Transcription
OSHA and Infection Control Compliance:Checklists and ResourcesA single incident can put the health and welfare of your employees, studentsand/or patients at risk; therefore, safety MUST be a priority in every healthcareenvironment. While infection prevention may seem an overwhelming task, thereare resources available to help you walk this important path. This session willprovide a review of applicable regulations and the CDC recommendations fordental settings, as well as tools that can assist with overall compliance.Karen Gregory, RN2016 CADAT Annual Conference – Manhattan Beach MarriottSaturday, April 23, 2016
DisclaimerOSHA and Infection Control Compliance:Checklists and ResourcesKaren Gregory, RNTotal Medical ComplianceSponsored by: OSAP Karen Gregory is an employee of Total Medical Compliance,serves on the OSAP Board of Directors, a Hu‐Friedy KeyOpinion Leader, and a presenter for SciCan. No commercial support has been provided for this activity.Any reference to a commercial product is for examplepurposes only and does not reflect endorsement.Why Is IC Important in Dentistry?The Three “P’s”Learning Outcomes Explain the basic safety concepts outlined in the BloodbornePathogen Rule. Describe what changes are required by alignment of theHazard Communication Standard with the GloballyHarmonized System of Classification (GHS). Recall four critical (4) steps in instrument processing. Identify resources to assist with creating a safe environment. Potential exposure to pathogens for both patients andhealthcare workers Potential exposure to blood, oral and respiratorysecretions and contaminated surfaces/equipment Proper procedures can prevent transmission of infectionto patients and workersWorker AwarenessWorker awareness, Instrument processing, Surface decontaminationCare CAN Be Delivered Safely Safety CultureStandards – policies and proceduresOrientationTraining – OSHA and infection controlCompetency Demonstration – High Risk Areas Surface disinfection Instrument processing Worker exposure/health issuesSection A1
Infectious Hazards Hep B, C, HIVo HIV ‐ More than 1 million people are living with HIV.o Hepatitis B ‐ Over 1 million people living with chronic HBVinfection.o Hepatitis C ‐ Over 3 million people living with chronic HCVinfection. Herpes Staph, MRSA Chicken pox, measles, mumps Influenza, “colds”, enterovirus D‐68 TBChemical Hazards Disinfectants Surface High‐level Sterilants Dental procedure materials Bleach Chloform AmalgamPhysical HazardsWorker Safety Prevention is the KeyElectricalFireCutsFallsBurnsFlying objectsExposure to ionizing radiation Processing and exposure to salivaBloodborne Pathogen Standard ‐ 1991 Enacted to protect employees from exposure to HIV,hepatitis B, and hepatitis C Specifically defines what employers must do to protectemployees through job functions Must have written plan in place to outline safeguards A copy of the Bloodborne Pathogen Rule must beavailable during training If asked, you must provide a written copy of theExposure Control Plan to employeesSection APotential Routes of Transmission of BBPPatientDHCPDHCPPatientPatientPatient2
Reasons for Standard PrecautionsHepatitis B VaccinationHIV May have flu‐like symptoms or none at all People with HIV infection are often affected by viral hepatitis Risk of infection if exposed by needlestick is .3% Hepatitis B May have fever, joint pain, nausea, vomiting, weakness 50 ‐ 100 times more infectious than HIV Best protection? VaccinationHepatitis C May have fever, joint pain, nausea, vomiting, weakness Estimated that 3.2 million people living in the US with chronic HCVinfection, most not knowing they are ill 75 – 85% of people will move to chronic infectionFive Measures to Protect Against Exposure Hepatitis B vaccination made available toemployees who are occupationallyexposed: Free of charge at a reasonable time andplace After training and within 10 working daysof initial assignmentAnti‐HBs testing should be performed 1–2months last dose of the vaccine series Proof of series or declination on file Exception: Employee has been vaccinated Antibody testing reveals immunityExposure Determination Standard Precautions Everyone has the potential to spread infection Use of PPE Masks, face shields, goggles, gloves, gowns Engineering Controls Pieces of equipment to reduce the likelihood of exposure Work Practice Controls Employee behaviors to protect against exposure to blood or body fluid Surface/instrument decontamination Reduce the likelihood of patient to patient transfer of diseasePPE – Personal Protective Equipment Use based on task being performedEmployer must ensure properutilization of PPEMust be accessible, properly cleaned,laundered, repaired, and disposed ofat no cost to employeesRemoved when leaving area or uponcontamination List of job classifications inwhich all or some employeeshave occupational exposure. List of all tasks and/orprocedures in whichoccupational exposure occur. Exposure determination madewithout regard to the use ofPPE.Masks Required when contaminationof mucous membranes withbody fluids may occur throughsplashes or aerosolization Change between patients andif becomes moist during aprocedure May use in combination with aface shield or eye protectionAre people appropriately utilizing PPE?Section A3
Eye Protection Safety glasses Prescription glasses, but must beequipped with solid side shields Face shield Must be used in combination withmask to protect the nose and mouth Clean after use Clean and disinfect if visibly soiledGowns Reusable or disposable gowns, lab coats when clothing oruniform is likely to be soiled with blood or OPIM Change gowns at least daily or as soon as it becomes moist orvisibly soiled Remove barrier protection before leaving patient care areas Employer must launder contaminated protective clothingGloves Expected contact with blood, salvia, ormucous membranes Utilized for all pre‐clinical, clinical, postclinical, and lab procedures When touching contaminated surfaces Remove after patient care and if torn New pair for EACH patient. Cannot be washed for reuseNeedlestick Safety and Prevention Act Safety devices to be evaluated by theemployees’ utilizing the devices If using safety devices alwaysactivate the safety mechanism Feedback or work practice controlsHeavy Duty Utility Gloves Handling contaminated sharp items: during post procedure clean‐up in sterilization area when handling/using hazardous chemicals Puncture and chemical resistant, sizableMay wash or surface disinfectSome gloves can be sterilizedDiscard when cracked, peeling, torn,punctured or when ability to protect iscompromisedEngineering ControlsBlade RemoverRecappingDeviceSharps ContainerSafety AspiratingSyringeSection ACassettesSafety Scalpel4
Work Practice Controls Alter the way a task is performed Based on employee behavior instead of equipment One handed recapping of needles Only pass needles which are recapped Placing contaminated sharps immediately or as soon as possiblein a sharps container Do not reach by hand into container of contaminated sharps No eating, drinking, applying lipstick or contact lenses in areaswhere there is likelihood of exposure to blood or body fluidsEmployee Training – BBP No cost to the employee and during work hours At the time of initial assignment to tasks whereexposure may occur and annually thereafter Annual training within one year of previous training Within 90 days after the effective date of anychange in a standard An opportunity for interactive questions andanswersHazard Communication and GHSIdentify These Work Practices ControlsSafe transport ofsharpsEliminate reaching intoa container of sharpsMedical Record Employees at risk of exposure ‐ includes name, social security number HBV vaccination status Copy of results of examinations, medical testing, follow‐upprocedures. Employer’s copy of healthcare professional’s written opinion Copy of information provided to healthcare provider after exposure All incident reports Retained for duration of employment plus 30 years. If records requested provide a copy: To the employee or anyone with the employee’s written consent Director of NIOSH or HHS and/or Assistant Secretary of LaborHazard Communication and GHS Globally Harmonized System of Classification and Labeling(GHS) Collection of best practices by the United Nations Communicating severity of hazards of chemicals consistently Classification – Type of risk associated with use/exposure Labeling – Include pictograms, signal words, hazard statement Safety Data Sheets – Specified 16 section formatThis is the Year for GHSSection A Final compliance date June 1, 20165
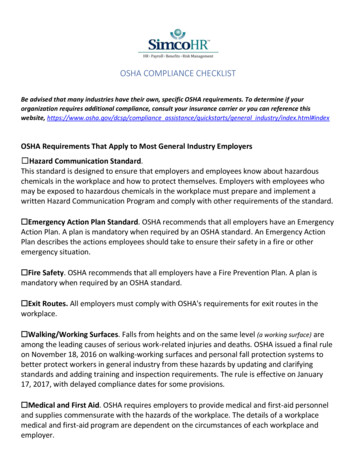
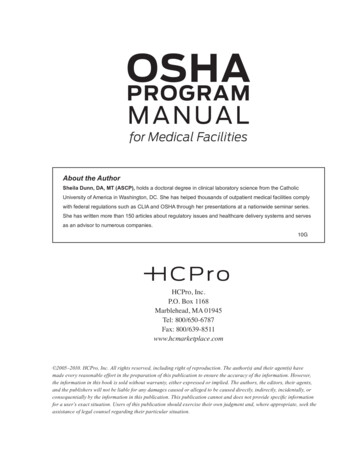
ToxiFlam (Contains: XYZ)GHS Manufacturer’s Labels Symbols ‐ Pictograms: Convey health and physical hazard information Signal Words: "Danger" or "Warning“. Only one signal word on a label Hazard Statements: Describes the nature of the hazard Precautionary Statements: Measures to minimize or prevent adverse effects First aid measuresSafety Data Sheet ReviewSection 2 – Hazard IdentificationSection 4 ‐ First‐aid measuresSection 6 ‐ Spill clean‐upSection 8 ‐ Personal protectionAn Exposure Has OccurredSignal WordDanger!Toxic If Swallowed,Flammable Liquid and VaporDo not eat, drink or use tobacco when using this product.Wash hands thoroughly after handling.Keep container tightly closed. Away from heat/sparks/open flame. – No smoking.Wear protective gloves and eye/face protection.Ground container and receiving equipment. Use explosion-proof electrical equipment.Take precautionary measures against static discharge.Use only non-sparking tools. Store in cool/well-ventilated place.IF SWALLOWED: Immediately call a POISON CONTROL CENTER or doctor/physician.Rinse mouth.In case of fire, use water fog, dry chemical, CO2, or "alcohol" foam.See Material Safety Data Sheet for further details regarding safe use of thisproduct.MyCompany, MyStreet, MyTown NJ 00000, Tel: 444 999 9999Compliance Date – June 1, 2016 Review the current status of MSDS and SDS sheets Reach out to vendors/manufacturers to obtain SDS, but notrequired Review the current inventory, consider elimination of any productsno longer used Educate supply personnel to retain any SDS received Manufacturers are only required to provide the SDS with thefirst shipment or first shipment if changes to the document Review new SDS for any change in hazards associated with the useand educate staffItems to Consider Who will mange the post exposure process Employee Health Occupational Medicine Emergency Departments/Urgent Care Difficulty in locating a care partner Worker’s Compensation provider Local dental societies Establish the relationship in advance Payment of services Wait times to be evaluated Rapid HIV testing for source patient Availability of post exposure medication Current with most recent guidance on bloodborne exposuresSection A6
What Are the Next Steps? Clean and flush Wash with soap and water for sharps injury to the skin Where is the closest eyewash for a splash to the face?Incident Evaluation Type and amount of bodysubstance involved Type of exposure percutaneous, mucousmembrane, intact/non‐intactskin, bites resulting in bloodexposure Report Who is the person to respond to these reports? Employees will be offered medical evaluation which mayinclude baseline testing, and counseling Source patient tested for Hepatitis B and C, and HIV Infection status of the source Susceptibility of the exposedpersonSource PatientExposed Worker Obtain patient consent based on state law Obtain testing if disease status is unknown HIV Antibody Obtain consent or declination for medical evaluationand counseling If employee declines HIV testing, offer the option todraw and hold blood for 90 days If source patient test results are negative forinfection, no further testing of employee will beindicated Rapid HIV test must be used if available If rapid HIV is not available, expedite the HIV test Hepatitis B Surface Antigen (HBsAG) Source patient testing is not indicated if exposed worker hasdocumented serologic evidence of hepatitis B immunity Anti‐Hepatitis C virus (Anti‐HCV)Environmental Infection ControlTesting Medical evaluation and counseling Conduct baseline testing of employee for all exposures: HIV Antibody Hepatitis B Surface Antigen (HBsAG) Testing of employee not indicated, if documented titer indicatesimmunity to hepatitis B. Anti‐Hepatitis C Virus (Anti‐HCV) Or test only if source patient testing indicates disease or anunknown exposure event Dependent on source patient test results additional testing forworker may occur for up to a 6 (six) month window.Section A Must maintain a clean and sanitary workplace Clinical Contact Surfaces High potential for direct contamination from spray or spatter orby touch Housekeeping surfaces Limited risk of disease transmission Clean on a routine basis7
Written Cleaning Schedule HousekeepingSurfacesCleaning and decontamination.Location within the facility.Type of surface to be cleaned.Type of soil present.Tasks or procedures beingperformed.May use barriers.Surfaces must be appropriatelydisinfected after completion ofprocedures with splash orsplatter blood or OPIM. CDCCleaning Housekeeping SurfacesClinicalContactSurfaces Include housekeepingsurfaces on cleaningschedule. Cal/EPA registered detergent‐ disinfectant prepared fresheach day. Mops and cloths – cleanedafter use, allow to dry or usedisposables. Consider break area andother non‐patient care areas.CDCTips on Barrier UseClean or Use Barriers Risk of transmitting infectionsgreater than for housekeepingsurfaces Surface barriers can be usedand changed between patients Clean surfaces Beginning of day End of day Barrier compromised Fluid proof If using plastic wrap mustmeet FDA weight for foodwrap Best to utilize commercialbarriersOR Clean then disinfect using anCal/EPA‐registered low‐(HIV/HBV claim) or when visiblysoiled an intermediate‐level(tuberculocidal claim) hospitaldisinfectantConsider: Saliva ejector holder Light switches Light handles Air‐water syringe handleCDCSection A8
Disinfection LevelsHigh – inactivates vegetative bacteria, mycobacteria, fungi,and viruses but not necessarily high numbers of bacterialsporesIntermediate – destroys vegetative bacteria, most fungi,and most viruses; inactivates Mycobacterium tuberculosisLow ‐ destroys most vegetative bacteria, some fungi, andsome viruses. Does not inactivate MycobacteriumtuberculosisEngineering Controls – Safety Devices Devices or equipment controlsthat eliminate, isolate orremove the bloodbornepathogens hazard from theworkplace. Safety devices are required bythe Needlestick Safety andPrevention Act. Comprehensive program ofdevices to reduce the likelihoodof a sharps exposure.Sharps Safety Avoid cleaning instruments chairside by hand or by wipingon the patient’s bib Utilize cotton rolls taped together for cleaning Purchase commercial product to avoid hand cleaning ofinstrument Grasps instruments by handle as opposed to “sharp” end Use great care when handling double‐ended instruments Only pass instruments one at a time Transport contaminated reusable sharps appropriatelySection ASurface Disinfection ‐ ReviewFollowmanufacturer’sinstructions foruseUse PPE ‐ Based onexposure potentialUtilize Two StepMethodSurfacedisinfectantcontact time?Cal/EPA registeredHospital DisinfectantDon‘t forgethandpiececradles, lightswitches, doorhandlesSharps Safety If needed, only pass needles which have been recapped Use needle re‐capper or one handed scoop method to recapused needles Dispose of non‐reusable sharps immediately in the area ofuse Remove burs immediately once no longer neededHand Hygiene Hands most common meansto spread pathogens Increased use of glovesincreased the need for hand‐hygiene Possibility of crosscontamination duringremoval or through breaks inglove material.9
Exudative Lesions or DermatitisDisinfection and SterilizationIf lesions on hands/wrists the DHCP must refrain from: Handling patient care equipment Handling devices used for invasive procedures All direct care activities likely to have contact withlesionHow to Proceed State law – Must post CaliforniaDental Board IC regulations Manufacturer’s validatedinstructions for use CDC Spaulding System Policies and proceduresDisinfection and SterilizationEH SpauldingHow an object is processed depends on the object’s intended use. CRITICAL ‐ objects which enter normally sterile tissue or the vascularsystem or through which blood flows should be sterile. SEMI‐CRITICAL ‐ objects that touch mucous membranes or skin thatis not intact require a disinfection process (high‐level disinfectionHLD) that kills most microorganisms except for high numbers ofbacterial spores. NONCRITICAL ‐objects that touch only intact skin require low‐leveldisinfection.Section AQuestions to Ask Is there an appointed individual to oversee all infectioncontrol standards? Can you locate the manufacturer’s validated instructions foruse on all equipment, including instruments utilized? Are written policies in place for instrument cleaning,disinfection, sterilization? Have workers been trained? Is there written proof of workers competency and training?Critical Instruments Penetrate mucous membranes or contact bone, thebloodstream, or other normally sterile tissues (ofthe mouth) Heat sterilize between uses or use sterile single‐use,disposable devices Examples include surgical instruments, scalpelblades, periodontal scalers, and surgical dental burs10
Semi‐critical Instruments Contact mucous membranes but do notpenetrate soft tissue Heat sterilize or high‐level disinfect Examples: Dental mouth mirrors, amalgamcondensers, and dental handpiecesNoncritical Instruments and Devices Contact intact skin Clean and disinfect using a low tointermediate level disinfectant Examples: X‐ray heads, facebows, pulseoximeter, blood pressure cuffGuidelines for Infection Controlin Dental Health‐Care Settings — 2003 Use only FDA‐cleared medical devices for sterilization and followthe manufacturer's instructions for correct use. Clean and heat‐sterilize critical dental instruments before each use. Clean and heat‐sterilize semi‐critical items before each use. Use of heat‐stable semi‐critical alternatives is encouraged. Reprocess heat‐sensitive critical and semi‐critical instruments byusing FDA‐cleared sterilant/high‐level disinfectants or an FDA‐cleared low‐temperature sterilization method (e.g., ethylene oxide).Dental Handpieces and Other DevicesAttached to Air and Waterlines Clean and heat‐sterilize handpieces and otherintraoral instruments that can be removed from theair and waterlines of dental units between patients. Follow the manufacturer's instructions for cleaning,lubrication, and sterilization of handpieces and otherintraoral instruments. Do not surface‐disinfect, use liquid chemicalsterilants, or ethylene oxide on handpieces and otherintraoral instruments that can be removed from theair and waterlines of dental units.Dental Board Specifics All high‐speed dental hand pieces, low‐speed handpieces, rotary components and dental unit attachmentssuch as reusable air/water syringe tips and ultrasonicscaler tips, shall be packaged, labeled and heat‐sterilized in a manner consistent with the samesterilization practices as a semi‐critical item.Steps in the Process CleaningPackagingSterilization or disinfectionMonitoring Physical Chemical Biological StorageSection A11
Divide and ConquerCleaning ‐ First Step Must utilize PPE Limit hand‐washing ofinstruments Ultrasonic cleaner Equipment must becleared by the FDA Rinse and DRYinstruments prior topackaging Establish the flow in theinstrument processing area Receiving, cleaning, anddecontamination Preparation and packaging Sterilization StorageCourtesy of Andrea CookPreparation and PackagingCDC Guidance Elimination /destruction of all forms of microbial life Heat Based Steam under pressure (autoclaving) Use an internal chemical indicatorin each package. If the internalindicator cannot be seen fromoutside the package, also use anexternal indicator . Use a container system orwrapping compatible with thetype of sterilization process usedand that has received FDAclearance. Gravity displacement Pre‐vacuum Dry heat Unsaturated chemical vapor ChemicalSteam Sterilization Advantages Non‐toxic Cycle easy to control andmonitor Inexpensive Rapidly microbicidal Least affected byorganic/inorganic soils Rapid cycle time Penetrates medicalpacking, device lumensSection ASterilization Disadvantages Potential for burns Inappropriate for heat ormoisture sensitiveinstruments Dulling RustingSteam Sterilizers Loading Allow for circulation Dry non‐porous containersmust be positioned so thatwater will run out Non‐perforated trays on edge All peel packs on edge All instruments open Maintain dedicated loads12
Packaging Peel packs – limit numberof instruments/weight Rigid containers Self seal roll stock Sterile wraps woven andnon‐woven Compatible withsterilization method Must be FDA clearedPackage Labeling Date Sterilizer number if morethan one unit Load number Record on plastic side ofpeel pouches or onsterilization tape Ink that does not run3/31/2016Dry Heat Sterilization Transfers heat energy from airinside the oven to theinstruments Good for items that are likely todull or rust in the autoclave, Good for powders, cellulose andink Packaging must be able towithstand high temperatures Utilize internal and externalindicators Ensure proper spore testing isperformedStorage of Sterile Items Event‐related shelf life recognizes that the product remainssterile until an event causes it to become contaminated (e.g.moisture). Time related – Remains sterile for an assigned period of timebased on packaging type. Packages should be evaluated before use for loss ofintegrity. Repack and reprocess if compromised.Section AStorage of Sterile Items Well ventilated to protectagainst dust and moisture. Consistent temperature andhumidity. Packaging should includeload number, sterilizationdate, and expiration date ifindicated. Packages should not bestored resting on top of eachother.Chemical Disinfectants/Sterilant Use of heat‐stable semi‐criticalalternatives is encouraged. Reprocess heat‐sensitive criticaland semi‐critical instruments byusing FDA‐cleared sterilant/high‐level disinfectants or an FDA‐cleared low‐temperaturesterilization method(e.g., ethylene oxide).13
Chemical Disinfectants/Sterilant Prepare solution according to manufacturer’sinstructions and record expiration date Clean Rinse and dry Soak for appointed time Remove and rinse Test strip solution each day of use according tomanufacturer’s instructionsSterilization Monitoring Physical ‐ cycle time,temperature, pressure Chemical ‐ heat or chemicalsensitive inks that change colorwhen germicidal‐relatedparameters reached Biological ‐ Bacillus spores thatdirectly measure sterilizationTypes of Indicators ‐ AAMI Class 1 – process indicator Class 2 – Bowie Dick –(dynamic air‐removal only) Class 3 – Single‐variable Class 4 – Multi‐variable Class 5 – Integrating indicator Class 6 – Emulating indicator– load specificChemical Indicators External indicator – Providesvisual of sterilization process Internal Chemical Indicator Visual sterilant penetrated thepack or tray Pack control monitor ‐ packagesin multiple locations Detect local problemBiological Monitors Perform weekly and withimplants Types: Steam – Geobacillusstearothermophilus Dry heat – B. atrophaeus(formerly B. subtillis) ETO – B. atrophaeusAPIC Disinfection/Sterilization2005. WA RutalaSection A14
Positive Spore TestPositive Spore Test Following a single positive biologicalindicator: Remove the sterilizer from service andreview sterilization procedures (e.g., workpractices and use of mechanical andchemical indicators) to determinewhether operator error could beresponsible. Retest the sterilizer by using biological,mechanical, and chemical indicators. Repeat spore test is negative, put thesterilizer back in service If REPEAT test positive:PositiveA NEVER Event Ensure instruments are safe foruse: Packaging is intact – sealedappropriately. External indicator has changedcolor. Internal indicator has changedcolor. Instruments show no visibleevidence of contamination.Dental Laboratory Splash shields and equipment guards usedon dental laboratory lathes Fresh pumice and a sterilized or new rag‐wheel used for each patient Devices used to polish, trim, or adjust contaminated intraoral devicesmust be disinfected or sterilized, properly packaged or wrapped andlabeled If packaging is compromised, re‐clean the instruments, re‐package,and re‐sterilize Store sterilized items to prevent contaminationSection A Do not use the sterilizer until it has been inspected or repaired orthe exact reason for the positive test has been determined. Recall, to the extent possible, and reprocess all items processedsince the last negative spore test. Before placing the sterilizer back in service, re‐challenge thesterilizer with biological indicator tests in three consecutive emptychamber sterilization cycles after the cause of the sterilizer failurehas been determined and corrected. Maintain sterilization records (physical, chemical and biological)Dental Laboratory Communication – protocols andresponsibilities. Clean or dirty lab area on site? Materials, impressions, andintra‐oral appliances must becleaned and disinfected beforebeing handled, adjusted or sentto out to dental lab. Select and followmanufacturers’ directions forproper chemical based on typeof dental material in use.Dental Unit Water Lines For routine dental care, the ADA and the CDC recommendusing water that meets EPA standards for drinking water(i.e., 500 CFU/mL of heterotrophic water bacteria) Consult with the dental unit manufacturer for appropriatemethods and equipment to maintain dental water quality Follow recommendations for monitoring water qualityprovided by the unit manufacturer or waterline treatmentproduct15
Why the Concern? Small diameter of dentalwaterline tubing, design and flowrate, enable bacteria and othermicroorganisms to form a biofilm. Coats lining of tubing and mayslough off resulting incontamination of the water. 82‐year‐old otherwise healthywoman who developedLegionnaire's disease after adental visit.Single‐Use (Disposable) DevicesPossible Solutions Treatment of dental unit waterlines At the beginning of each workday Purge dental unit lines and devices with air orflushed with water for at least two (2)minutes prior to attaching handpieces,scalers, air water syringe tips, or otherdevices. Flush dental unit lines and devices betweeneach patient for a minimum of twenty (20)secondsSingle Use Items Intended for use on one patient during asingle procedure Solutions/medications typically do not havepreservatives Usually not heat‐tolerant Cannot be reliably cleaned Examples: Syringe needles, prophylaxiscups, and plastic orthodontic brackets FDA Law prevents reuse of “labeled” singleuse patient products or devicesDispose Appropriately“Regulated Waste” means waste that is any of the following: (1) Liquid or semi‐liquid blood or OPIM; (2) Contaminated items that: (A) Contain liquid or semi‐liquid blood, or are caked with dried blood or OPIM;and (B) Are capable of releasing these materials when handled or compressed. (3) Contaminated sharps. (4) Pathological and microbiological wastes containing blood or OPIM. (5) Regulated Waste includes “medical waste” regulated by Health and SafetyCode Sections 117600 through 118360.Section APracticing in the Real World Continuing education New kid on the block We didn’t learn that in school!16
Dental Laboratory Clean impression with a camel hairbrush. Disinfect for proper period of time –must stay “wet” for label contacttime. Surface disinfectants are nottested/approved for reuse (soaks). Rinse thoroughly. Do not transfer to laboratory incontainer containing disinfectant.Radiology Follow manufacturer’srecommendations on barrier protectionand cleaning and disinfection of digitalsensors. XCP (extension cone paralleling) filmholder positioning system ‐ heat sterilizeor HLD based on use Dispensers Devices used to deliver to site inthe mouth impression materials adhesives dental composites endodontic (root canal)materials3/31/2016Do Avoid contact of the reusable parts (e.g., the body of themultiple‐use dental dispenser) with the patient’s mouth Apply disposable barrier sleeves/wraps over multiple‐usedental dispensers before use with each patient Use new, uncontaminated gloves when handling multiple‐use dental dispensers Dental assistants dispense material for the ndMedicalProcedures/DentalProducts/ucm404472.htmDo Not Reuse the multiple‐use dental dispenser if contaminated Reprocess a contaminated multiple‐use dental dispenser byusing chemical wipes or disinfectants Immerse multiple‐use dental dispensers in a high level chemicaldisinfectant. May damage the dispenser and material in the device Sterilize multiple‐use dental dispensers. May damage the material in the deviceSection AThank You!Contact InformationKaren Gregory, RNDirector of Compliance and MedicalCompliance.com888.862.674217
OSHA and Infection Control Compliance: Checklists and Resources A single incident can put the health and welfare of your employees, students and/or patients at risk; therefore, safety MUST be a priority in every healthcare environment. While infection prevention may seem an overwhelming task, there