Transcription
Supplementary AppendixThis appendix has been provided by the authors to give readers additional information about their work.Supplement to: Sands BE, Peyrin-Biroulet L, Loftus EV Jr, et al. Vedolizumab versus adalimumab for moderateto-severe ulcerative colitis. N Engl J Med 2019;381:1215-26. DOI: 10.1056/NEJMoa1905725(PDF updated on November 27, 2019.)
Online SupplementTable of ContentsList of Study Investigators and Sites (VARSITY Study Group)List of Highest Recruiting SitesVARSITY Steering CommitteeData Safety Monitoring BoardProgressive Multifocal Leukoencephalopathy (PML) Adjudication CommitteeConcomitant Corticosteroid Discontinuation/TaperingPML MonitoringMonitoring and Auditing of Study Procedures and Data QualityPatient Eligibility CriteriaPrespecified Additional Outcomes in ProtocolPrespecified Exploratory Outcomes in Statistical Analysis PlanStatistical AnalysisFigure S1Patient Disposition.Figure S2Clinical Remission at Week 52 in Subgroups by Patient Demographic andBaseline Characteristics.Figure S3Clinical Remission and Endoscopic Improvement at Week 52 by BaselineConcomitant Medication Use.Figure S4Clinical Remission at Week 14 in the Overall population and Subgroups by PriorTNF Inhibitor Therapy.Figure S5Endoscopic Improvement at Week 52 by Patient Demographic and BaselineCharacteristics.2
Figure S6Corticosteroid-free Clinical Remission at Week 52 by Patient Demographic andBaseline Characteristics.Figure S7Oral Corticosteroid Use.Figure S8Histological Remission at Week 52 in Subgroups by Prior TNF inhibitor Therapy.Figure S9Histological Remission at Week 14.Figure S10Minimal Histologic Disease Activity at Week 52.Figure S11Clinical Response based on Total Score on the Mayo Scale at Week 14 in theOverall Population and Subgroups by Prior TNF Inhibitor Therapy.Table S1Schedule of Trial Procedures.Table S2Baseline Disease Characteristics.Table S3Post Hoc Analysis of Clinical Remission and Endoscopic Improvement at Week52, Using the Weighted Cochran–Mantel–Haenszel Method.Table S4Sensitivity Analysis to Assess the Impact of Dropouts Under Different MissingData Mechanisms for Primary and Secondary Outcomes.Table S5Results from Prespecified Analyses of Efficacy Outcomes.Table S6Most Frequent Adverse Events.Table S7Serious Adverse Events.3
List of Trial Investigators and Sites *ArgentinaDr Sebastian Calvo; Dr Edgardo Gimenez; Dr Jorge Hector Resk†; DrEmiliano Pablo TronAustraliaDr Mohammed Al-Ansari†; Dr Jane Andrews; Dr Peter Bampton†; DrHenry Debinski†; Dr Peter Hendy; Dr Gerald Holtmann†; Dr RupertLeong; Dr Gregory Moore†BelgiumDr Pieter HindryckxBosnia andDr Tatjana BaracHerzegovinaBulgariaDr Raina Draganova; Dr Iskren Kotzev; Dr Ivanka Marinova†; Dr MarioMarkov†; Dr Yordan Mihaylov†; Dr Dimitar Pavlov; Dr MarianaPenkova†; Dr Asen Petrov; Dr Zoia Spassova; Dr Daniela Stoyanova; DrEmilian Velev†; Dr Borislav Vladimirov; Dr Feliks Yanev†CanadaDr Jeffrey Axler; Dr Richard Fedorak‡; Dr Sharyle Fowler; Dr SmitaHalder†; Dr Vipul Jairath†; Dr Terry Ponich; Dr Karen WongColombiaDr Edwin Baez†; Dr Juan Ricardo Marquez VelasquezCroatiaDr Marko Banic; Dr Ivan Bogadi†; Dr Vladimir Borzan; Dr JadrankaCetina Zgrablic; Dr Marko Duvnjak; Dr Maja Gusej†; Dr Zeljko KrznaricCzech RepublicDr Ivana Cechova†; Dr Tomas Hala; Dr Lubos Janu; Dr Pavel Kohout;Dr Milan Lukas; Dr Martina Machkova; Dr Jan Matous; Dr JanUlbrych†; Dr Tomas VanasekDenmarkDr Lone Klinge; Dr Terje Rannem†; Dr Klaus TheedeEstoniaDr Julia Borissova†; Dr Karin Kull†FranceDr Morgane Amil; Dr Yoram Bouhnik†; Dr Cyrielle Gilletta; DrMathurin Fumery; Dr Jean-Charles Grimaud; Dr Xavier Hebuterne; DrDavid Laharie†; Dr Jacques Moreau; Dr Laurent Peyrin-Biroulet; DrXavier Roblin†GermanyDr Daniel Baumgart†; Dr Carsten Buening; Dr Johanna Dinter†; DrAnnika Gauss†; Dr Tanja Kuehbacher; Dr Khan Fareed Rahman†; Dr4
Ingolf Schiefke; Dr Stefan Schreiber; Dr Ulrike Von Arnim†; Dr StefanZeuzem†Hong KongDr Wai Keung Leung; Dr Michael Kin Kong LiHungaryDr Istvan Altorjay; Dr Laszlo Bene†‡; Dr Peter Lakatos†; Dr TamasMolnar; Dr Agnes Salamon; Dr Robert Schnabel; Dr Zsolt TulassayIsraelDr Yona Avni; Dr Olga Barkay; Dr Sigal Fishman; Dr Eran Goldin; DrDan Keret†; Dr Adi Lahat-Zok; Dr Ehud Melzer; Dr Timna Naftali; DrAssy Nimer; Dr Baruch Ovadia; Dr Eran ZittanItalyDr Angelo Andriulli; Dr Maria Cappello†; Dr Fabiana Castiglione†; DrSilvio Danese; Dr Walter Fries†; Dr Paolo Gionchetti; Dr Anna Kohn; DrGiovanni Maconi; Dr Marchi Santino; Dr Edoardo Savarino; DrAntonino Privitera†; Dr Marco Romano†; Dr Maurizio Vecchi†; Dr EricaVillaKorea,Dr Jae Hee Cheon†; Dr Dong Soo Han†; Dr Byung-ik Jang; Yoon-TaeRepublic ofJeen†; Dr Joo Sung Kim; Dr Sung Kook Kim; Dr Hyo-Jong Kim; DrYoungHo Kim; Dr Kang-Moon Lee; Dr Bo In Lee; Dr Dong il Park; DrYoung Soo Park; Dr Geun Am Song; Dr Byong-Duk YeLatviaDr Juris Pokrotnieks; Dr Ivars TolmanisLithuaniaDr Goda Denapiene; Dr Arunas Kancauskas; Dr Violeta Jakovlevaite; DrLaimas JonaitisMexicoDr Aracely Cruz Palacios; Dr Emmanuel Larriva de los Reyes; Dr LeslyeAsela Lujano Nicolas; Dr Eduardo Mendoza FuerteNetherlandsDr Geert D’Haens; Marieke Pierik†; Janneke van der Woude†PolandDr Krystian Adrych; Dr Wit Cezary Danilkiewicz; Dr Beata GawdisWojnarska; Dr Marek Hartleb; Dr Marek Karczewski; Dr JaroslawKierkus; Dr Ewa Malecka-Panas; Dr Robert Petryka; Dr WojciechPiotrowski; Dr Jaroslaw Regula; Dr Jacek Romatowski; Dr JerzyRozciecha; Dr Grazyna Rydzewska; Dr Patryk Smolinski; Dr PiotrWalczak; Dr Michal Walczak; Dr Barbara Wozniak-Stolarska5
PortugalDr Jose Cotter; Dr Luis Lopes; Dr Francisco Portela; Dr João RodriguesCarvalhoRomaniaDr Liliana Simona Gheorghe; Dr Adrian-Eugen Goldis; Dr Radu-BogdanMateescuRussianDr Rustem Abdulkhakov; Dr Alina Agafyina; Dr Olga Alexeeva; DrFederationBagdadi Alikhanov†; Dr Elena Bunkova; Dr Mikhail Dvorkin; Dr IrinaGubonina; Dr Vladimir Kashnikov; Dr Maria Livzan; Dr MarinaOsipenko; Dr Asfold Parfenov†; Dr Anatoly Pershko; Dr MarinaPesegova; Dr Vladimir Rafalskiy†; Dr Olga Reshetko; Dr VladimirSimanenkov; Dr Svetlana Tsybulko; Dr Ekaterina Valuyskikh; DrAlexey YakovlevSerbiaDr Mirjana Cvetkovic; Dr Dragomir Damjanov; Dr Srdjan Djuranovic;Dr Predrag Dugalic; Dr Aleksandar Nagorni; Dr Petar Svorcan; DrNatasa Zdravkovic PetrovicSlovakiaDr Ivan Bunganic; Dr Milos Gregus; Dr Tibor Hlavaty; Dr FrantisekHorvathSpainDr Eugeni Domenech Morral†; Dr Rodrigo Jover Martinez†; Dr MariaIsabel Vera MendozaTaiwanDr Ming-Jium Shieh; Dr Cheng-Chung WeiTurkeyDr Engin Altintas; Dr Ozlen Atug; Dr Can Gonen; Dr Hulya Hamzaoglu;Dr Saadettin Hulagu; Dr Murat TorunerUkraineDr Ivan Chopey; Dr Svitlana Danyliuk; Dr Oleksii Datsenko; Dr NataliiaGolovchenko; Dr Oleksandr Golovchenko†; Dr Ihor Hospodarskyy; DrValeriy Ivanov; Dr Volodymyr Klymenko; Dr Olena Levchenko; DrViktor Lizogub†; Dr Yuriy Mostovoy; Dr Oleksandr Oliinyk; Dr IgorPolianskyi†; Dr Volodymyr Pyrohovskyi; Dr Sergii Shevchuk; DrGrygorii Ursol; Dr Valeriy Vdovychenko; Dr Vira VyshyvanyukUnited KingdomDr Ian Beales†; Dr Matthew Brookes†; Dr Chukwaka Nwokolo; Dr JackWinterUnited StatesDr Avanish Aggarwal†, Dr Humberto Aguilar†; Dr Zaid Alnoah†; DrEsperanza Arce-Nunez†; Dr Calin Arimie; Dr James Arterburn†; Dr6
Curtis Baum; Dr Emanuelle Bellaguarda†; Dr Bonnie Bock†; Dr TashaBoone; Dr Norman Callahan†; Dr Jonathon Chapman†; Dr Stuart Chen†;Dr Michael Chiorean; Dr Allan Coates; Dr Michael Connor†; Dr StevenDellon; Dr Gerald Dryden; Dr George Du Vall; Dr Lucky Flores; DrRonald Fogel; Dr Juan Frias†; Dr Philip Ginsburg†; Dr EugeneGreenberg; Dr David Grunkemeier†; Dr Paul Hellstern; Dr HansHerfarth; Dr Brenda Hoffman; Dr Sara Horst†; Dr Samuel Idarraga; DrHeba Iskandar†; Dr Rajesh Jain†; Dr Erin Jenkins†; Dr Barry Kaufman†;Dr Abdul Khaleq†; Dr Ahtaram Khan†; Dr Sunil Khurana; Dr JasonLake; Dr James Leavitt†; Dr Bernard Leman; Dr Derek Lewis†; DrDaniel Lindenberg†; Dr Edward V Loftus Jr†; Dr Louis Korman; DrJennifer Martin†; Dr Matthew McCullough; Dr Alfred McNair†; DrNilesh Mehta†; Dr Ece Mutlu†; Dr Vijay Narayen†; Dr Jorge PaoliBruno; Dr Nolan Perez†; Dr Raymond Phillips†; Dr Isaac Raijman; DrRuben Ramirez-Vega†; Dr Charles Randall; Dr Scott Rinesmith; DrTimothy Ritter; Dr Alan Safdi†; Dr Marc Saltzman†; Dr Bruce Sands†;Dr Jennifer Seminerio; Dr Michael Schulman†; Dr Shahriar Sedghi†; DrIra Shafran†; Dr Murali Shankar†; Dr David Silvers; Dr Nehad Soloman†;Dr Harvey Tatum†; Dr Robert Tepper†; Dr Felix Tiongco; Dr MartinValdes; Dr John Weber†; Dr Chen Zhang†*Only investigators consenting to be acknowledged are listed.†Investigators who screened but did not enroll randomized patients in the trial.‡Investigators who are deceased.7
List of Highest Recruiting SitesSites with 3% total enrollmentCity/State orInvestigator nameDr Jeffrey AxlerDr Jaroslaw KierkusDr Beata ySC (N 386), nIV (N 385), nPoland714Note: Only sites with greater than 3% of total enrollment in any treatment group are included.8
VARSITY Steering CommitteeBruce E. Sands, MD (Chair), Stefan Schreiber, MD, Laurent Peyrin-Biroulet, MD, PhD, EdwardV. Loftus Jr., MD.9
Data Safety Monitoring BoardKeith Lindor, MD (Chair), Henry Bodenheimer Jr., MD.10
Progressive Multifocal Leukoencephalopathy (PML) Adjudication CommitteeDavid B. Clifford, MD (Chair), Eugene O. Major, PhD, Michael H. Lev, MD, Joseph R. Berger,MD.11
Concomitant Corticosteroid Discontinuation/TaperingPatients who were receiving oral corticosteroids and had a clinical response at Week 6 asassessed by the Investigator began a non-fixed corticosteroid tapering regimen. Patients who didnot achieve clinical response at Week 6 initiated tapering on a subsequent study visit as soon as aclinical response was achieved. For patients who could not tolerate the corticosteroid taperwithout recurrence of clinical symptoms, corticosteroids could be increased up to the baselinecorticosteroid dose one time before tapering was restarted. In such cases, the tapering regimenabove was reinitiated within 2 weeks. Patients who consistently could not be tapered werewithdrawn from the trial.12
PML MonitoringAll patients were closely monitored for signs and symptoms of PML prior to administration ofeach dose of trial drug using a PML subjective symptom checklist, which assessed for any recentchanges in vision, speech, gait, sensation, comprehension, coordination, and personality. Anypositive response on the PML checklist prompted further objective evaluation based on aprespecified diagnostic algorithm (the PML Case Evaluation Algorithm). Cases of newneurological symptoms were promptly evaluated by an independent adjudication committee(IAC) of academic experts (including a neurologist, a neuroradiologist, and a virologist) using aprespecified diagnostic algorithm that included stepwise contrast-enhanced brain magneticresonance imaging and, if indicated, lumbar puncture with polymerase chain reaction analysis ofcerebrospinal fluid for JC virus DNA. If patients entered the algorithm, study drug was withhelduntil PML could be definitively excluded.13
Monitoring and Auditing of Study Procedures and Data QualityAt regular intervals, routine on-site monitoring visits were performed by clinical researchassociates (CRAs) at all sites on the basis of a prespecified written monitoring plan, and 100% ofdata were source verified during these visits. In addition, remote CRA and medical monitoring ofthe study’s electronic database, which included all source documents (case report forms andlaboratory results), was performed for each patient throughout the study according to themonitoring plan. In addition to monitoring visits, clinical quality assurance audits wereconducted by CRAs.An independent data safety monitoring board (DSMB) provided oversight of the phase 3vedolizumab program and met at 6-month intervals. The DSMB was composed of 2gastroenterologists and a statistician. Before scheduled meetings, the DSMB received unblindedtables and listings of all clinical safety data. The DSMB reviewed these data in closed sessionsand subsequently provided a recommendation to the sponsor. In addition, the DSMB receivedmonthly listings of all SAEs that included the most current individual reports of the Council forInternational Organizations of Medical Sciences (CIOMS) form.14
Patient Eligibility CriteriaInclusion Criteria1. In the opinion of the investigator, the patient is capable of understanding and complying withprotocol requirements.2. The patient or, when applicable, the patient’s legally acceptable representative signs and datesa written, informed consent form and any required privacy authorization prior to the initiation ofany study procedures.3. The patient has a diagnosis of UC established at least 3 months prior to Screening by clinicaland endoscopic evidence and corroborated by a histopathology report.4. The patient is male or female and aged 18 to 85 years, inclusive.5. The patient has moderately to severely active UC as determined by a total score on the Mayoscale of 6 to 12 with an endoscopic subscore 2 within 14 days prior to the randomization.6. The patient has evidence of UC proximal to the rectum ( 15 cm of involved colon).7. The patient with extensive colitis (up to the hepatic flexure) or pancolitis of 8 years durationor left-sided colitis of 12 years duration must have documented evidence that a surveillancecolonoscopy was performed within 12 months of the initial screening visit (may be performedduring the Screening Period).8. The patient with a family history of colorectal cancer, personal history of increased colorectalcancer risk, age 50 years, or other known risk factor must be up-to-date on colorectal cancersurveillance (may be performed during Screening).15
9. The patient:a) Has had previous treatment with TNF inhibitor without documented clinical responseto treatment (e.g., due to lack of response [primary non-responders], loss of response, orintolerance [secondary non-responders]), orb) Has previously used a TNF inhibitor (except adalimumab), and discontinued its usedue to reasons other than safety, orc) Is naïve to TNF inhibitor but is failing current treatment (e.g., corticosteroids, 5-ASA,or immunomodulators).10. A male patient who is non-sterilized and sexually active with a female partner ofchildbearing potential agrees to use adequate contraception from signing of informed consentthroughout the duration of the study and for 5 months after the last dose.11. A female patient of childbearing potential who is sexually active with a non-sterilized malepartner agrees to use routinely adequate contraception from signing of informed consentthroughout the duration of the study and for 5 months after the last dose.Exclusion CriteriaGastrointestinal Exclusion Criteria1. The patient has clinical evidence of abdominal abscess or toxic megacolon at the ScreeningVisit.2. The patient has had an extensive colonic resection, subtotal or total colectomy.16
3. The patient has had ileostomy, colostomy, or known fixed symptomatic stenosis of theintestine.4. The patient has a diagnosis of Crohn’s colitis or indeterminate colitis, ischemic colitis,radiation colitis, diverticular disease associated with colitis, or microscopic colitis.5. The patient has received any of the following for the treatment of underlying disease within 30days of randomization:a) Non-biologic therapies (e.g., cyclosporine, tacrolimus, thalidomide) other than thosespecifically listed in Section Permitted Medications for Treatment of UC.b) An approved non-biologic therapy in an investigational protocol.6. The patient has received any investigational or approved biologic or biosimilar agent (otherthan those listed in Exclusion Criterion #7) within 60 days or 5 half-lives prior to Screening(whichever is longer).7. The patient has previously received natalizumab, efalizumab, adalimumab, etrolizumab,AMG-181, anti–mucosal addressin cell adhesion molecule-1 antibodies, or rituximab.8. The patient has previously received vedolizumab.9. The patient currently requires or is anticipated to require surgical intervention for UC duringthe study.10. The patient has history or evidence of adenomatous colonic polyps that have not beenremoved, or colonic mucosal dysplasia.17
Infectious Disease Exclusion Criteria11. The patient has evidence of an active infection during the Screening Period.12. The patient has evidence of, or treatment for, C. difficile infection or other intestinalpathogen within 28 days prior to the first dose of trial drug.13. The patient has chronic hepatitis B virus (HBV) infection* or chronic hepatitis C virus(HCV) infection.* HBV immune patients (i.e., being hepatitis B surface antigen [HBsAg] negative and hepatitis Bantibody [HBsAb] positive) may, however, be included.14. The patient has active or latent TB as evidenced by the following:a) A diagnostic TB test performed within 30 days of Screening or during the ScreeningPeriod that is positive, defined as:– Positive QuantiFERON test or 2 successive indeterminate QuantiFERON tests, OR– A TB skin test reaction 5 mm.NOTE: If patients have received BCG vaccine then a QuantiFERON TB Gold test should beperformed instead of the TB skin test.ORb) A chest X-ray within 3 months of Day 1 that is suspicious for pulmonary TB, and apositive or 2 successive indeterminate QuantiFERON tests (or, a positive T-SPOT TBtest [Japan only]) within 30 days prior to Screening or during the Screening Period.18
Note: Patients with documented previously treated TB with a negative QuantiFERON test can beincluded in the study.15. The patient has any identified congenital or acquired immunodeficiency (e.g., commonvariable immunodeficiency, human immunodeficiency virus (HIV) infection, organtransplantation).16. The patient has any live vaccination within 30 days prior to Screening or is planning toreceive live vaccination during participation in the study.17. The patient has a clinically significant infection (e.g., pneumonia, pyelonephritis) within 30days prior to Screening, or ongoing chronic infection.18. The patient has used a topical (rectal) treatment with (5-ASA) or corticosteroidenemas/suppositories within 2 weeks of the administration of the first dose of trial drug.General Exclusion Criteria19. The patient has a history of hypersensitivity or allergies to vedolizumab or adalimumab.20. The patient has any unstable or uncontrolled cardiovascular disorder, heart failure moderateto severe (New York Class Association III or IV), any pulmonary, hepatic, renal, GI,genitourinary, hematological, coagulation, immunological, endocrine/metabolic, or other medicaldisorder that, in the opinion of the investigator, would confound the study results or compromisepatient safety.21. The patient has history of lupus or lupus-related conditions.22. The patient has had a surgical procedure requiring general anesthesia within 30 days prior toScreening or is planning to undergo major surgery during the study period.19
23. The patient has a history of malignancy, except for the following: adequately-treated nonmetastatic basal cell skin cancer; squamous cell skin cancer that has been adequately treated andthat has not recurred for at least 1 year prior to Screening; and history of cervical carcinoma insitu that has been adequately treated and that has not recurred for at least 3 years prior toScreening. Patient with remote history of malignancy (e.g., 10 years since completion ofcurative therapy without recurrence) will be considered based on the nature of the malignancyand the therapy received and must be discussed with the sponsor on a case-by-case basis prior toScreening.24. The patient has a history of any major neurological disorders, including stroke, multiplesclerosis, brain tumor, demyelinating, or neurodegenerative disease.25. The patient has a positive PML subjective symptom checklist at Screening or prior to theadministration of the first dose of trial drug at Day 1.26. The patient has any of the following laboratory abnormalities during the Screening Period: Hemoglobin 8 g/dL. White blood cells (WBC) 3 109/L. Lymphocyte 0.5 109/L. Platelet count 50 109/L or 1200 109/L. Alanine aminotransferase (ALT) or aspartate aminotransferase (AST) 3 upper limit ofnormal (ULN). Alkaline phosphatase 3 ULN. Serum creatinine 2 ULN.20
27. The patient has a history of drug abuse (defined as any illicit drug use) or a history of alcoholabuse within 1 year prior to the Screening Visit.28. The patient has an active psychiatric problem that, in the investigator’s opinion, mayinterfere with compliance with study procedures.29. The patient is unable to attend all the study visits or comply with study procedures.30. The patient is required to take excluded medications listed in Section 7.3.31. If female, the patient is pregnant or lactating or intending to become pregnant before, during,or within 5 months after participating in this study; or intending to donate ova during such timeperiod.32. If male, the patient intends to donate sperm during the course of this study or for 5 monthsthereafter.33. The patient is an immediate family member, study site employee, or is in a dependentrelationship with a study site employee who is involved in conduct of this study (e.g., spouse,parent, child, sibling) or may consent under duress.21
Prespecified Additional Outcomes in Protocol Clinical response (defined as a reduction in total score on the Mayo scale of 3 pointsand 30% from baseline [or a partial score on the Mayo scale of 2 points and 25%from baseline, if the total score on the Mayo scale was not performed at the visit] with anaccompanying decrease in rectal bleeding subscore of 1 point or absolute rectal bleedingsubscore of 1 point) at Week 52 Clinical remission (defined as a total score on the Mayo scale of 2 points and noindividual subscore 1 point) at Week 14 Rectal bleeding subscore indicative of mild disease ( 1) at Week 52 Physician’s Global Assessment (PGA) subscore indicative of mild disease ( 1) at Week52 Stool frequency subscore indicative of mild disease ( 1) at Week 52 Total score on the Mayo scale of 2 points and no individual subscore 1 point whererectal bleeding subscore of 0 and endoscopy subscore of 0 at Week 52 Endoscopy subscore of 0, rectal bleeding subscore of 0, and stool frequency subscoredecreases or no change from Baseline at Week 52 Endoscopy subscore 1, rectal bleeding subscore of 0, and stool frequency subscore of 0at Week 52 Endoscopy subscore 1, rectal bleeding subscore of 0, and stool frequency subscore 1 atWeek 52 Endoscopy subscore 1, rectal bleeding subscore of 0, stool frequency subscoredecreases or no change from Baseline, and total score (sum of these 3) 1 at Week 5222
Inflammatory Bowel Disease Questionnaire (IBDQ) score change of 16 points fromBaseline to Week 52 Clinical remission based on IBDQ score 170 at Week 52 Change in oral corticosteroid use from Baseline to Week 52 Discontinuation of corticosteroids as well as clinical remission at Week 14 amongpatients using corticosteroids at baseline Time to major UC-related events (e.g., hospitalizations, colectomies, and procedures) Change in fecal calprotectin concentrations from Baseline to Weeks 14, 30, and 52 Change in histology from Baseline to Week 52 Histological remission at Week 14 Histological remission at Week 52 Observed serum concentration at the end of a dosing interval (Ctrough) of vedolizumab Positive anti-vedolizumab antibodies (AVA) during the study Positive neutralizing AVA Safety for maintenance therapy as assessed by AEs, adverse events of special interest(AESIs, including serious infections including opportunistic infection such as PML, liverinjury, malignancies, infusion-related or injection site reactions or systemic reactions andhypersensitivity), serious adverse events (SAEs), vital signs, results of standardlaboratory tests (clinical chemistry, hematology, coagulation, urinalysis), and results of12 lead electrocardiograms (ECGs)23
Prespecified Exploratory Outcomes in Statistical Analysis Plan Clinical response at Week 14 Total score on the Mayo scale of 1 and rectal bleeding subscore 0 at Week 52 Durable clinical remission, defined as clinical remission at Week 52 amongst those inclinical remission at Week 14 (Note: the denominator will be the patients in the fullanalysis set) Clinical remission at Week 52 and in clinical remission for 14 weeks leading up toWeek 52. Clinical remission is defined by total score on the Mayo scale, or partial scoreon the Mayo scale if the total score on the Mayo scale was not performed at the visit(Note the denominator will be the patients in the full-analysis set) Disease control at Week 52, defined as total score on the Mayo scale of 2, rectalbleeding subscore 0, endoscopy subscore 0, C-reactive protein 5 mg/L, fecalcalprotectin (FCP) 100 ug/g and in histological remission (either by Geboes Score or byRobarts Histopathology Index) Rectal bleeding subscore 0 at Week 52 Major UC-related events (e.g., hospitalizations, bowel resection, and procedures)throughout the study up to Week 52 FCP 250 ug/g at Week 14, 30, 52 (among those with FCP 250 ug/g at baseline). (Notethe denominator will be a subset of patients with FCP 250 ug/g at baseline in the fullanalysis set) Treatment persistence with adalimumab or vedolizumab at Week 68 Change from baseline in IBDQ-specific domain at Week 30 and Week 52, includingbowel symptoms, systemic symptoms, emotional function, and social function24
Time to first clinical remission. Clinical remission is defined by total score on the Mayoscale, or partial score on the Mayo scale if the total score on the Mayo scale was notassessed at the visit Time to first clinical response. Clinical response is defined by total score on the Mayoscale, or partial score on the Mayo scale if the total score on the Mayo scale was notassessed at the visit Clinical remission by visit (e.g., Week 2, Week 4, Week 6, Week 14, Week 22, Week 30,Week 38, Week 46, Week 52). Clinical remission is defined by total score on the Mayoscale, or partial score on the Mayo scale if the total score on the Mayo scale was notassessed at the visit25
Statistical AnalysisThe first interim analysis was conducted after approximately 100 patients had been randomizedinto the study for 52 weeks and had completed the Week 52 Final Visit or Early TerminationVisit. The study design employed a prospectively planned interim analysis using a promisingzone design with an adaptive sample size re-assessment approach1 (conditional power derivedfrom the primary efficacy outcome of clinical remission at Week 52). This was conducted by anexternal independent statistical team. As prespecified in the protocol, the sponsor, investigators,and study participants were blinded to this interim analysis and its results. The Independent DataMonitoring Committee recommended the predefined maximum total sample size increase of 100patients.The primary efficacy analysis was performed when all patients had completed Week 52 orwithdrawn from the study (leaving 7 patients still to complete their Week 68 safety follow-up).This was for publication purposes. Final analyses included the off-treatment safety follow-up atWeek 68.1. Mehta CR, Pocock SJ. Adaptive increase in sample size when interim results arepromising: a practical guide with examples. Stat Med. 2011;30:3267-3284.26
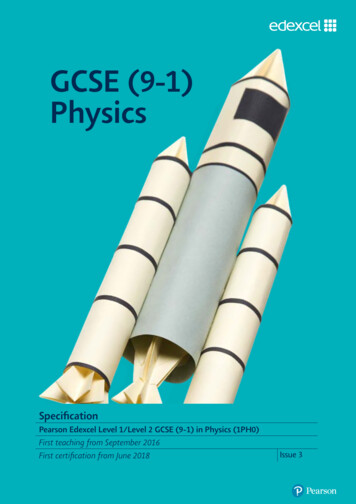
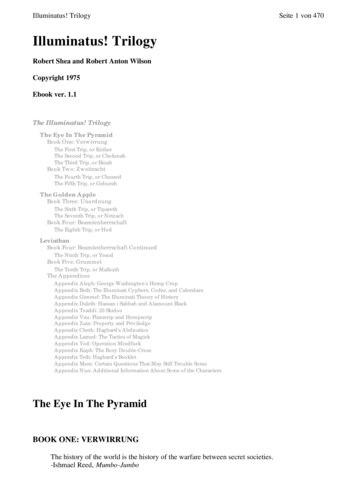
Figure S1. Patient Disposition.AE, adverse event; IV, intravenous; SC, subcutaneous.*Includes 2 patients randomized, but never received any study drug.27
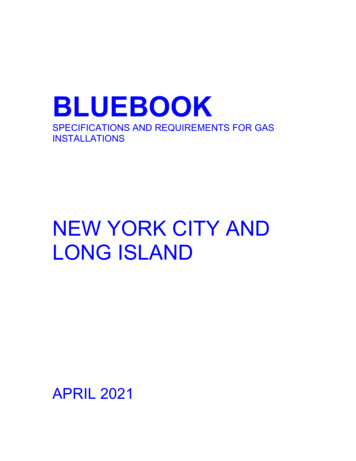
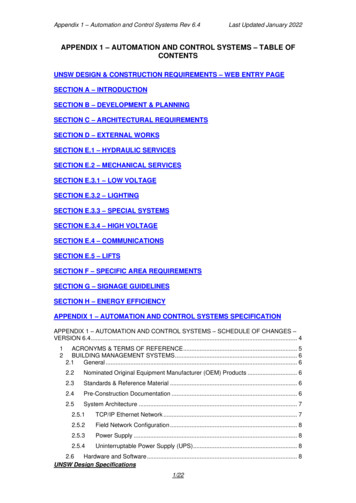
Figure S2. Clinical Remission at Week 52 in Subgroups by Patient Demographic andBaseline Characteristics (FAS).Plot of treatment differences (dots) and 95% confidence intervals (CIs; horizontal bars) forcomparing the proportion of patients in clinical remission between vedolizumab and adalimumabat Week 52.CI, confidence interval; FAS, full-analysis set; IV, intravenous; SC, subcutaneous; TNF, tumornecrosis factor; UC, ulcerative colitis.Clinical remission is defined as a total score on the Mayo scale of 2 points (or a partial score onthe Mayo scale of 2 points, if the total score on the Mayo scale was not assessed at the visit)and no individual subscore 1 point.Patients with missing clinical remission status are considered as non-responders.The 95% CI for the treatment difference is based on crude estimates using the normalapproximation method (the Fisher’s exact method used if the numerator is 5).28
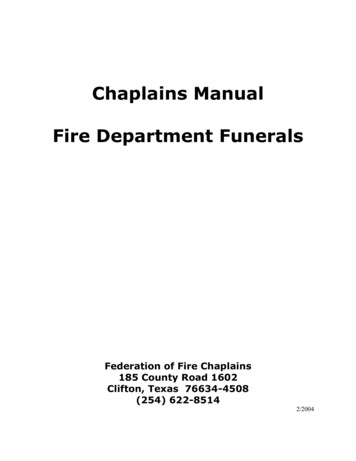
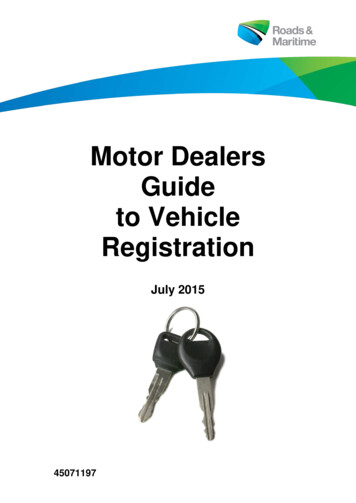
Figure S3. Clinical Remission and Endoscopic Improvement at Week 52 by BaselineConcomitant Medication Use.CI, confidence interval; eCRF, electronic Case Report Form; IV, intravenous; IWRS, interactiveWeb response system; SC, subcutaneousAbsence of baseline steroid use reflects data reported by IWRS. Absence of baselineimmunomodulator use reflects data reported on the eCRF.29
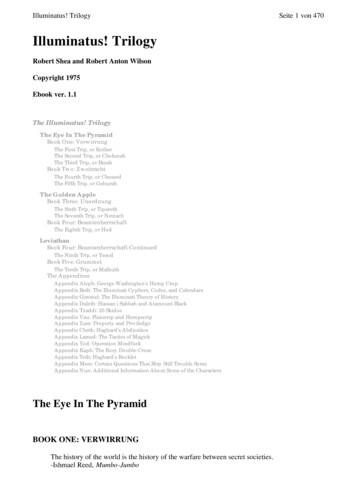
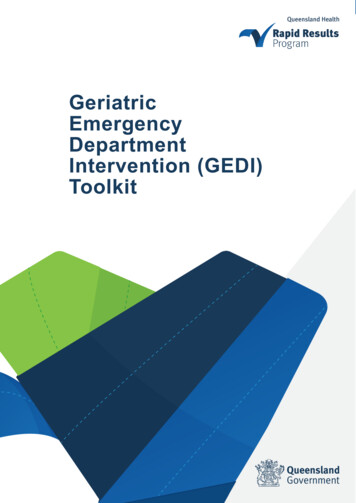
Figure S4. Clinical Remission at Week 14 in the Overall population and Subgroups byPrior TNF Inhibitor Therapy (FAS).CI, confidence interval; FAS, full-analysis set; IV, intravenous; SC, subcutaneous; TNF, tumornecrosis factor.Point estimate and 95% CI for the overall analysis were obtained from Cochran-Mantel-Haenszelmethod adjusted by randomization stratification factors: concomitant use of oral corticosteroids(Yes/No) and prior use of TNF inhibitor (Yes/No).Point estimates and the 95% CIs for TNF inhibitor subpopulations were obtained from CochranMantel-Haenszel method adjusted by randomization stratification factor: concomitant use of oralcorticosteroids (Yes/No) or the Fisher’s exact method if the numerator is 5.Patients with missing data to determine outcome status were considered as treatment failures;i.e., non-responders.30
Figure S5. Endoscopic Improvement at Week 52 by Patient Demographic and BaselineCharacteristics (FAS).Plot of treatment diffe
each dose of trial drug using a PML subjective symptom checklist, which assessed for any recent . routine on-site monitoring visits were performed by clinical research associates (CRAs) at all .