IV Facilities - Obstetrics . 59Level IV Facilities - Neonatal. 67
TENNESSEE PERINATAL CARE SYSTEMGUIDELINES FOR REGIONALIZATION, HOSPITAL CARE LEVELS,STAFFING AND FACILITIESPREFACEThe first edition of these Guidelines appeared in 1978; further editions were published in 1984,1990, 1997, 2004, 2010, 2014 and 2017. This ninth edition was prepared by a work grouprepresenting a broad spectrum of health care professionals drawn from throughout the state. Itwas subsequently adopted by the Perinatal Advisory Committee. As was the case with the eightpreceding editions, the ultimate goal of these Guidelines is to improve perinatal outcomes inTennessee by providing quality care to every mother and newborn. The Guidelines describecomponents of various care levels with the full realization that many of these components arealready in place while others are goals which are actively pursued. The document emphasizesthe importance of communication and collaboration among all health care professionals whoprovide perinatal services in Tennessee. It is also important to remember that, because our state’spopulation has grown to include people from all over the world, the services provided to mothersand newborns must be culturally, as well as medically, appropriate.As described in Tennessee Code Annotated 68-1-802,(a) The department [of Health] is directed to develop a plan to establish a program for thediagnosis and treatment of certain life-threatening conditions present in the perinatal period.(b) The program shall assist pregnant women and their fetuses and newborn infants bydeveloping a regionalized system of care, including highly specialized personnel, equipmentand techniques that will decrease the existing high mortality rate and the life-long disabilitiesthat currently prevail in surviving newborn infants.Regionalization of perinatal health care in the State of Tennessee was motivated by anoverwhelming need to ease access to contemporary care by as large a segment of the populationas was feasible. Since publication of the first edition, the number of providers of perinatal healthcare has increased remarkably. There has also been an increase in the level of expertise in mostinstitutions in the state. However, many Tennessee counties have hospitals without perinatalservices. We must continue to provide professional advice and supervision on perinatal healthcare to health care providers, thereby making quality care available to every woman and child inTennessee regardless of community size and geographic location.In order to assure contemporary pertinence of these and subsequent Guidelines, the PerinatalAdvisory Committee has limited its approval to a period no longer than five years from the date ofapproval by the Commissioner of the Department of Health. A revision of this document will bemandatory at that time, unless one becomes necessary at an earlier date.1
INTRODUCTIONProfessional advice and supervision of health care must be available to every pregnant womanand her newborn child in Tennessee. The vast majority of the newly born are healthy, but intactsurvival is jeopardized in a substantial number who require complex medical attention. Thesesevere illnesses often can be anticipated and then ameliorated or eliminated by specialmanagement of high-risk mothers. In the extreme, this type of medical attention entailsrecruitment of a variety of specialized professional personnel who are generally moreconcentrated in densely populated communities. It is in these larger communities that the fullestspectrum of medical consultants, nurse specialists, laboratory capabilities and equipment areusually situated, but complex medical management must be accessible to all patients regardlessof community size and geographic location. That perinatal mortality and morbidity can besubstantially reduced by contemporary technology has been plainly documented for decades.From this fact alone, there remains a sense of urgency to make such technology available to allmothers and infants in Tennessee, to eliminate existing inaccessibility to complex care, and toassure a high quality of medical attention in every hospital that renders it, complexity of care andlocation of hospital notwithstanding.The overall goal is effective care for the State as a whole. Available resources must beappropriately utilized. Access to care (Levels I, II, III, and IV) should be available within allperinatal regions, and each level of care, no matter how complex, should be of optimal quality.The sole determinant of where care will be administered, and by what types of personnel,should be the severity of illness and not be limited to or governed by financial constraints. Thedecision regarding the location of care should be made jointly by the obstetric and pediatriccare providers caring for the mother and fetus / newborn, as level of maternal care and levelsof neonatal care may not match within facilities.When providing care and considering selection of a delivery site for the maternal fetal dyad,the perinatal provider(s) should evaluate both components separately. The delivery locationselected should provide the highest level of care for the component with the highest acuityneed. This decision must be made independent of gestational age, fetal weight, and maternalcondition. For example, a woman with acute fatty liver of pregnancy at term requires Level IVmaternal care because of this life-threatening condition. Conversely, a woman whoexperiences preterm premature rupture of membranes at 24 weeks of gestation but has nomaternal issues should be transferred to a facility capable of providing appropriate neonatalcare for this situation.Although services should be available as close to home as possible, transfer of patients from onehospital to another is inevitable if all levels of care are to be provided. An effective system requiresdesignation of hospitals for provision of care according to their capacity. These Guidelines havebeen written for that specific purpose. Beyond care levels, consultation and transport of patientsshould provide functional continuity between hospitals. Fundamental to all these activities is thecontinuing education of personnel within perinatal regions; without it the effectiveness of care willdeteriorate.Although these Guidelines are addressed to institutions that provide perinatal services, the basicemphasis is on the role of physicians, nurses and other health care personnel who directly andpersonally provide patient care. Institutions herein described differ from each other in the varietyof services performed by their personnel. The institutional components of the Tennessee Perinatal2
Care System include birth centers and four hospital categories that indicate their capacities toprovide complex care for mothers and newborns: Levels I, II, III, and IV. Each level of care reflectsrequired capabilities, physical facilities, and medical and support personnel. Each higher level ofcare includes and builds on the capabilities of the lower levels.In regard to obstetric care, Levels I, II, III, and IV are adopted from the ACOG / SMFM consensusstatement on levels of maternal care, initially published in 2014 and subsequently updated inAugust 2019. Trauma is not integrated into the levels of maternal care because trauma centerlevels are already established. Pregnant women should receive the same level of trauma care asnon-pregnant patients. In terms of neonatal care, we have adopted the hospital designations(Levels I, II, III, and IV) recommended by the American Academy of Pediatrics Committee onFetus and Newborn in its policy statement on Levels of Neonatal Care, which was published in2012. Adoption of these designations brings Tennessee into compliance with national guidelines.Regional Perinatal Centers operate within Level III or Level IV institutions that have beendesignated by the State to coordinate certain regional activities that relate to professionaleducation, patient transport and inter-hospital functions, as well as care of patients. The generalcharacteristics of each care level are summarized in the paragraphs that follow. Details of thesecharacteristics are set forth in the corresponding service level sections of these Guidelines.The 2019 ACOG/SMFM consensus statement on levels of maternal care provided clarificationrelated to the availability of personnel by providing more specific terminology as detailed below:†Readily available: the specified person should be available 24 hours a day, 7 days a week,for consultation and assistance, and able to be physically present on-site within a time framethat incorporates maternal and fetal or neonatal risks and benefits with the provision of care.Further defining this time frame should be individualized by facilities and regions, with inputfrom their obstetric care providers. If referring to the availability of a service, the service shouldbe available 24 hours a day, 7 days a week unless otherwise specified.**Physically present: the specified person should be on-site in the location where perinatalcare is provided 24 hours a day, 7 days a week.3
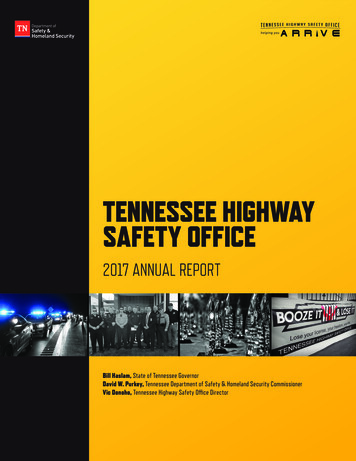
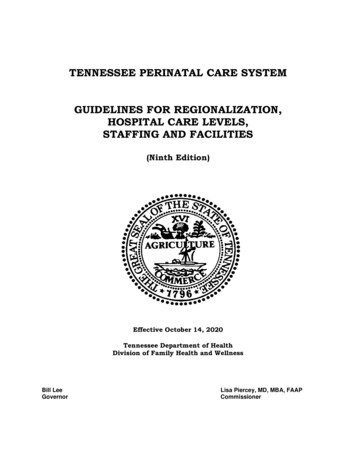
REGIONAL PERINATAL CENTERSI.REGIONS DEFINEDThere are five perinatal regions in Tennessee: Northeast, East, Southeast, Middle, andWest. Each region is comprised of a group of contiguous counties. The perinatal regionsand the counties comprising them are listed on page 6. Each region contains one RegionalPerinatal Center, which has been so designated by the Commissioner of the TennesseeDepartment of Health.II.REGIONAL PERINATAL CENTERS LISTEDEach of Tennessee's five Regional Perinatal Centers is capable of providing Level III orLevel IV obstetric and neonatal care. The Regional Perinatal Centers are:Northeast Tennessee Regional Perinatal CenterJohnson City Medical Center HospitalJohnson City, TennesseePerinatal Center Office: (423) 431-6640Obstetric Education/Training Requests: Patti Jacobs, RN-C, BSNPhone: (423) 431-5352 E-mail: patti.jacobs@balladhealth.orgNeonatal Education/Training Requests: Vicki Davis, RN, BSNPhone: (423) 431-5646 E-mail: vicki.davis@balladhealth.orgL&D: (423) 431-6436Referrals: 1-800-365-5262Neonatal Consult/Transport: (423) 952-3720General Hospital Operator: (423) 431-6111East Tennessee Regional Perinatal CenterThe University of Tennessee Medical Center at KnoxvilleKnoxville, TennesseeObstetric Education/Training Requests: Lauren Lake, APRN, FNP-CPhone: (865) 305-9300 E-mail: llake@utmck.eduNeonatal Education/Training Requests: Nicole Watson, RN, BSN, CLCPhone: (865) 305-9300 E-mail: nwatson@utmck.eduL&D: (865) 305-9830Maternal Referrals: 1-800-422-9301 or 865-305-9300Neonatal Consult/Transport: 1-800-732-7295 or (865) 305-9834NICU: (865) 305-9834General Hospital Operator: (865) 305-90004
Southeast Tennessee Regional Perinatal CenterErlanger Health System/Children’s Hospital at ErlangerChattanooga, TennesseeObstetric Education/Training Requests: Jennifer Shelton, RNC-OB, MSNPhone: (423) 778-3547 E-mail: jennifer.shelton@erlanger.orgNeonatal Education/Training Requests: Jill Rimmer, RNC, NICPhone: (423) 778-5096 E-mail: elizabeth.rimmer@erlanger.orgL&D: (423) 778-7956OB Consults / Referrals: (423) 778-8100 or 1-866-4HI-RISKNeonatal Consult/Transport: (423) 778-6438NICU: (423) 778-6438General Hospital Operator (Erlanger): (423) 778-7000General Hospital Operator (Children’s Hospital): (423) 778-6011Middle Tennessee Regional Perinatal CenterVanderbilt University Medical Center/Monroe Carell, Jr. Children’s Hospital at VanderbiltNashville, TennesseeObstetric Education/Training Requests: Susan Drummond, RN, MSN, C-EFMPhone: (615) 343-9930 E-mail: susan.drummond@vumc.orgNeonatal Education/Training Requests: Mary Lee Lemley RNC, MSNPhone: (615) 343-8686 Email: mary.lemley@vumc.orgL&D: (615) 322-2555OB Consults/Referrals: 1-888-636-8863 (1-888-MFM-VUMC)Neonatal Consult / Transport: 1-855-322-9111NICU: (615) 322-0963General Hospital Operator (Vanderbilt): (615) 322-5000General Hospital Operator (Children’s Hospital): (615) 936-1000West Tennessee Regional Perinatal CenterRegional Medical Center at Regional One HealthMemphis, TennesseeObstetric Education/Training Requests: Kitty Cashion, RN-BC, MSNPhone: (901) 448-4794 Email: mcashion@uthsc.eduNeonatal Education/Training Requests: Nancy Ruch, RN, MSN, NNPPhone: (901) 448-6717) Email: nruch@uthsc.eduL&D: (901) 545-7345OB Inpatient Transport: (901) 545-8181Neonatal Consult/Transport: (901) 545-7366NICU: (901) 545-7366General Hospital Operator: (901) 545-71005
PERINATAL REGIONSNORTHEAST TENNESSEE(Johnson City)MIDDLE TENNESSEE(Nashville)WEST RutherfordSmithStewartSumnerTrousdaleVan onObionShelbyTiptonWeakleyEAST UTHEAST McMinnMarionMeigsPolkRheaSequatchie6
III.SERVICES PROVIDEDTennessee's Regional Perinatal Centers must provide the following services:A.B.C.Consultation and Referral1.If no other appropriate facility is available to manage significant high-riskconditions, the Regional Perinatal Center must accept all such patientsregardless of financial status.2.Telephone consultation by obstetric and newborn sub-specialists must beavailable to physicians and nurses within the region 24 hours a day, 7 daysa week.Professional Education1.For the Staff of the Regional Perinatal Center: A program of professionaleducation must be maintained for the staff of the Regional Perinatal Center.These programs should satisfy the educational requirements forphysicians, nurses, social workers, and others who function in theadministration of Level III or Level IV care.2.For the Staff of Other Hospitals in the Region: The Regional PerinatalCenter must maintain a program of professional outreach education forhospitals within its region. These programs of instruction require a staff ofqualified educators to present ongoing courses to Level I, II, and IIIhospitals. These courses must satisfy the educational objectives set forthin the series of publications for the education of nurses and social workerspublished by the Tennessee Department of Health.Maternal-Fetal and Neonatal TransportThe Regional Perinatal Center is responsible for maternal-fetal and neonataltransport described for Level III or Level IV facilities elsewhere in these Guidelines.Whereas the provision of these transport services is an option for Level III or LevelIV units that do not function as Regional Perinatal Centers, transport services arerequired of a Regional Perinatal Center. Transport for the purpose of admission tothe Regional Center must be made available to all patients within the stateregardless of their financial status, and to patients referred from other RegionalPerinatal Centers. Protocols for transport should conform to the most recent editionof the Tennessee Perinatal Care System Guidelines for Transportation, publishedby the Tennessee Department of Health.D.Site VisitsThe Regional Perinatal Center staff will engage in site visits upon request withinits region.7
E.Post-discharge Maternal Follow-upFollow-up evaluation of selected women who are discharged from the RegionalPerinatal Center should be arranged.F.Post-discharge Neonatal Follow-upFollow-up evaluation of selected infants who are discharged from the RegionalPerinatal Center should be performed. Neonatal intensive care unit graduates whoare considered high risk and those with birthweights 1500 grams should beenrolled in an organized follow-up program that tracks and records medical andneurodevelopmental outcomes to allow later analysis.G.Data CollectionThe Regional Perinatal Center must compile data (Program Objectives Report[POR]) on educational outreach that is performed as well as the region’s analysisand evaluation of maternal and neonatal outcomes for quality improvementaccording to requirements prescribed by the Tennessee Perinatal Care System.These data are forwarded to a central facility on a regular basis. All RegionalPerinatal Centers, if possible, should support clinical teams within the institutionthat are responsible for implementing State or National continuous qualityimprovement initiatives by providing advisory assistance, sharing data from thePOR, disseminating information to the region, and/or aiding with financial support.H.Perinatal Advisory CommitteeThe Perinatal Advisory Committee was established by statute and exists as aconsultative body to advise the Department in administration and implementationof the perinatal regionalization system across Tennessee. The Committee iscomposed of individuals with expertise and a vested interested in the health andwellbeing of pregnant women and newborns, including the State’s Title V / MCHBlock Grant Director, Co-directors of each of the five perinatal centers, as well asrepresentation from local hospitals, medical specialists in obstetrics and newbornconditions/private practice, family physicians, obstetrical and neonatal intensivecare nurses, a medical school, and the general public.(TCA § 68-1-803-804)8
SUMMARY OF PERINATAL SERVICE LEVELSREGIONAL PERINATAL CENTERSThe perinatal regionalization program was established to provide for the diagnosis and treatmentof certain life-threatening conditions of pregnant women and newborn infants. The five regionalperinatal centers across the state have made this specialized care available by providing astatewide mechanism to health care providers for consultation and referral of high risk patients;transport of these patients, if necessary; personnel skilled in high risk perinatal care; postgraduate education for physicians, nurses, and other medical personnel; and site visits to localhospitals. These Centers, which are co-directed by the high risk perinatal sub-specialists, offeroutreach education for facilities and health care provide
In 1977, the law appropriated state funds as well as expanded the program to include high-risk obstetrics and thereby created the Tennessee Perinatal Care System, establishing a Perinatal Center within each of the four (4) designated regions. A fifth Center was established in Johnson City in 1986.