Transcription
11Proprioceptive Neuromuscular FacilitationVICKY L. SALIBA, GREGORY S. JOHNSON, and CHERYL WARDLAWmovements) cause repetitive, abnormal, andstressful usage of the articular and myofascialsystem, often precipitating structural dysfunctions and symptoms. 3,6,12,19,23,24The goal of the PNF approach is to facilitate an optimal structural and neuromuscularstate. This helps to reduce symptoms, to improve the distribution of forces through thesymptomatic region, and to reduce the inherent functional stresses caused by poor neuromuscular controJ.15,1 9 ,23,24The principles and procedures of PNF areespecially effective when integrated with appropriate use of joint and soft tissue mobilization techniques. The basic philosophy andprinciples of PNF can be universally integrated into any treatment approach, since thefoundation is the evaluation and treatment ofposture and movement. The utilization ofPNF for spinal dysfunction is enhanced by aworking knowledge of arthrokinematics, neurophysiology, and possible pathomechanics ofthe spine.Proprioceptive Neuromuscular Facilitation(PNF) is a dynamic approach to the evaluationand treatment of neuromusculoskeletal dysfunction with particular emphasis on thetrunk. Over the past couple of decades substantial progress has been made in the conservative care of spinal problems. 1- 5 The shifttowards evaluating and treating them from afunctional or neuromuscular perspective enhances and complements the symptomaticand structural approaches. 6- 14 A functional orneuromuscular approach looks beyond theclassical diagnosis, identifying their habitualpatterns of posture and movement; their dynamic strength, flexibility, and coordination;and the specific muscle recruitment andmotor control of the symptomatic region,as well as contributing factors in the patients'environment.PNF applies neurophysiological principlesof the sensory/motor system to manual evaluation and treatment of neuromuscular skeletal dysfunctions. PNF provides the therapistwith an efficient means for evaluating andtreating neuromuscular and structural dysfunctions.15-19Structural dysfunctions (myofascial and articular hyper- and hypomobilities) affect thebody's capacity to assume and perform optimal postures and motions and often are associated with symptoms.2,5,15,20-22Neuromuscular dysfunctions (inability to coordinate and efficiently perform purposefulTHE EVOLUTION OF PNFThe PNF approach was developed by Herman Kabat, MD, and Margaret Knott, PT,(Fig. 11.1), during the 1940s and early 1950s,primarily as a method to treat patients withneurological dysfunctions. 16·25,26 Dr. Kabatdesired to offer more to the neurologicallyinvolved patient population than walkersand passive range of motion exercises. He243
244Figure 11.1. Margaret Knott, PT (December 18,1978) -Devoted to her patients, dedicated to her students, and a pioneer in her profession.searched the literature to uncover basic neurophysiological principles which could serveas the foundation for a more dynamic andfunctional approach. His studies led him tothe works of Sherrington, Gellhorn, Coghill,Gesell, Hellebrandt, and others. 15·17 Theseresearchers identified that a muscle responsecould be influenced by resistance, stretch reflex, irradiation, and other proprioceptiveinput. Stimulated by his studies, Dr. Kabatsearched for clinicians whose treatment approach could serve as a foundation for theclinical application of these neurophysiological principles. His search then led him to Sister Elizabeth Kenny, who was successfullyusing manual resistance and neurophysiological principles to facilitate active functionalmovement in polio patients.Dr. Kabat, a physician who liked to physically work with his patients, began to put intoaction the knowl edge he had acquiredRATIONAL MANUAL THERAPIESthrough his research, along with the clinicalknowledge he gained from watching SisterKenny. His goal was to meet the needs of theneurological population by focusing on thereeducation of the patient's developmentalpostures and movements. He believed this approach facilitated the patient toward more efficient function and independence duringADL.16The effectiveness of PNF evolved with itsspecificity. When Margaret Knott began towork with Dr. Kabat in the mid-40s, theyfocused their attention toward utilizing theconcepts of resistance, stretch reflex, approximation, traction, and manual contact to thefacilitation of efficient motor recruitment patterns. Their goal was to facilitate efficientresponses in specific muscles and musclegroups. This commitment towards developing specificity laid the groundwork for theeffectiveness of PNF as a broadly applicablemanual therapy approach.Regardless of the underlying pathology,evaluation and treatment of structural andneuromuscular dysfunctions depend upon anassessment of specific motor recruitment andcontrol. The PNF approach offers the trainedclinician tools to quickly and effectively evaluate these motor components. It builds on theconcept that motor recruitment can be enhanced through appropriately utilized reflexand proprioceptive input. From this initialfoundation, PNF continues to evolve to newlevels of proficiency through clinical experience and scientific advances, but the initialconcepts and principles developed by Kabatand Knott have withstood the test of time.PHILOSOPHYThe philosophy of the PNF approach is basedupon the premise that all human beings haveuntapped existing potential. Therefore, the roleof the physical therapist is to identify dysfunctions and facilitate the patient's optimal physical capacity.10,15,17,27To facilitate the patient's optimal functional level and insure total involvement inthe rehabilitation program the therapist must
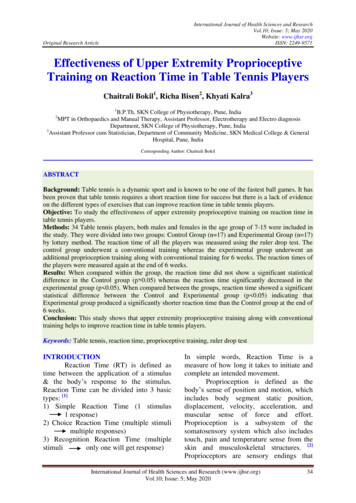
CHAPTER 11 : PROPRIOCEPTIVE NEUROMUSCULAR FACILITATIONdevelop effective rapport. An important aspect of developing rapport is to capitalize andplace emphasis upon the individual's physical,mental, and emotional strengths, rather thanhis or her deficits. A person's strengths become the foundation from which reeducationand learning take place. Working from one'sstre?gths, rather than one's deficits, tends toachieve succes , not frustration-physically,mentally, emot10nally, and spiritually.S engths are best utilized by mutuallyagreemg upon clear and attainable short- andlong-term goals. These goals should be developed both from a thorough evaluation andthe needs and desires of the patient. Basedupon stabli hed goals, the treatment program 1s specifically designed to address theidentified functional limitations. When treating neuromuscular dysfunct10ns, complex motor patterns are reduced totheir basic movement and developmentalcomp?nents. The emphasis is placed uponselective reeducation of individual motor elements, through developing the fundamentalskills of trunk control, stability, and coordinated mobility. These basic motor skills arebuilt upon by progressing to less stable postures and more complex functional activities.Each movement and posture learned is reinforced tJ:irough repetition in an appropriatelyde andmg and mtense training program.This program may consist of manual treatment, a home program, an exercise class, and?r a gym prog am. The intensity of the physical program is graded to meet the patient'sspecific strength and endurance needs for performing efficient postures and movementsduring daily activities.PRINCIPLESThe principles of PNF are based upon soundneurophysiological and kinesiological principles and clinical experience. 10 15 Each is ane sential component of the approach and provides the basis for developing consistencythroughout the evaluation and treatment process. Through applying these basic principlesthe patient's postural responses, movemen 245patterns, sn·engths, and endurance can be assessed and enhanced.Manual ContactsThe psychological effect of manual contact iswell known. 15 28 29 The comment "You arethe first one to really touch me where it hurts"is frequently made after the initial evaluationby a manual medicine or therapy practitioner.The inherent responsibility of a manual therapist is to maximize the psychological benefitby establishing trust and cooperation withoutfacilitating dependency. 1;he quality of touch influences the patients confidence and the appropriateness ofthe motor response and relaxation. Thereforesensitivity and specificity should be utilizedwhen applying a manual contact. The therapist should be consistent and specific with allmanual contacts to allow for accurate evaluation, effective treatment, and continuous reassessment.On a physical level, manual contacts to theskin and deeper receptors influence neuromuscular responses. 3o, 3i Through the use ofappropriate and specific manual contacts thetherapist can influence and enhance th direction, strength, and coordination of a motorre ponse. Ap ropriate manual contacts are applied to the skm suiface on the side to which themovement or stabilizing contraction is desired. lo, 15If inappropriate contacts are applied, the sensory input is confusing and affects the motorresponse. One testing for shoulder flexions ength to access t e effectiveness of the applied manual techniques can distort the findings if consistent manual contact is not maintained during the pre and post treatmenttesting. Use of a lumbrical grip is the mosteffective means of applying appropriate manu.al co tacts. This allows for a less compressive gnp, while still facilitating specific unidirectional contact (Fig. 11.2).Therapist Position and Body MechanicsAn essential aspect in applying appropriatema al contacts is the use of proper bodyposition and mechanics. 13 The therapist needs
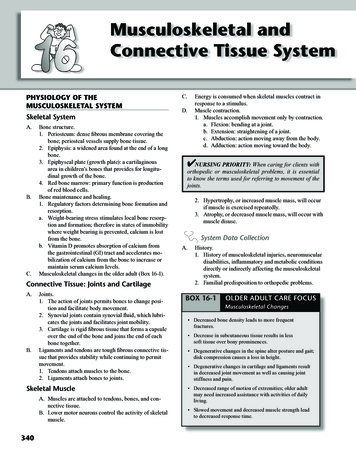
246RATIONAL MANUAL THERAPIESFigure 11.2. Appropriate manual contact- utilizing a lumbrical grip.to position his center ofgravity and base ofsupportin line with the direction ofmotion being resisted.This position allows the movement to occureither towards or away from the therapist, sothat weight transference and acceptance canbe coordinated and smooth. The therapist'stotal body and arm movement should equalthe same excursion and reflect the same arcof motion as the body part being treated. Thetherapist's spine should remain in a neutralalignment with motion occurring primarily inthe hips, legs, and arms (Fig. 11.3).Appropriate manual contacts and body position provide resistance from the therapist'strunk rather than the upper extremities.Therefore, the arms can relax and bettertranslate the resistance and evaluate the motorresponse. The slightest deviation from the useof appropriate position and body mechanicscan alter the desired response and distort thetherapist evaluation.lO,ll,ISAppropriate ResistanceAppropriate resistance 10 is the amount of resistance which facilitates the desired motorresponse through a smooth, coordinated, andoptimal muscle contraction. 15 Appropriateand variable resistance is applied to an activecontraction for two purposes. Initially, the resistance allows the therapistto evaluate the patient's motor response.Characteristics such as control, strength,initiation, stabilization, endurance, relaxation, and quality of contraction are effectively assessed when manual resistance is applied to the patient's contraction.10,IS,19 If a dysfunction is identified in any of thesecharacteristics, appropriate resistance applied in conjunction with various PNF techniques, facilitates the relearning and rehabilitation process. 10 15 18During normal activity the neuromuscularsystem utilizes a variety of muscle contractions to meet the normal demands of efficientmotor control.32 The patient's capacity to stabilize (isometric), as well as move (isotonic),can be specifically evaluated through manualresistance. The use of resistance allows thetherapist to determine the patient's ability toselectively and efficiently perform and integrate each of these contractions. Identifieddysfunctions are specifically treated to facilitate optimal function.The kinesiological definitions of isometricand isotonic contractions vary within the lit-
247CHAPTER 11 : PROPRIOCEPTIVE NEUROMUSCULAR FACILITATIONFigure 11 .3. Proper therapist body position and body mechanicspromotes smooth and coordinated movements.erature. We have chosen to define these termsto correspond with "functional evaluation andtreatment" represented by the approach ofPNF.Isometric Contractions. The traditionaldefinition of an isometric contraction is onein which "the external force is equal to theinternal force developed by the muscle andno external movement occurs." 32 33 The functional definition of PNF builds on this definition to include the intention of the contractions . According to the authors, thiscontraction is a stabilizing contraction "inwhich the patient's intention is to maintain aconsistent position in space." 10Isotonic Contractions. The traditionaldefinition of an isotonic contraction is, "acontraction in which the external force is constant and motion occurs." 32 33 An isotoniccontraction as defined in the PNF approachis one "in which the patient's intention is tocreate movement." 10These are subdivided into concentric (a dynamic shortening of the muscle), eccentric (adynamic controlled lengthening), and maintained contractions. A maintained contractionis a dynamic contraction in which the patient'sintention to produce movement is limited bya greater external force. This contraction differs from an isometric contraction in that theintention of an isometric contraction is tomaintain a stabile position. 10An example of the interaction of these variouscontractions occurs during the removal of abowl from a high shelf. When reaching, thearm must concentrically raise, perform a maintained contraction to stabilize the weight of thebowl as it leaves the shelf, and eccentricallylower the bowl and arm to the counter. Duringthis motion components of the trunk performisometric contractions to maintain a stable position in space.Each of these functional types of contractions needs to be specifically evaluated andfacilitated. Nonvarying mechanical resistancecannot create the variables needed to stimulate these differentiated contractions. ThePNF principle of manually applied appropriate resistance allows for this selective differentiation to occur. The therapist varies thetype and degree of resistance to facilitate theappropriate response. The resistance mustvary in application, power, and endurance toevaluate and treat the patient's dysfunctions
248of selective motor control, coordination,range of motion, strength, initiation, stabilization, and/or relaxation.Irradiation. Resistance can also be usedto produce appropriate irradiation. 10 Irradiation is defined as the overflow of excitationfrom stronger components to weaker or inhibited components. 15 ·34,35,36 This is accomplished through the application of graded resistance to stronger components to facilitateirradiation and produce an appropriate andenhanced contraction in weaker ones.There are many variables which the therapist must consider while utilizing appropriateresistance to facilitate an efficient motor response such as: the patient's position, gravity,existing normal and abnormal reflexes, therapist's manual contacts, and body mechanics.The encouragement of controlled breathingfurther reinforces efficient movement.RATIONAL MANUAL THERAPIESing the desired motor response. 15· 36 They supply a reflex enhancement to the volitional response to resistance. Therefore, the therapistmust be aware of blending traction or approximation with resistance to ensure smooth andappropriate resistance (Fig. 11.4).Traction. This is the elongation of a segment and separation of joint surfaces whichfacilitates an enhanced muscular response topromote movement or enhance stability.10,15The direction of traction is always appliedaway from the apex of the arc of motion (Fig.11.4).Example. Use of general traction when n·eating a patient with an acute cervical spine canassist the patient in his/her abil ity to performcontrolled contractions without pain. The PNFapproach utilizes traction differently than distraction which is designed to specifically separate joint surfaces. 20Example. Various forms of resistance can beapplied to the shoulder girdle as an effectivetreatment of cervical dysfunction. In cases of acute pain, gentle, slowly builtisometrics can often decrease tone, mobilizearticulations, improve circulation, and decrease pain through indirect means. In many individuals with cervical dysfunction , abnormalities in neuromuscular control of shoulder girdle motions are identified. This alteration of neuromuscularcontrol is effectively treated using the various forms of isotonic contractions combinedwith isometric contractions. The isometriccontraction allows the therapist to monitorthe slowly building conn·action to assureproper muscle recruiunent, followed by theretraining of the isolated group with variousisotonic contractions. In these cases appropriate resistance is utilized in conjunctionwith the appropriate technique for trainingcontrol. In patients where more trwik or neck facilitation is desired maximal resistance is givento the shoulder girdle to facilitate appropriate irradiation.Traction and ApproximationTraction and approximation utilize forcevectors to assist the resistance and in facilitat-Figure 11.4. The force vectors of resistance and traction or approximation-combine to provide appropriate resistance and facilitation.
CHAPTER 11 : PROPRIOCEPTIVE NEUROMUSCULAR FACILITATIONApproximation. A compression force towards the axis of motion resulting in an approximation of joint surfaces is Approximation. It facilitates an increased muscularresponse and promotes stability, and is oftenused when facilitating stability in weight bearing postures or positions. 15 19 37, 3s The desiredresponse can be initiated or reinforced by areflex- producing quick approximation, followed immediately by a maintained approximation and resistance.Example. Use of approximation can be usedto retrain postural awareness in sitting by facilitating a more stable and improved responseof the trunk musculature and improve trunkstability (Fig. 11.5).249less coupled with a volitional contraction andappropriate resistance.Cautions. When applying traction or approximation care must be taken to avoid increasing pain, and consideration must begiven to the underlying pathology. In manycases where the joint is the source of pain,such as arthritis, judicious use of traction orapproximation may decrease symptoms andallow for a more intensive rehabilitation program. Pain which is secondary to articularinstability may be reduced with a combinationof resistance and traction or approximation,allowing for greater facilitation of neuromuscular stabilization.Quick StretchEven though reflex responses can be facilitated through use of traction and approximation, these responses are not therapeutic un-Figure 11.5. Use of approximation- to reinforce stab ility and reeducation.In the presence of weakness, incoordination,poor initiation, or poor endurance a volitionalcontraction can be heightened and reinforcedthrough the use of spinal reflexes. PNF usesa facilitating cue termed quick stretch to offera stretch stimulus and produce a desiredstretch reflex. 15 18Gelhorn defined stretch stimulus as the"increased state of responsiveness to corticalstimulation that exists when a muscle is placedin an elongated position."39 The stretch reflexis a spinal reflex that is facilitated by a quickelongation of a muscle on stretch. T his stretchstimulates the extrafusal and intrafusal musclespindles fibers to fire and produce a reflexcontraction. 18 40 This reflex response, if isolated, produces a quick, short-lived contraction. However, if resistance is applied immediately to the contraction in conjunctionwith an appropriate verbal command, the result is a facilitated muscular response.The use of these neurophysiological principles, such as the stretch reflex, allows thetherapist to facilitate the initiation, force, direction, or endurance of a specific motor response through quick stretch. While theseprinci pies can affect the response of individualmuscles, the tool is most effective when applied to a synergistic group of muscles or aPNF pattern of facilitation. Quick stretch canbe applied at the beginning of a contraction
250when the muscle group is lengthened orthroughout an active contraction. When utilized throughout an active contraction, thestretch reflex is facilitated from existing tension within the contracting muscle. A contraindication to the application of quick stretchis increased pain. ISExample. Consider the posterior elevation pelvic pattern which is functionally utilized in stepping backwards and scooting. To perform thispattern the latissimus dorsi, erector spinae, andquadratus lumborum must function together toachieve an efficient movement. If the patienthas difficulty in initiating the contraction, justplacing the muscles on stretch often will facilitate a stronger more effective pattern. If thatis not sufficient, a stretch reflex can be appliedto initiate the contraction and repeated eitherat the beginning or through the range.RATIONAL MANUAL THERAPIESheightened or easily aroused neuromuscular responses.Summary. Verbal commands are used to: coordinate volitional effort with reflex response, define the type of muscular contraction, define the direction of motion, signal timing of relaxation of contraction, facilitate increased involvement and arousal, stimulate generalized relaxation.Visual StimuliThe visual system is important in normal development and coordinated use of the body(Fig. 11.6). The therapeutic utilization of visual stimuli goes beyond the use of vision toteach an activity. Developmentally, the neuromuscular system gains its control in a ce-Verbal StimuliThe therapist's verbal command is a primarylink between reflex responses and the patient'svolitional response. 15 Without the use of verbal commands, there is no cognitive reeducation taking place, only reflex responses to proprioceptive input. This is a primary functionalconsideration with all patients because a reflexresponse must become volitional to facilitatethe patient's independence in motion activities.Verbal commands, coupled with manualcontacts, provide the therapist with the primary tools for establishing communicationand cooperation. Verbal commands should besimple, concise, and unidirectional. In addition, the quality of the verbal commandshould vary depending upon the type of motorresponse desired from the patient.15Example. In a sports rehabilitation setting,when a patient is stable with minimally irritablesymptoms, the goal of treatment is a heightenedmotor response and strength. The therapist'senergetic and enthusiastic verbal commandscan facilitate the patient's excitement and participation in the treatment. However, with apatient who has acute, highly irritable cervicaldysfunction, the commands are most effectivewhen given in a quiet and assuring manner.This is to promote relaxation and to not triggerFigure 11.6. Visual stimuli-reinforces the otherprinciples of facilitation and enhances the patient'sresponse.
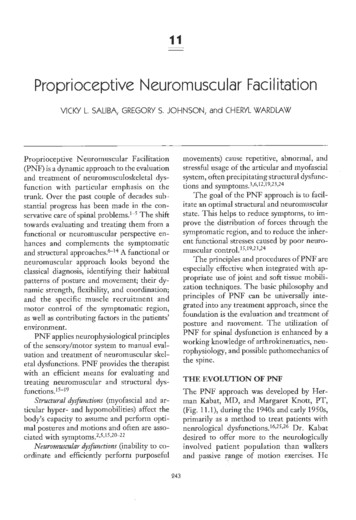
CHAPTER 11 : PROPRIOCEPTIVE NEUROMUSCULAR FACILITATIONphalic-caudal direction. Movement of thetrunk and extremities can be facilitated by theincorporation of the visual system, which requires integration of the head and neck. Failure to evaluate and include the visual systemin a rehabilitation program can inhibit or retard the development of complete and coordinated trunk and extremity control. In addition, balance and equilibrium responses relyheavily on visual input for accurate interpretation of spatial relationships.15,30,41,42Patterns of FacilitationThe patterns of facilitation were discoveredby Kabat in the final stages of his developmentof PNF.15,27 Through the utilization of all thepreviously identified principles, he began tounderstand and recognize the inherent movement patterns which humans utilize to perform normal functional and athletic activities.H e observed that normal coordinated activities are accomplished by the moving of theextremities and tnmk in diagonal and spiralmotions in relationship to each other. He observed that muscular responses were strongand coordinated when resisted within specificdiagonal patterns. In addition, the use of reflex facilitation, such as the stretch reflex, wasmost effective when the part was elongated inits specific diagonal. T his observation madeKabat question the validity of using cardinalplane motions in the rehabilitation of functional activities, because normal motion isperformed in diagonal and spiral patterns.Through trial and error, Kabat and Knottdeveloped the specific trunk and extremitypatterns.Patterns of facilitation provide the therapist with tools to evaluate and treat dysfunctions of neuromuscular control and mobilityof selective spinal articulations, as well as theability to integrate synergistic muscle groupswithin the patterns. As control is developed,synergistic muscle activity is integrated intofunctional whole body movements. Throughuse of patterns of facilitation, the patient isprovided the opportunity to correctly performand learn the desired motor response and in-251tegrate that response into daily functional activities.The patterns exist in narrow diagonals inrelationship to tl1e central axis of motion ofthe extremity and trunk. Each pattern is aswide as the part being treated and moveswithin a smooth arc of motion. T hree componen ts of motion are blended within eachdiagonal movement pattern.In the Trunk. The components ar e:flexion/extension, lateral movement, and rotation (Figs. 11. 7A,B,C).In the Extremities. The components are:flexion/extension, abduction/adduction, androtation (Figs. l l. 8A,B).Parameters. Each pattern can be identified by the following parameters.10,23,24l. When in the elongated position all synergistic muscles are equally on stretch. In thismanner the patient's functional range canbe evaluated.2. The stretch r eflex is optimally facilitatedwithin a synergistic group of muscles at onetime.3. Clinically, it can be shown that a musclecontraction is stronger when performedwithin a facilitation pattern than outside ofthe pattern. It is theorized that muscles worktogether more efficiently when placedwithin these patterns and the contraction ismore readily enhanced by irradiation. Anexample is the function of thumb and littlefinger opposition, which is easily demonstrated to be not only stronger, but moreeasily recruited when the upper exn·emity isplaced within the extension-abduction pattern.4. Resistance to an extremity pattern will facilitate a contraction within the relatedtrunk patterns.5. Increased tone and cl onus are generally reduced when the part is specifically placedwithin a component of the diagonal. This isoften dramatically illustrated in a patientwith increased abnormal tone of the upperextremity or an immediate reduction in tonewhen the scapula of that same extremity isplaced into posterior depression. 10By using the PNF patterns of facilitation,the therapist can more quickly and effectively
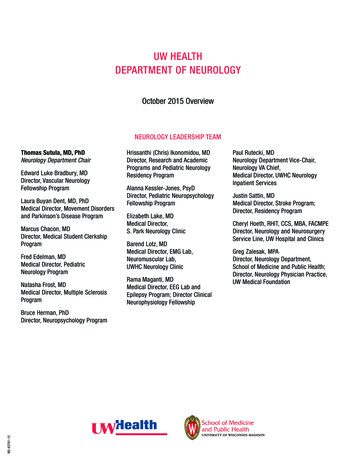
252RATIONAL MANUAL THERAPIESFigure 11 . 7. Available trunk patterns include: A) lower trunk flexion; 8) upper trunk flexionwith chopping; C) lower trunk lateral flexion with rotation.
253CHAPTER 11 : PROPRIOCEPTIVE NEUROMUSCULAR FACILITATIONAFigure 11.8. Extremity patterns include: A) lower extremity flexion/adduction/internal rotation,B) upper extremity flexion/adduction/internal rotation.evaluate neuromuscular control and range ofmotion within synergistic muscle groups.When dysfunctions are identified, specificPNF techniques are applied to enhance thedesired movement.Example. The lower trunk extensor patterncan be utilized to selectively evaluate for hypoand hypermobilities of the spine, and then treatthe identified dysfunction through specifictreatment procedures described later m thechapter.TimingNormal timing refers to the efficient sequencingof dynamic muscle contractions to achieve adesired functional result. 10 15 43 This includesthe sequence in which the muscle fires andthe controlled interaction between mobility
254RATIONAL MANUAL THERAPIESand stability of the selected components of amovement. In the orthopedic and sports injured population there is often a deficit innormal timing of motions during the performance of a pattern within symptomatic regions. These deficits are identified throughmanual and observational assessment.Example. Orthopedic patients frequentl ydemonstrate an inability to brace, or to stabilizethe lumbar spine during normal or stressfulactivities.2 1 44 The contraction of the trunkmuscles should occur reflexively in response toany external demand which could potentiallystress the spinal structures. Often the trunkmuscles will test strong with conventional muscle testing, but when tested within a mass movement pattern or during a functional activity(such as push/pull activities) the contractionwill be delayed or nonexistent. Through appropriate use of reeducation techniques abnormaltiming can be improved and integrated intonormal functional activities. (See Fig. 11. 9)Appropriate Techniques. Treatment ofdysfunctions of normal timing can occurthrough multiple avenues. Reduce the motion or activity to the simplest components and facilitate an optimalcontraction of each individual component.Then combine these individual componentstogether into the desired functional motionor activi ty. Appropriate use of resistance, quick stretch,and verbal command are used to reinforcenormal timing. If abnormal timing is evaluated in a complexskill such as walking, less complex motionssuch as rolling and crawling can be usedinitially to train timing and kinestheticawareness.Example. One of the most valuable activities to observe for the assessment of a patient's inherent patterns of motions is rolling.To roll efficiently al
manual therapy approach. Regardless of the underlying pathology, evaluation and treatment of structural and neuromuscular dysfunctions depend upon an assessment of specific motor recruitment and control. The PNF approach offers the trained clinician tools to quickly and effect