Transcription
Emergency Care Quality Imaging Benchmarksin a Statewide Collaborative:Estimated Excess and Associated SpendingKocher KE, Arora R, Bassin BS, Benjamin LS, Bolton M, Dennis BJ, HamJJ, Krupp SS, Levasseur KA, Macy ML, O’Neil BJ, Pribble JM, SherwinRL, Sroufe NS, Uren BJ, Nypaver MMDirector, Michigan Emergency Department Improvement CollaborativeDepartment of Emergency MedicineUniversity of MichiganSAEM 5.15.19www.medicqi.orgkkocher@umich.edu@kekocher
The TeamMEDIC CoordinatingCenter Keith Kocher, MD MPHMichele Nypaver, MDMichelle Macy, MD MSJason Ham, MB BChApril Proudlock, RNEmily White, MSMegan Hogikyan, MPHAlyson Stone, BAChristie Radden, MAMEDIC Partner Institutions Beaumont – Farmington HillsBeaumont Hospital – Royal OakBeaumont Hospital – TroyChildren’s Hospital of Michigan, DMCDetroit Receiving Hospital, DMCHelen DeVos Children’s HospitalHenry Ford Allegiance HospitalHenry Ford HospitalHolland HospitalHurley Medical CenterHuron Valley Hospital, DMCLakeland HealthMidMichigan Medical CenterMunson Medical CenterSt. Joseph Mercy Hospital - Ann ArborSt. Joseph Mercy Hospital - LivingstonSinai-Grace Hospital, DMCSparrow HospitalUniversity of MichiganMEDIC SiteAbstractorsMEDIC Clinical Champions Timothy Archer, MDRajan Arora, MDBen Bassin, MDLee Benjamin, MDMolly Bolton, MDDominic Borgialli, DO MPHBlaine Dennis, MDLori Dixon, MDBrian Holt, DODiane Kaiser-Alexander, DOSeth Krupp, MDKelly Levasseur, DORobert Nolan, MDBrian O’Neill, MDJames Paxton, MD MBAZach Sawaya, MDRob Sherwin, MDAthina Sikavitsas, DOMichelle Slezak, MDDave Somand, MDNicole Sroufe, MD MPHSanford Vieder, DOIan Walker, DO Terri BetheaHeather FaraoneNancy FauserPenny HawkinsWendy HerzogPaulette HoeraufAmy MawhorterLaura McLaughlinAngela MedranoSarah MiceliAndrea MillardKaren MooreMegan PerkajNancy RadovicIrene RasmussenMary SeraphinoffVita VyskocilKristin WatsonNancy WuCassandra York@kekocher
Disclosures Michigan Emergency Department Improvement Collaborative(MEDIC) Funded by Blue Cross Blue Shield of Michigan and Blue Care Network www.medicqi.org Agency for Healthcare Research and Quality (AHRQ) Career development award@kekocher
Background and ObjectivesGap betweenevidence andpracticePerformancevariesSingle etwork ofEDs1. Describe the building of a large scale quality collaborative to drive practice change.2. Report real world baseline performance across key ED quality measures.3. Estimate excess imaging and associated spending.@kekocher
BackgroundPracticeChangeEst. 2015LearningCollaborative@kekocher
Collaborative SitesFor Current Study15 hospitals community & academic rural & urban pediatric & adult25,000 – 125,000 ED visitsannually at each site 23% pediatric ( 18 yearsold) 22% of all ED visits inMichigan
Methods: Structurehttp://www.valuepartnerships.com/ Michigan Cardiovascular Consortium Michigan Society of Thoracic and CardiovascularSurgeons Quality Collaborative Michigan Bariatric Surgery Consortium Michigan Surgical Quality Collaborative Michigan Anticoagulation Quality ImprovementInitiative Michigan Oncology Quality Consortium Hospital Medicine Safety Consortium Michigan Trauma Quality Improvement Project Michigan Urological Surgery Improvement Collaborative Michigan Radiation Oncology Quality Consortium Michigan Arthroplasty Registry Collaborative for QualityImprovement Michigan Spine Surgery Improvement Collaborative Michigan Value Collaborative Anesthesiology Performance Improvement andReporting Exchange Michigan Pharmacists Transforming Care and QualityConsortium Michigan Emergency Department ImprovementCollaborative Integrated Michigan Patient-Centered Alliance on CareTransitions
Methods: Quality Measurement4. Adult suspectedpulmonaryembolism2. Pediatric minorhead injury3. Pediatricrespiratory illnessCanadian HeadRulePECARN RuleChest CTsCTappropriatenessCT overuse &utilizationAsthma,bronchiolitis,croupCXR utilizationdiagnostic yield1. Adult minorhead injury@kekocher
Methods: Data SourcesAutomatedElectronic DataoooooooooEvery ED visitPatient demographicsChief complaintsVital signsTriage scoreTimestampsProcedure codesDiagnostic codesDispositionProviderOn Demand Real TimeReports via Web PlatformManual ChartAbstractionSpecific to core quality initiativeso Minor head injuries (symptoms,findings)o CT scans for suspected PEo Pediatric respiratory illnessesCoordinating CenterCustomized Reports@kekocher
Methods: Analysis StepsStep 1 Analyzed MEDIC registry data from 6/1/16 – 10/31/17 Prior to when quality improvement efforts began Report site level baseline performance and variationStep 2 Calculate the Achievable Benchmark of Care (ABCTM)* for each qualitymeasure Objective, reproducible, data-driven method for determining qualityimprovement targets across a population of performance* NW Weissman, JJ Allison, CI Kiefe, et al. Achievable benchmarks of care:the ABCs of benchmarking. J Eval Clin Pract 1999;5: 269-281.
Methods: Analysis StepsStep 3 Calculate reduction in imaging studies for each quality measure basedon meeting ABCTM targetStep 4 Calculate associated spending related to avoided imaging studiesprojection Price estimates from the Healthcare Bluebook website*Step 5 Use direct standardization to extrapolate these findings to a typical EDwith 20% children Express as avoidable imaging and excess spending for every 10,000annual ED visit volume* Healthcare Bluebook, Accessed 10/25/18. Available at: https://www.healthcarebluebook.com/
Results: MEDIC Baseline Performance*Collaborative(%)Site Median, %(Range)ABCTMBenchmark (%)40.947.7 (24.3 – 58.6)55.5CT Overuse10.39.9 (5.8 – 16.8)5.8Intermediate Risk CT Utilization23.422.7 (9.5 – 54.4)12.538.144.0 (9.0 – 62.1)18.58.78.4 (7.5 – 14.3)10.7Quality InitiativeAdult Head Injury (Canadian Rule)CT AppropriatenessPediatric Head Injury (PECARN Rule)Pediatric Respiratory IllnessesCXR UtilizationAdult Pulmonary EmbolismCT Diagnostic Yield* Data from 6/1/16 – 10/31/17
Results: MEDIC Projected Excess and Savings Over 1Year if ABCTM Benchmark Achieved*Quality InitiativeAdult Head Injury (Canadian Rule)CT AppropriatenessPediatric Head Injury (PECARN Rule)CT OveruseIntermediate risk CT utilizationPediatric Respiratory IllnessesCXR utilizationAdult Pulmonary EmbolismCT Diagnostic YieldCount of 2017Imaging Studies inthe MEDIC RegistryNumber of PotentiallyAvoidable Studies in2017Range of PotentiallyAvoidable Spendingin 20172,4221,083 325,983 – 747,270TOTALS:94 head CTs1,5196833,308 CXRs4,254 PE chest CTsTOTALS:44 3.59 –392 5.02million 13,244 – 30,360 117,992 – 270,4805,8903,308 135,628 – 231,56017,8844,254 2,994,816 –3,743,520* Calculated based on Healthcare Bluebook range of “fair prices” for Michigan as follows: CPT code 70450 (non-contrast headCT) 301-690; CPT code 71275 (CT chest angiography) 704-880; CPT code 71020 (2-view CXR) 41-70
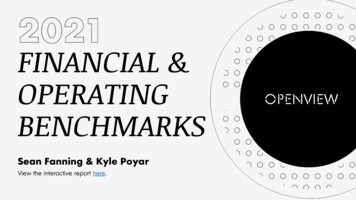
Results: Projected Excess Imaging Per IndividualED Over 1 YearNumber of Imaging StudiesPotentially Avoidable450421400350PE CT300245211250CXR200Head CT1221501001364250 240681410K20K30K40K50K60K70K80K90K100KED Annual Visit Volumes (in 10,000 visit increments)@kekocher
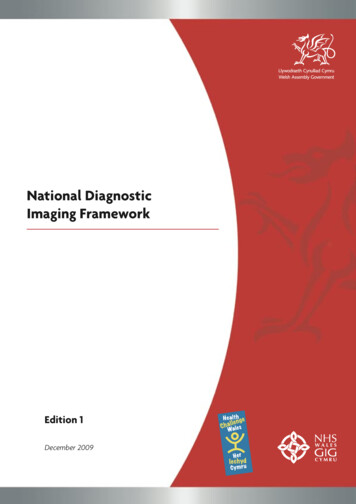
Results: Projected Savings Per Individual EDOver 1 Year* 481,887Projected Avoidable Spending 500,000 400,000Total 300,000 240,943PE CT 347,597 200,000 100,000Head CT 173,798 48,189CXR 34,760 010K20K30K40K50K60K70K80K90K100KED Annual Visit Volumes (in 10,000 visit increments)* Calculated based on Healthcare Bluebook range of “fair prices” for Michigan as follows: CPT code 70450 (non-contrast headCT) 301-690; CPT code 71275 (CT chest angiography) 704-880; CPT code 71020 (2-view CXR) 41-70
Limitations: Assumptions and Implications1. MEDIC data sources are valid and high quality Analysis relies on diagnostic/procedural codes and human abstractors2. 15 EDs in Michigan are representative National and individual ED case mix and practice patterns may vary3. Avoidable imaging projections are theoretical Providers may respond to quality improvement intervention differently4. Excess spending projections are theoretical Prices vary, savings vary@kekocher
Conclusion15 Michigan EDsUrbanRuralCommunityAcademicChildrenAdult1.12 Million ED Visits( 22% of all ED visits in Michigan )4 Quality MeasuresBaseline PerformanceChildren:(1) Computed Tomography (CT) in Minor HeadInjuries(2) Chest X-Ray (CXR) in Respiratory ConditionsPotentially Avoidable Low ValueCare in 2017:Adults:(3) CT in Minor Head Injuries(4) CT in Suspected Pulmonary Embolism1,519 Head Injury CTs3,308 CXRs4,254 PE CTs 3.59 – 5.02 million1. Substantial opportunity for avoiding low value imaging studies in EDs.2. If ABCTM targets can be safely achieved, result would be significant health care savings.* Manuscript accepted, soon to be in presswww.medicqi.org@kekocher
Beaumont -Farmington Hills Beaumont Hospital -Royal Oak Beaumont Hospital -Troy Children's Hospital of Michigan, DMC . Michigan Bariatric Surgery Consortium Michigan Surgical Quality Collaborative Michigan Anticoagulation Quality Improvement Initiative