Transcription
DOCUMENT RESUMEED 263 176AUTHORTITLEPUB DATENOTEPUB TYPEEDRS PRICEDESCRIPTORSIDENTIFIERSTM 850 666Dawson-Saunders, Beth; And OthersPredicting MCAT Examination Scores.Apr 8518p.; Paper presented at the Annual Meeting of theAmerican Educational Research Association (69th,Chicago, IL, March 31-April 4, 1985).Speeches/Conference Papers (150) -- Reports Research /Technical (143)MF01/PC01 Plus Postage.*College Entrance Examinations; EducationalCounseling; Grade Point Average; Higher Education;Longitudinal Studies; *Medical Schools; *PredictiveMeasurement; *Predictive ValidityACT Assessment; Medical College Admission TestABSTRACTAcceptable performance on the Medical CollegeAdmissions Test (MCAT) is necessary for acceptance into medicalschool; therefore, students planning a career in medicine and theiradvisors would benefit by having information useful in predictingperformance on this examination. The present study examined theialidity of the ACT Assessment as such a predictor, using as subjects197 undergraduate students at a large midwestern university whoapplied to the medical school during a five year period. The resultsindicated th t the ACT composite score was strongly related to MCATperformance, though the predictability was enhanced by inclusion ofinformation on the student's grade point average in science subjects:multiple R's runged from .57 for predicting MCAT reading to .62 forbiology. Used appropriately, these results will be beneficial toundergraduate students, pre-medical advisors, and others indetermining the need for remedial coursework and deciding when totake the MCAT examination. ****** -***********************Reproductions supplied by EDRS are the bmz that can be madefrom the original ******************************
Predicting MCAT Examination Scores.1)N.r-4te1.0C\Jc:aLiiBeth Dawson-Saunders, Ph.D., Rosalia E.A. Paiva, Ph.D.,and Deane R. Doolen, M.A.Southern Illinois UniversitySchool of MedicineSpringfield, ILU.S DEPARTMENT OF EDUCATIONNATIONAL INSTITUTE OF EDUCATIONEOUCAT1ONAL RESOURCES INFORMATION.LATER (ERIC)0 This document has been reproduced as,.rued from the person or organizationoriginating it.i Minot changes have been Tide to improvereproduction Quality.Points of vow or opinions stated in this docu.mint do not necessarily repter.ont Ott icial MEposition Of POLCY"PERMISSION TO REPRODUCE THISMATERIAL HAS BEEN GRANTED BYB. -7)6 up SnY1 -Si ILINckSTO THE EDUCATIONAL RESOURCESINFORMATION CENTER (ERIC\Sli.5.9Paper presented at the annual meeting of the American Educational ResearchAssociation, Chicago, April 1985.0LnDo2
AbstractAcceptable performance on the MCAT examination is necessary foracceptance into medical school; therefore, students planning a career inmedicine and their advisors would benefit by having information useful inpredicting performance on this examination.The ,.resent study examined thevalidity of the ACT examination as such a predictor, using as subjects197undergraduate students at a large midwestern University who applied to themedical school during a five year period.The results indicated that the ACTcomposite score was strongly related to MCAT performance, although thepredictability was enhanced by inclusion of information on the student'sgrade point average in science subjects:multiple R's ranged from .57 forpredicting MCAT reading to .62 for biology.Used appropriately, theseresults will be beneficial to undergraduate students, pre-medical advisorsand others in determining the need for remedial coursework and deciding whento take the MCAT examination.3
Professional educational activities include counselling and advisingfunctions as well as teaching.Advice on strategies to gain admission toprofessional and graduate schools is an important component of thecounselling process.Admission to most U.S. and Canadian medical schoolsdepends upon three factors:undergraduate grade point average, scores on theMCAT examination, and other dimensions such as interview performance or otherevidence of interpersonal skills and behavior-related factors (1-5).Pre-medical advisors and others who counsel undergraduate students regardingcareers in medicine provide guidance on coursework, when to take the MCATexamination, schools to apply to, and general strategies for gainingadmission.From the personal experience of one of the authors (ORO),pre-medical advisors initially use grades, especially those inscience-related subjects, as indicators of success.Once students have takenthe MCAT examination, advisors may recommend application to medical schoolor, in the case of low scores, may suggest further coursework or specialstudy followed by another try at the MCAT.(In extreme cases, of course,they often counsel alternate career choices.)Even though the MCATexamination is not an educational outcome in itself, its utility as an indexfor medical school selection makes it desirable for students to score well.Therefore, undergraduate students aspiring to a career in medicine and theiradvisors would profit by being able to "predict" how well they will do on theMCAT examination.It may be that coursework of a remedial nature can beundertaken prior to the expense of taking the MCAT examination.Natural candidates for such predictors are the standardized examinationsstudents take for admission to college itself, such as the SAT and ACT.
There appears to have been little research on the applicability of the SAT orACT examinations to predict measures other than undergraduate performance ofstudents.The SAT was evaluated for its potential as an indicator ofperformance in one U.S. medical school over a ten year period (6), and it wasfound that four subgroups, based on each of the verbal and mathematicssubtests scores, were different with respect to their subsequent performanceon some criteria of success in medical school.In a discussion of thevalidity of the SAT and the MCAT, the authors noted correlations (notcorrected for restriction of range) of .55 between SAT verbal and MCAT verbaland of .37 between SAT mathematics and MCAT science.The predictive validity of the ACT for success in nursing school wasexamined in two studies.One study examined data over a ten year period todetermine whether the ACT subtests have incremental validity in predictingsuccess in the nursing curriculum itself (7).Another study examined thecapability of the ACT score and other measures to predict performance on theState Board Examination in Nursing (8).The stability of prediction,independent of undergraduate major, was examined using a national sample ofcolleges participating in the ACT testing program between 1972 and 1977 (9).Although the correlations across the four study years were stable, theanalysis was based upon high school grade point average as well as ACTscores, and no results were presented for these latter scores alone.A review of several past volumes of the primary journals devoted toresearch in medical education and computerized literature searches on MEDLINEand ERIC failed to disclose additional sources.Therefore, the present studywas designed to evaluate the efficacy of the ACT as a predictor ofperformance on the MCAT examination.Since students and pre-medical advisors-2-
also have information on the undergraduate grade point averages--both inscience subjects and in nonscience subjects--the incremental validity of thisinformation was also evaluated.It was expected that the ACT English andmathematics subtests would correlate highest with their MCAT counterparts andthe ACT natural science with MCAT biology and science problems.The gradepoint averages were expected to add significantly to all the predictionequations.MethodSubjects were students attending Southern Illinois University (SIU) atboth Carbondale and Edwardsville campuses who applied for admission to theSIU School of Medicine during the years 1978 through 1982.Only thoseapplicants who had been students at SIU and had ACT scores on file with theUniversity were included.Computer tapes provided the School of Medicine bythe Association of American Medical Colleges were the source for dataelements from the AMCAS biocard.In addition to biographic information,these elements included the MCAT subtest scores and cumulative undergraduategrade point average (GPA) in nonscience subjects (AO) and in science subjects(BCPM) at the time of application.All MCAT scores were based on the newexamination, and if taken more than one time, the scores from the firstadministration were used for analysis.The data were analyzed using the Statistical Package for Social Sciences(SPSSX).In addition to basic descriptive statistics, correlation andregression analyses on each of the six MCAT scores were performed.If twoindependent variables were highly correlated, one was eliminated to reduceeffect.5 multicollinearity.ACT subtest scores with regressioncoefficients significant at .10 were retained in the equations.-3-In the
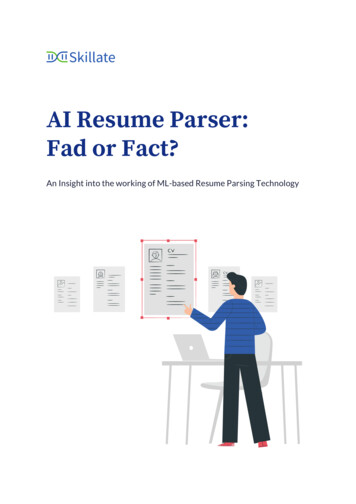
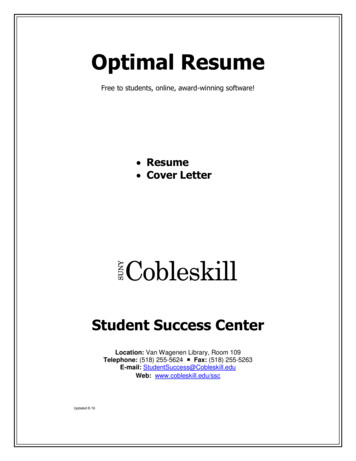
incremental analysis, a variable was retained only if its addition wassignificant at p .05.The analysis was then repeated using the ACTcomposite score in place of the four subtest scores.The sample was thenrandomly divided into two parts and the analytic procedures repeated on eachsubsample for a double cross-validation analysis.ResultsThe search of the AMCAS computer tapes for the medical school applicantyears from 1978 through 1982 resulted in 364 students who had been enrolledat Southern Illinois University--Carbondale or Edwardsville.Universityrecords had ACT examination scores on file for 197 of these students,indicating that the remaining 167 applicants had matriculated asundergraduate transfers or as graduate students.Of the 197 students forwhom complete data were available, 19.8% of the applicants were female.MeanMCAT scores ranged from 8 to 9, with s'Indard deviations of approximately 2.The mean nonscience (AO) GPA was 3.56; the mean science (BCPM) GPA was 3.31;both had a standard deviation less than 0.5.Mean ACT scores ranged from21.5 in English to 27.7 in natural science; standard deviations wereapproximately 4.This sample included 54 applicants who were subsequentlyadmitted to the medical school at SIU.The correlations among all continuous variables are given in Table 1.The two GPA's were correlated at .72.The ACT composite score was highlycorrelated (.73 to .82) with all ACT subtest scores.The correlationsbetween the ACT and MCAT subtests were generally in the .30's and .40's.Ashypothesized, the MCAT quantitative subtest was most highly correlated withACT mathematics.The MCAT reading and science problems, however, werecorrelated most highly with ACT social science scores, which also correlated-4-7
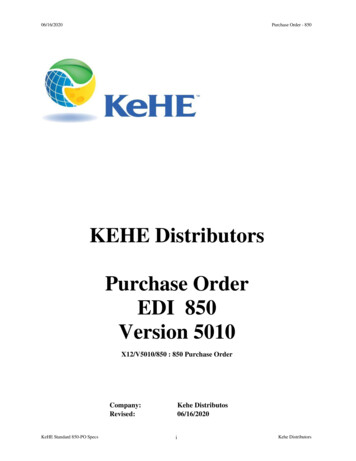
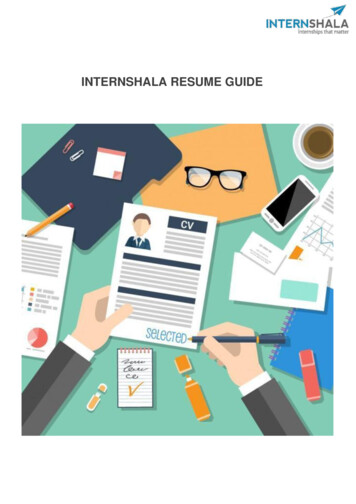
as highly with MCAT biology as did ACT natural science.Correlations betweenthe composite ACT and MCAT scores were higher, however, ranging from .43 to.55.All but three interset correlations were significant at p.001.The regression equations based upon individual ACT scores using the totalsample produced multiple correlation coefficients ranging from .480 for MCATchemistry to .561 for MCAT reading (Table 2A).Because of the highcorrelation between the GPA's, only the BCPM grade point average was used inthe incremental regression analyses.The results indicated a significantimprovement over the prediction based on ACT scores alone in all scores; themultiple R's ranged from a low of .584 for physics to a high of .623 forbiology.The addition of sex produced small but significant increases(p .05) for prr-di tilg all subtests except biology and reading, with malespredicted to score higher.Regression equations are given in Table 3.Because of the relatively high correlations between the composite ACT itssubtests, the analyses were duplicated regressing on ACT composite in placeof the four ACT subtest scores (Table 2B).Comparison of correlations basedon dependent samples (10) indicated no significant differences (p .05)between these results and those based upon using ACT subtests.The additionof the BCPM GPA resulted in regression results similar to those achievedusing individual subtest scores, and the addition of sex increased allpredictions except MCAT reading (Table 3).The cross-validation analysis generally resulted in similar-sizedmultiple correlations in the two subsamples (Table 2).The apparentexception was the prediction of the MCAT physics subtest; however, the-5-
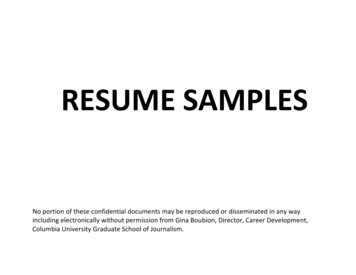
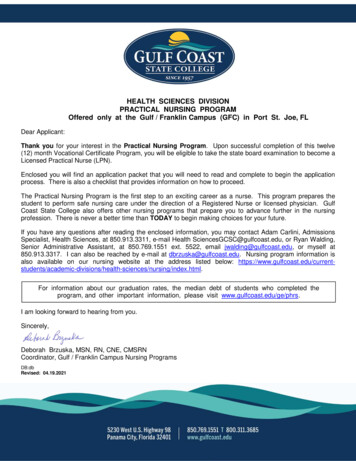
differences were not significant (p,.05) after the addition of the BCPM SPAto the regression equation.There was some variation between the twosubsamples in the magnitude of the regression coefficients, given in detailfor the regression on composite score in Table 4, and also indicated by theinconsistent results for the addition of the sex variable to the regressionon ACT component scores (Table 2A).None of the differences in regressioncoefficients was significant at p.4.05, however.The cross-validationmultiple correlations obtained by applying the regression equation from onesubsample to the other (Table 4) show an amount of shrinkage generally withinthe expected ranges predicted by the Wherry or Olkin Pratt formulae (11).Only in the prediction of the quantitative subtest did the observed values ofthe cross-validation R depart from the predicted value based on the aboveformulae by more than .05.Therefore, the regr:ssion equations based uponthe entire sample are justified and can be used on similar samples with someconfidence in their predictions.Discussion and ConclusionsThe present study has demonstrated the usefulness of both the ACTcomponent scores and composite score in predicting the MCAT subtest scores.The prediction is significantly enhanced with the addition of the nonscience(BCPM) grade point average to the regression on all MCAT subtests and withthe sex of the students on all except reading and quantitative.Thesefindings should be very useful to students and pre-medical advisors atundergraduate schools that have ACT and MCAT score distribution similar tothose observed in the present study; i.e., mean ACT composite of 25 with astandard deviation of 4 and slightly negatively skewed, and mean MCAT scores-6-
of 8 to 9 with standard deviations of 2 and slight negative skewness.Theseresults may not generalize to highly competitive undergraduate environmentsin which the scores are significantly different or the range of scores ismore restricted.The present study should be replicated in universitysettings in which the selection criteria produce a student population morehomogeneous than that at Southern Illinois university.With the above caveat in mind, pre-medical advisors may find theprediction equations produced in this study of use with their advisees andpre-med clubs.Many medical schools utilize a cut-off score, especially onthe science problems subtest of the MCAT.For example, SIU uses the sixtiethcentile (a score of 8) as a recommended selection factor.In order to obtaina predicted science problems score of 8 with a science grade point average of3.5, a student would require an ACT composite score of 20 if a male and 25 ifa female or (found by substituting the appropriate values in the equation inTable 3).This calculation represents the ACT score needed to predict a meanscience problems score of 8, and a pre-medical advisor might suggest the needfor a higher GPA with an ACT composite in the range of 20 to 25 to increasethe likelihood of a score of 8.AlternateL, it may be appropriate for thestudent to take additional science coursework or a review course designed toincrease performance on the MCAT.Of course, many factors affect how any given student will perform on anational, standardized examination, such as the MCAT.That past performanceon the ACT examination is indicative of future performance on the MCAT is notterribly surprising.The present study, however, has attempted to formalizethis relationship in a way that is useful to students who wish to apply to-7-10
medical school and to the people who advise and counsel them.It is hopedthat these students, their parents, and advisors will find the relationshipsderived in this study a useful addition to the other information typicallyused in career planning and counselling.-8-11
References1. Milstein, R.M., Wilkinson, L., Burrow, G.N., and Kessen, W.Decisions and Performance During Medical School.""AdmissionJ. Med. Educ 56:77-82, 1981.2. Benor, D. and Hofboll, S.E."Prediction of Clinical Performance:Role of Prior Expectation."3. Yens, D.P. and Stimmel, B.J. Med. Educ., 56:653-658, 1981."Science Versus Nonscience UndergraduateStudies for Medical School:57:TheA Study of Nine Classes."J. Med. Educ.,429-435, 1982.4. Schermerhorn, G.R., Colliver, J.A. and Kolm, P.Interviewing:"SelectiveIdentifying Congruence with Institutional Goals AmongAcademically Qualified Medical School Applicants."Education:Research in Medical1982 Proceedings of the Twenty-First Annual Conference,199-204, 1982.5. Stokes III, J. and Martin, M."Changes in Medical School ApplicantPreparation and Admission Requirements in the Behavioral Sciences."Med. Educ., 58:J.58-59, 1983.6. Zeleznik, C., Hojat, M., and Veloski, J."Long-Range Predictive andDifferential Validities of the Scholastic Aptitude Test in MedicalSchool."Educ. & Psych. Meas., 43:7. Halpin, G. and Halpin, G.223-232, 1983."Incremental Validity of the ACT Test Batteryfor Predicting Success in a School of Nursing over a 10-Year Period."Educ. & Psych. Meas., 36:433-436, 1976.-9-12
8. King, Jr., J.R."Prediction of Nursing State Board Test Pool ExaminationPerformance from ACT, NLN Achievement Test Scores, and College GradePoint Averages."Dissertation Abstracts International, 39:9. Sawyer, R. and Maxey, J.Equations over Time.""The Validity of College Grade PredictionJ. Educ. Meas., 16:10. Glass, G.V. and Stanley, J.C.Psychology, p. 313-314.279-284, 1979.Statistical Methods in Education andEnglewood Cliffs, NJ:11. Kendall, M.G. and Stuart, A.Ed.), Volume 2.2147, 1978.New York:Prentice-Hall, Inc., 1970.The Advanced Theory of Statistics (2ndHarper, 1967.
Table 1:Correlations Among All Variables*ACTEngACTEnglishMathematicsSocial ScienceNatural ScienceCompositeGPAAll 49.76.23.49.40.56PhysicsScience ProblemsReading.43Quantitative*Two-tailed critical values require r .14 at p .05; r .19 at p .01; r .24 at p .001.14
Table 2:MCAT SubtestPredictedSamp 1Multiple Correl ation Coefficients for Cross Validation SamplesA.Using ACT Subtest ScoresACT's onlySamp 2 TotalAddin BCPMamp 2 Tail-Samp 1A c 1( 4:684.534.613Sci AT 92.383.443Physics.552.207Sci Prob.564ReadingQuantNote:.658.630.654.610Using ACT Composite ScoreACT's onlymSaal Samp 2.691TaiTiAdding BCPMSamp .561.547.553.556.549.554Adding SexSamp 2 .586.625.577.576.574.594.583.587Blanks indicate no significant increase in R at p .05.16-12-.624.602
Table 3:MCAT SubtestPredictedagRegression Equations for Entire SampleUsing ACT Subtest scoresMath SSciNSciBCPM SexBiology-.07 *.07.061.69Chemistry**.08*1.66Physics*.07*.09Sci Prob**.09Reading**Quant.08 .10ConstUsing ACT Composite ScoreBCPM ression coefficient not significant (p .10).Blanks indicate no significant increase in R at p .05.07.62-1.45
Table 4:MCAT SubtestPredictedBiolChemPhysSci ProbReadingQuantRegression Equations Using ACT Composite ScoreCompositeBCPMn 197n 98n 99.10.09.141.771.522.12n 197n 98n 99.12.09.161.701.761.72n 197n 98n 99.13.17.07n 197n 98n 99Sample.Sex.63Constant.11R.615.627.662Cross-,Val. 4-2.31.625.645.586.637.533n 197n 98n 99.25.22.29.65.62.78.07.87-1.52.574.577.576n 197n 98n 7.881.16.82.592.610.509.511.506 .450 (1) The first correlation is between the actual and predicted subtest scores in thefirst sample using the second sample regression equation; the second correlation isbetween the actual and predicted subtest scores in thes second sample using the firstsample regression equation.Blanks indicate no significant increase in R at p .05. Cross-validated R varies from estimated by more than .05.
A review of several past volumes of the primary journals devoted to . MCAT scores ranged from 8 to 9, with s'Indard deviations of approximately 2. The mean nonscience (AO) GPA was 3.56; the mean science (BCPM) GPA was 3.31; both had a standard deviation less than 0.5. Mean ACT scores ranged from