Transcription
UNICEF/Bangladesh/2021/MawaAdvocacy briefACCELERATING PROGRESS TOWARDSUNIVERSAL HEALTH COVERAGE FORA HEALTHIER BANGLADESHA young girl plays outside a vaccination centre in Khagrachari HIll District, Bangladesh.Health is a fundamental human right.Good health enables children to learnand adults to earn, it helps to reducepoverty, and provides the foundationfor sustainable development.1Advancing the goal of UniversalHealth Coverage (UHC) has thepotential to transform society inBangladesh by reducing diseaseburdens, optimizing health outcomes,boosting economic growth andstrengthening accountability to allcitizens.Key factsPopulation: 165 millionUHC service coverage index:49 out of 10025 % of people affected by catastrophic healthexpenditure in 2016Over 5 million people impoverished by healthcarecosts each yearCurrent public health expenditure:0.7% of Gross Domestic Product (GDP)1
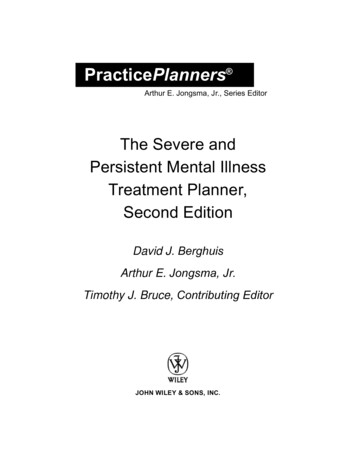
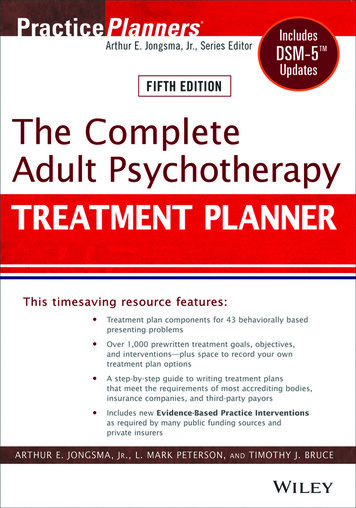
UNICEF/UN0377818/MawaIntroductionUHC means every person has access to quality healthservices when and where they need them withoutrisking financial hardship. This includes all healthservices a person may need throughout their lifetime, from health promotion to prevention, treatment,rehabilitation, and palliative care.1Achieving UHC is both a political and technical process.Each country can make progress no matter where it ison the UHC journey. Bangladesh has performed well inachieving the health-related Millennium DevelopmentGoals, by using its modest health spending efficientlyand equitably, concentrating on primary care servicesand advancing the social determinants of health.2However, as the population ages and the burden ofnon-communicable diseases increases, the healthsystem is not well placed to achieve its healthrelated Sustainable Development Goal (SDG) targets– including UHC. Furthermore, UHC is fundamentalto achieving other SDGs for example, eradicatingpoverty in all its forms and dimensions, SDG 1. TheCOVID-19 pandemic presents new challenges for thehealth system while exposing some fundamentalweaknesses.2 At the same time, COVID-19 providesopportunities to strengthen both coverage and qualityof services and reshape the health system to make itmore resilient for future pandemics.A nurse provides care to a vulnerable newborn baby at the SpecialCare Newborn Unit (SCANU) in Kurigram District Hospital.With strong political commitment, targeted policyinterventions and financial investment, Bangladesh canovercome its challenges and accelerate progress onUHC to benefit children and all citizens.Figure 1: Changes in coverage of essential health services in Member States of the South-East Asia Region,2010-2020UHC service coverage index827220102020666463626256Thailand DPR Korea Sri lankaBhutanIndia554949Indonesia Maldives Myanmar Timor-Leste Bangladesh NepalSource: World Health Organization (WHO) Crisis or Opportunity? Health Financing in Times of Uncertainty. Country profiles from theSouth-East Asia Region32
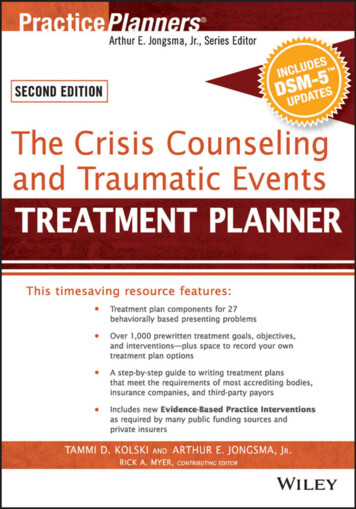
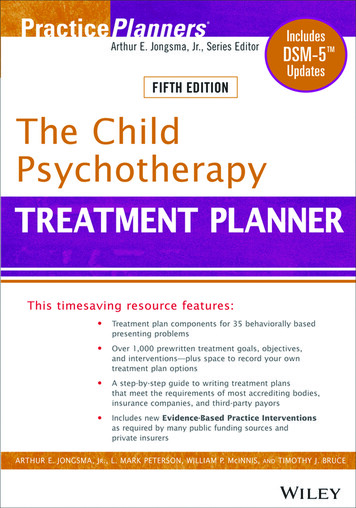
The issuesWhile the number of Primary Health Care (PHC)facilities has increased in Bangladesh, the urban PHCsystem is fragmented and uncoordinated. Privatefacilities and NGOs provide many urban health servicesincluding PHC. The overreliance on largely unregulatedprivate providers has led to a high burden of financialstress for urban residents.2Health service coverage and quality, financing andgovernance are the key components that create anenabling environment for UHC.While Bangladesh has made progress over the pastdecade, it continues to reach less than half of thepopulation with essential health services, among thelowest in the South-East Asia region. Figure 1 showsthat in 2020, Bangladesh scored 49 out of 100 on theUHC service coverage index, an increase from 38 outof 100 in 2010. However, the country still has someway to go towards achieving UHC.Access to maternal health services reveals inequitiesacross different socioeconomic groups. Only 17 percent of the poorest women had four antenatal visitscompared to 66 per cent of the wealthiest women,while 32 per cent of the poorest women delivered witha skilled birth attendant, compared to 86 per cent ofthe wealthiest women.4 This gap in access to maternalhealth services is reflected in a high maternal deathrate (196 per 100,000 live births).5Inequitable accessDespite overall improvement in health servicecoverage, inequities persist across differentgeographical locations and socio-economic groups.Figure 2 shows that between 2015 and 2019, nationalcoverage of immunization remained consistent (82-83per cent). However, coverage varied widely betweendistricts, with some districts improving as othersdisimproved during this period.Figure 2: National and district level coverage of immunization: Valid Full Vaccination Coverage by age of 12 monthsamong 12-23 Months old Children 2015-2019PANCHAGARHPANCHAGARHPANCHAGARHLALM ONIRHATTHAKURGAO NLALM ONIRHATNILPHAMA RITHAKURGAO NKURIGRAMRANGPURDINAJPURTHAKURGAO AB.BARIANARAYANGANJCOMI ANJBARISALKHULNASATKHIRANARSHINGDIM PURCHUADAN HIGANJMADARIPURSIRAJGANJNATORECOMI AZARSYLHETNETRAKON AMYMENSINGHPABNAM DAN GAMUNSHIGANJSHARIATPURNARAILJESSOREB.BARIACOMI LLASHERPURNAOGAO JGANJNATOREHABIGANJPABNAM ANIKGANJSYLHETNETRAKON GRANAWABGANJMYMENSINGHJOYPURHATSHERPURNAOGAO NNETRAKON AMALPURBOGRACHUADAN GANILPHAMA RIGAIBANDHANAOGAO M ONIRHATNILPHAMA RIGAIBANDHARAJSHAHI2019: National coverage 83.9%2016: National coverage 82.3%2015: National coverage 82.5%PATUAKHALIBARGUNABARGUNABANDARBA NBANDARBA NBANDARBA NCOX'S BAZAR (CL)COX'S BAZAR (CL)COX'S BAZAR (CL)Number of districts201520162019 75%33375-79%138380-84%27353085-89%15142090% 648Source: Government of Bangladesh (2019) Expanded Programme on Immunization (EPI) Coverage Evaluation Survey (CES) 20193
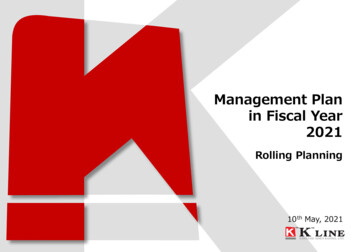
Chronic underfundingFinancial protectionWhile Bangladesh has one of the fastest growingeconomies in the world, achieving 8.2 per cent annualgrowth in Gross Domestic Product (GDP) in 2019, thecountry’s health system is chronically underfunded.6Bangladesh has three main sources of health revenue:the government budget; household out-of-pocketpayments; and external donor funds.Bangladesh has comparatively low spending on healthcare at 0.7 per cent of Gross Domestic Product (GDP)in 2019. This must be increased to at least 2 per cent ofGDP to reach the target established in the Governmentof Bangladesh’s 8th Five-Year Plan 2020-2025.7Figure 3 below highlights that Bangladesh is the onlycountry in the South-East Asia Region experiencingsome backward development on public healthexpenditure. From 2009-2018, the Government’sbudget allocation to health decreased by more than40 per cent from 5.2 per cent to 3 per cent of totalgovernment expenditures.Figure 4 shows that in 2018, the governmentbudget made up 17 per cent of the Current HealthExpenditure, external donor sources comprised 6.5 percent and out-of-pocket expenditure (OOP) accountedfor 74 per cent.3The heavy reliance on Out-Of-Pocket (OOP) paymentsto fund the health sector means that unexpectedillness can lead to severe financial stress, sometimesrequiring people to sell or borrow assets, oruse up their life savings – which can perpetuateintergenerational poverty Health share of domesticgovernment expendituresDomestic government spending on healthas share of total health expendituresFigure 3: Domestic government spending on health among South-East Asia Region Member States: its share inoverall health spending and government health expenditures, 201810%0%0%BangladeshIndiaMyanmarContinued improvementNepal Timor-Leste Bhutan Sri lanka Indonesia Thailand MaldivesFairly unchangedSome backward developmentSource: WHO (2021) Crisis or Opportunity? Health Financing in Times of Uncertainty. Country profiles from the South-East Asia Region3Figure 4: Sources of financing by country as a share of current health expenditure 2018MyanmarBangladeshIndiaNepalIndonesiaSri ent40%Social health insurance60%OOPS80%External financing100%Rest**Rest includes other domestic revenue sources than OOPS, such as corporations, non-profit entities, and voluntary prepayments, etc.Source: WHO (2021) Crisis or Opportunity? Health Financing in Times of Uncertainty. Country profiles from the South-East Asia Region34
UNICEF/UNI171904/KironNurse Shilu Majumder takes a pause during her busy day in the Cox’s Bazar District Hospital.Bangladesh has the highest catastrophic healthexpenditure rates in South Asia, with 25 per centof the population experiencing catastrophic healthexpenditure in 2016, and over 5 million peopleimpoverished by healthcare costs each year.3Figure 5 below shows the increasing numbers ofpeople pushed into poverty in Bangladesh due tohealth expenditure.Without urgent action, catastrophic health expenditureand impoverishment are expected to increase betweennow and 2030, pushing millions more into poverty.2Health system indicatorsHealth service coverage and financial protectionare strongly linked to key health system indicatorsincluding human resources, medicines, infrastructure,information technology and governance. Bangladeshis experiencing a health workforce crisis. WHOrecommends 23 health workers (doctors, midwivesand nurses) per 10,000 population as a minimumto provide the most basic coverage.8 As of 2018,there were only four nurses and five doctors per10,000 population.7 This workforce shortage impactsthe quality of care provided and pushes poorer andmarginalised populations to seek health care fromunqualified providers.2Figure 5. Catastrophic and impoverishing incidence due to out-of-pocket expenditures on health in 92016Proportion of population spending morethan 10% of their expenditures on health20092016Proportion of population being pushed under US 1.90per capita poverty line due to health expendituresSource: WHO (2021) Crisis or Opportunity? Health Financing in Times of Uncertainty. Country profiles from the South-East Asia Region35
Demographic transitionDisease burdenBangladesh is experiencing major demographic shifts.Improvements in life expectancy combined withlower fertility rates are resulting in a rapidly ageingpopulation. The speed of ageing in Bangladesh isfaster than Japan, and considered among the fastestin the world. As people age, their health needsbecome more complex, placing increased demands onthe healthcare system.The disease burden is shifting from communicablediseases towards non-communicable diseases (NCDs)such as heart disease, cancer, chronic respiratorydisease and diabetes, requiring more lengthy andcostly treatments. Figure 7 below shows that in 2016,NCDs accounted for 67 per cent of total deaths.10Despite its growing significance, the health system isprimarily geared towards addressing communicablediseases and maternal, neonatal and child health.Figure 6 below highlights the actual and projectedshapes of population pyramid of Bangladesh in 1980,2015 and 2050.There is an urgent need to address the underlyingfactors that often result in poor health – includingpoverty, nutrition, education, water and sanitation,climate change, discrimination, as well as investing inexpansion of essential health services for NCDs.2Figure 6. Population pyramids of Bangladesh1980100 95 - 9985 - 8990 - 9480 - 8475 - 7970 - 7465 - 6960 - 6455 - 5950 - 5445 - 4940 - 4435 - 3930 - 3425 - 2920 - 2415 - 1910 - 145 -90 -410502015100 95 - 9985 - 8990 - 9480 - 8475 - 7970 - 7465 - 6960 - 6455 - 5950 - 5445 - 4940 - 4435 - 3930 - 3425 - 2920 - 2415 - 1910 - 145 -90 -45101050% Male2050100 95 - 9985 - 8990 - 9480 - 8475 - 7970 - 7465 - 6960 - 6455 - 5950 - 5445 - 4940 - 4435 - 3930 - 3425 - 2920 - 2415 - 1910 - 145 -90 -451010505% FemaleSource: United Nations World Population Prospects 20199Figure 7: Proportional Mortality in Bangladesh 20162016 total population:163,000,0002016 total deaths:856,00030% Cardiovascular diseasesNCDs are estimatedto account for67% of all deaths26% Communicable, maternal, perinatal and nutritional conditions12% Cancers12% Other NCDs10% Chronic respiratory diseases7% Injuries3% DiabetesSource: WHO Noncommunicable Diseases (NCD) Bangladesh Country Profile, 201810610
Why investment in UHC matters?Way ForwardHow countries invest in health matters enormouslyfor children. UHC advances children’s right to healthand develop to their full potential. UHC also brings awide range of benefits for all society, from improvedaccess to health services and better health outcomes,to financial protection from health costs, economicgrowth, poverty reduction and the promotion ofpolitical stability.To achieve UHC, Bangladesh requires strong politicalleadership and steadfast commitment.Helping achieve children’s right to healthChildren are the most vulnerable in any population.UHC can help to advance children’s right to healthenshrined in Article 24 of the Convention on the Rightsof the Child by covering the entire population andremoving barriers to health service access. Growingevidence suggests that poor health status in infancycan predispose adults to non-communicable diseasesin later life. Investing in children’s health will bring longterm benefits to both children and society.9The road to UHC is long but progress can be made ateach step of the journey. To address the most criticalgaps and accelerate progress to achieve UHC and SDGtargets, the following are the key recommendations foraction.Key recommendations1Human capitalUHC maximizes the potential of the most criticaland strongest asset for a country, human capital. It’sa foundational investment in human capital and ineconomic growth, without good health, children areunable to go to school and adults are unable to work.2Health benefitsUHC will improve the health and well-being of allBangladeshi people, with the poorest and traditionallymarginalized populations likely to benefit the most.Everyone has the right to access affordable, equitablehealthcare. UHC boosts individual health outcomesand contributes to healthier, happier families andcommunities.113Economic benefitsInvesting in health delivers excellent economic returns.For every 10 per cent gained in life expectancy,economies can expect a boost of 0.3 to 0.4 per centin annual growth.12 By improving health and reducingthe economic cost of illness (productivity and incomelosses), UHC boosts economic and social security.Families can redirect money previously spent onhealthcare for other household needs including food,education, housing and savings.10Political benefitsUHC requires strong political leadership, commitmentand action. Championing a UHC agenda can deliversignificant political benefits as the majority of citizenswant access to affordable, quality health services.UHC builds solidarity and strengthens accountabilitybetween government and its citizens. Advancingprogress on UHC would demonstrate decisiveleadership in tackling the COVID-19 crisis and futurehealth needs.456Increase allocations to health to addresscritical shortages of skilled health workers,medical equipment and supplies from currentpublic health expenditure of 0.7 per cent ofGDP to at least 2 per cent as per the 8th FiveYear Plan. Without investment and reform,Bangladesh risks deepening existing inequalitiesthrough increased OOPs, pushing millions moreinto poverty.Provide health care services for free. Investin the expansion of quality primary health careservices and implementation of the EssentialServices Package. Increase human resourcesfor health and pay special attention to the poor,hard-to-reach populations. Leverage resourcesand learnings from the COVID-19 response.Utilize health and well-being data includingthe key components for UHC in a geographicarea, keeping in mind emerging challengeslike climate change, environmental health andCOVID-19. Use evidence-based health datato guide expansion of health services acrossgeographic areas and socio-economic groups.Review and expand social protectionschemes like Shasthyo Shurokhsha Karmasuchi(SSK) and the Maternal Health Voucher Schemeas outlined in the 8th Five-Year Plan.Expand urban primary health care servicesand reduce inequities. Investment in urbanhealth clinics will address inequities in healthcoverage and reduce out-of-pocket expenditurefor Bangladesh’s rapidly growing urbanpopulation.Bring together coalitions and createchampions for UHC in Bangladesh. Buildmomentum and create a winning situation forthe country to achieve UHC.7
Endnotes1World Health Organization, What is Universal Health Coverage? niversal-health-coverage-(uhc) Accessed 16 May 2021.2 UNICEF Policy Brief Universal Health Coverage (unpublished)3 World Health Organization (2021) Crisis or Opportunity? Health Financing in Times of Uncertainty. Country profiles from the SouthEast Asia Region https://apps.who.int/iris/handle/10665/341404 Accessed on 22 June 20214 UNICEF (2019) Bangladesh Multiple Indicator Cluster Survey (MICS) 20195 Government of Bangladesh (2016) Bangladesh Maternal Mortality and Health Care Survey 2016 Final Report. MMS-2016-Final-Report 10-Feb-2020.pdf Accessed on 2 March 20216 World Bank national accounts data, and OECD National Accounts data files. D.ZG?locations BD Accessed on 24 May 2021.7 Government of Bangladesh (2020) 8th Five-Year Plan 2020-2025. Promoting Prosperity and Fostering Inclusiveness -03-17-04-ec95e78e452a813808a483b3b22e14a1.pdf Accessed on 15 June 2021.8 World Health Organization www.who.int/workforcealliance/knowledge/en/ Accessed on 16 May 2021.9 United Nations (2019) World Population Prospects. Population Dynamics. ofiles/Pyramid/50 Accessed on 2 June 2021.10 World Health Organization (2018) Non-Communicable Diseases (NCDs) Bangladesh Country Profile www.who.int/nmh/countries/bgd en.pdf Accessed 16 May 2021.11 UNICEF (2016) Thematic paper: Accelerating progress towards universal health coverage for women and children in South Asia, EastAsia and the Pacific. www.unicef.org/rosa/media/4581/file Accessed on 16 May 2021.12 World Health Organization (2001), Investing in health: A Summary of the Findings of the Commission on Macroeconomics andHealth, WHO, Geneva. https://apps.who.int/iris/handle/10665/42435 Accessed on 16 May 2021.Published by UNICEF BangladeshUNICEF House, Plot E-30 Syed Mahbub MorshedAvenue, 1207 Dhaka, BangladeshTel: 880 (0)2 55668088E-mail: www.facebook.com/unicef.bd United Nations Children’s Fund (UNICEF)June 2021
UHC means every person has access to quality health services when and where they need them without risking financial hardship. This includes all health services a person may need throughout their life time, from health promotion to prevention, treatment, rehabilitation, and palliative care.1 Achieving UHC is both a political and technical process.