Transcription
The Implementation ofExternal Reference Pricingwithin and across CountryBordersPanos KanavosAnna-Maria FontrierJennifer GillDionysis Kyriopoulos
The Implementation of External Reference Pricing within and across Country Borders2London School of EconomicsHoughton StreetLondonEnglandWC2A 2AEweb: www.lse.ac.ukFirst published 2017Copyright Panos Kanavos, Anna-Maria Fontrier, Jennifer Gill, Dionysis Kyriopoulos 2017DOI: https://doi.org/10.21953/lse.y1tbizsxrl3nLONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders3CONTENTSList of Figures4List of Tables4List of lusionExecutive summary781.Introduction92.Methods102.1Study endpoints102.4Primary Data CollectionResults11133.1Results of the literature review133.4Is ERP the main pricing policy or a supportive 3.97Systematic Literature Review: Data sources, search strategy and keywordsStudy selection, data extraction, evaluation and synthesisObjective of ERP and alignment with health system objectivesCharacteristics of products subject to ERP price regulationTransparency of ERP pricing policyCompetent authorities responsible for ERP implementationAppeals by stakeholders to regulator decisionsNumber of basket countriesFrequency of price revisionsCriteria for basket country selection3.10 Type of comparator price used in ERP3.11 Methods for calculation of the reference price3.12 Sources of information for pricing decisions3.13 Inclusion of wealth adjustments in ERP calculations111314161618181819222222233.14 Accounting for exchange rate fluctuations233.17 ERP alignment with other negotiation tools of reimbursement253.15 Link between price and reimbursement3.16 Interaction of ERP with HTA and VBP4.1124253.18 Link between ERP regulation and patent statusDiscussion & Policy Implications284.1304.2Policy implications4.1.1 Objectives and scope of external price referencing system4.1.2 Administration and operations4.1.3 Methods for the conduct of external price referencing4.1.4 Implementation of external price referencingCountry Adherence to 14 Best Practice Principles253131323333LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders45.Conclusion356.References36Appendix 142List of FiguresFigure 1: PRISMA flow diagram with search results from the systematic literature review13Table 1: Definition of endpoints in ERP implementation10Table 4: Main role of ERP16List of TablesTable 2: Results of systematic literature search by sourceTable 3: Type of pharmaceuticals subject to ERP across countriesTable 5: Transparency in ERP across countriesTable 6: Competent authorities in ERP implementation across countriesTable 7: Presence of appeals process for stakeholdersTable 8: Overview of basket across countriesTable 9: Number of reference countries of basket across other non-EU countriesTable 10: Frequency of price revisions across the studied countriesTable 11: Criteria for basket selection across studied countriesTable 12: Price selection across countriesTable 13: Method for calculation of reference price across countriesTable 14: Sources of information across countriesTable 15: Inclusion of wealth adjustments in ERP calculationTable 16: Methods for dealing with exchange rate fluctuationsTable 17: ERP relationship with other pricing and reimbursement policiesTable 18: Adherence to the 14 best practice principles14151717181920202121222324242634LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders5List of AcronymsAUTAustriaLTUBusiness Monitoring LISLISRITABulgariaCyprusCzech RepublicGermanyDenmarkEuropean Federation of PharmaceuticalIndustries and AssociationsExternal Reference PricingSpainEstoniaEuropean UnionFinlandLUXLuxemburgMLTMaltaLVACentre for Reviews and DisseminationLithuaniaNLDLatviaMoldovaThe BSVKOrganisation for Economic Cooperation andDevelopmentPurchasing Power ParityPortugalResearch and veniaGreeceSWESwedenHealth in TransitionTURTurkeyCroatiaVBPValue Based PricingHealth Technology AssessmentVEDVital & Essential DrugsHungaryWHOWorld Health OrganizationIrelandWHO-CCWorld Health Organisation CollaboratingCentresIsraelWoSWeb of ScienceIcelandItalyLONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders6ACKNOWLEDGEMENTSWe would like to thank Mackenzie Mills, Erica Visintin,Olina Efythimiadou and David Taylor for their insightand support throughout the development of thepaper. Finally, we thank Pfizer Ltd. for providingthe sponsorship that allowed us to carry out thisresearch.LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders7ABSTRACTBACKGROUNDRESULTSExternal reference pricing (ERP), a frequentlyimplemented pricing policy, seeks to rationalizeprices and contain costs by using foreign pricesas reference for the determination of domesticprices and facilitation of negotiation. Its use acrosscountries varies significantly in terms of objectives,methods, administration and implementation.The systematic literature review confirmed thatthere is heterogeneity in the way that ERP isimplemented across countries. There tends to bevariation in the size of the country baskets, withlarger baskets becoming more common and in theway that countries chose their basket countries– some choose those with similar socioeconomiccharacteristics whilst others do not. Furthermorethere is variation in the calculation used with mostcountries vying away from the average-basedcalculations towards the lowest basket price or theaverage of the lowest ‘n’ prices. The frequency ofprice revisions differs according to authorities andgovernment negotiations, as does the rate at whichexchange rate fluctuations are taken into account inpricing decisions. In terms of the 14 best practiceprinciples Belgium, France, and South Africa adheredto the most principles whilst Bulgaria, Hungary andRomania had the most instances of non-adherence.METHODA systematic literature review was conductedaccording to CRD guidelines. 17 Study endpointswere used to identify characteristics of ERPimplementation across 29 countries, of which 17were EU member states. Multiple databases wereexamined to provide a wide range of ERP sources.After filtering for mention of ERP implementationrelated to at least one of the 17 study endpoints 176studies remained. Primary data collection, in theform of questionnaires directed at key stakeholders,were also used to supplement data in instanceswhere information received from the systematicliterature review was outdated or minimal. Findingsfrom the systematic literature review and primaryevidence from key stakeholders were benchmarkedagainst 14 best practice principles inherent to anoptimal ERP system to determine the quality of ERPsystems implemented by the countries of interest.CONCLUSIONHeterogeneity and recent trends in ERP design havepolicy implications for governments, which includeglobally declining pharmaceutical prices and other,potentially more undesirable consequences such aslaunch delays in low-income countries, parallel tradereducing drug stock levels, inflated prices in lowincome countries, reduced incentive for continuedR&D and reduced access to medicines in someregions. Overcoming this issue to ensure that ERPis beneficial to all stakeholders will require a focuson developing sustainable, transparent, simple andstable systems using a set of key guidelines thatshould maximise the benefits of the pricing policy.LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders8EXECUTIVE SUMMARYThis paper aimed to highlight differences in theway that 29 countries implement ERP, which aimsto contain medicine costs, using a systematicliterature review-based process combined withprimary evidence from key stakeholders. Of the29 countries analyzed 17 were European MemberStates, with the remainder representative of LatinAmerica, South East Asia, the Middle East and NorthAfrica. Secondary data was collected from literaturepublished between 2000 and 2015 on a set of 17criteria (endpoints) based on the ERP system design.Databases examined included Web of Science (WoS),CINAHL, EconLit, Medline, ProQuest, CochraneLibrary and Scopus. Special keywords and a definedsearch strategy were used to arrive at an initiallist of studies. After filtering for mention of ERPimplementation related to at least one of the 17 studyendpoints 176 studies remained. Primary evidencewas collected via questionnaires distributed amongkey stakeholders. Results of the systematic literaturereview and of the primary evidence collection werecontrasted with analysis of the goals and observedimpacts of the different ERP systems to identifyoptimal design features of ERP systems.Findings confirmed high levels of heterogeneitybetween the ERP systems of different countries.Variation was present in many of the 17 endpointsanalyzed. For example, some countries use ERPfor all medicines, regardless of their patent status,whilst others use it only for in-patent medicines. ERPprocesses range from formal to informal and fromthe main to the supportive pricing policy in place in acountry. In cases where the process is informal thereis limited definition of policy objective and scopewhich can affect transparency. Country baskets rangein size from three to 36 (not including those countriesthat use prices in the medicine country of origin)whilst very few countries use any kind of wealthadjustment, even if countries are not selected basedon financial characteristics. Reference calculationstend to be based on a lowest price in the basket stylecalculation, rather than an average based calculation.Some countries use ex-factory prices, which do notreflect confidential discounts or rebates, to form thebasis of their calculations meaning referenced pricesdo not reflect reality.Rapidly evolving healthcare costs and increases inlife expectancy and chronic disease prevalence meanthat reduced drug prices are the ultimate aim for mostcountry governments. However, badly designed ERPsystems can be detrimental to all stakeholders andshould be avoided at all costs. ERP systems shouldbe designed with both health and industrial policyaims in mind to ensure that the requirements of allstakeholders including patients, manufacturers andgovernments are represented in order to ensure thatpatients get access to well-priced medicines as andwhen required, governments can spend within theirmeans and manufacturers have enough incentive tocontinue investing in future R&D in order to benefitfuture patient populations.There are a number of key criteria that can be adheredto that may ensure an ERP system is designed tobenefit all stakeholders and remains transparent,simple, stable and sustainable. These criteria arebased on the selection of reference countries andprices; the use of exchange rates; the types of productsfor which ERP should be used; price revisions; andthe derivation of target prices. Furthermore, as notwo countries are identical any EPR system shouldoutline the objective and scope of the ERP systemand ensure it reflects the overall healthcare system’svalues and objectives. It is also recommended thattarget prices should align with the expected value ofthe product, determined by using HTA or a similarmechanism. Encouraging countries to follow suchguidelines could ensure that ERP systems do notalienate the innovative pharmaceutical companyand ensure that they are incentivized to continueinvesting in global R&D which in the long run willmaximize global population health. In this paper, 14basic principles that an optimal ERP system shouldfollow were benchmarked against the findingsfrom the systematic literature review and primaryevidence from key stakeholders to determine thequality of ERP systems implemented by the countriesof interest. Belgium, France, and South Africa adheredto the most principles whilst Bulgaria, Hungary andRomania had the most instances of non-adherence.LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders91. INTRODUCTIONERP, also known as external price referencing orinternational price comparison/ benchmarking, is awidely used pricing policy with high global researchinterest. It is introduced when governments decideto use foreign drug prices to regulate domestic prices(EFPIA, 2014; Danzon and Towse, 2003) and toimpose price caps based on prices of similar drugs inother reference countries (Houy and Jelovac, 2014)with the official definition being: “the practice ofusing drug prices in several countries to derive abenchmark or reference price for the purposes ofsetting or negotiating prices in countries” (WHO,2013; EFPIA, 2014). The primary aim of the pricingmechanism is to control in-patent drug prices(Ruggeri and Nolte, 2013) via the containment ofpharmaceutical prices and expenditure (Espin etal., 2010). The widespread use of ERP generallyarises due to government cost control requirements.Authorities can use international comparisons toevaluate the fairness or appropriateness of the actualprice related to comparative cases (OECD, 2008).Specifically, drug prices in other countries are usedas a reference to determine a limit for the entry priceof a drug or reimbursement price (Nguyen et al.,2015).The implementation of ERP varies significantlybetween countries in terms of the various rulesfollowed by individual countries to calculate thefinal product price (Espin et al., 2014). For example,an increase in the number of reference countriesin a basket generally leads to further reductions indrug prices (BMI Research, 2010). Furthermore,the countries used in the basket can affect pricevariation. Financial performance of the country,pharmaceutical pricing systems, publication ofactual versus negotiated or concealed prices, exactcomparator products and disease burden of thepotential reference country all need to be taken intoaccount when choosing reference countries (WHO,2015).Although ERP may have the potential to contributeto improved access and counteract affordabilityproblems sometimes seen in lower-incomecountries, there are potential consequences. Themost significant concern is related to the fact thatERP could lead high-income countries to demandlow prices creating resulting difficulties for lowincome countries. ERP-related price leakages cantrigger a manufacturer to set either a single price ornarrow band of prices before launch is allowed. Suchlinking of low and high income markets can lead toprices converging at a higher level than would havebeen the case if markets had been separate. In lowincome countries, this can lead to inappropriatelyhigh prices and reduced access for patients. In highincome countries, whilst in the short run importedlower prices may be beneficial, in the long run,lower revenues can lead to reduced return on R&Dinvestment and consequently fewer new medicines(Danzon and Towse, 2003). Furthermore, marketingauthorization holders may prefer initially to promotetheir products to high-price countries rather thanlow-price countries so that these high prices areused as references in countries performing ERP(Vogler et al., 2015). At the same time, the accuracyof international comparisons may be distorted dueto methodological issues and differences acrosscountries in strength, formulation and pack sizesavailable (Timur and Picone, 2010). ERP assessmentis considered complex compared to other pricingmethods. The promotion of transparency aroundthe use of ERP may improve the accountability ofdecision-making, which could reduce uncertaintyfor manufacturers and eliminate discrimination andcorruption (Espin et al., 2014).There is a need to study the implementation ofERP with a focus on differences in implementationacross countries. The present study will attempt, viaa combination of primary and secondary evidence,to contribute to the review, analysis and body ofinformation about ERP structure and its alignmentwith other policies across countries where thefollowing countries are of interest: Austria, Belgium,Bulgaria, Czech Republic, Estonia, France, Germany,Greece, Hungary, Italy, Latvia, Poland, Portugal,Romania, Russia, Slovakia, Slovenia, Spain, Turkey,Brazil, Egypt, Jordan, Kuwait, Lebanon, Qatar, SaudiArabia, South Africa, South Korea and United ArabEmirates. To determine the quality of ERP systemsimplemented by the countries of interest webenchmark findings from the systematic literaturereview and primary evidence from key stakeholdersagainst 14 basic principles that an optimal ERPsystem should follow (Sullivan et al., 2017).LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders102. METHODSBoth primary and secondary evidence have been usedto identify characteristics of ERP implementationacross 29 countries and to inform the discussionand analysis in the sections that follow. Secondaryevidence was collected via a systematic literaturereview, which was carried out based on the CRDguidelines for systematic reviews.2.1 STUDY ENDPOINTSA number of defined endpoints relating to thestructural elements of ERP were analysed in thissystematic literature review (see Table 1). The mainrole of ERP in each country of interest was analysedin order to determine differences in applicationacross countries. Transparency was evaluated toexamine fairness in pricing. We also investigated therole of stakeholders in the design of ERP systemsand their involvement in any appeals processes.The number of basket countries and the criteriaused for their selection was also analysed alongsidethe methods used for price calculation. The roleof the patent status and innovation was taken intoaccount. Furthermore, investigation around theinclusion of wealth adjustments, price revisionsand exchange rate fluctuations was necessary giventheir impact on price determination (Toumi et al.,2014). The sources, dissemination and accessibilityof price data were also assessed as key issues inprice setting. As far as interaction with other policiesis concerned, the alignment of the pricing processwith the reimbursement process was examined andthe combination of ERP with different negotiationtools for reimbursement was used as an endpoint.The interaction of other pricing processes such asvalue based pricing (VBP) and health technologyassessment (HTA) with ERP was also examined.Table 1: Definition of endpoints in ERP implementationEndpointsDefinitionObjective and alignment with health systemobjectivesAssesses the aim of international comparisons and the relationship with healthsystems’ objectivesMain roleDetermine whether ERP provides the major or supportive role in negotiations anddetermination of drug pricesCharacteristics of pharmaceuticals subject toERPTransparencyCompetent authorities in ERP implementationStructural ElementsTakes into account the categories of drugs included in the ERP systemIncludes the legislative criteria used by countries to promote a fair pricing processPresents the authorities in control of ERP policy implementationAppeals by stakeholders to regulator decisions Assesses the possible appeals of stakeholders in pricing processNumber of basket countries and countries inthe basketCriteria for basket country selectionType of comparator priceMethod for calculation of the reference priceSources of information for pricing decisionsInclusion of wealth adjustmentsAccounting for exchange rate fluctuationsLink between price and reimbursementInteraction with HTA or VBPAlignment with other negotiation tools ofreimbursementLink between ERP regulation and patent statusPresents the countries and the number of members included in each basketAssesses the appropriate criteria to select reference countriesPresents the selection of price category across countriesExamines the different methods of countries to determine reference pricePresents the sources and stakeholders that contribute to public access of price dataAssesses whether wealth adjustments made to the reference price when countriesof higher or lower GDP are included in the basketAssesses whether calculations used to account for exchange rate fluctuationsacross countriesInteraction with other policiesRefers to the countries that take into account price determination andreimbursement process at the same timeAssesses the parallel use of international comparisons with other methods to setdrug pricesRefers to the combination of international comparisons with reimbursementpurposesTakes into consideration the role of patent status in ERP price calculationLONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Borders112.2 SYSTEMATIC LITERATUREREVIEW: DATA SOURCES, SEARCHSTRATEGY AND KEYWORDS2.3 STUDY SELECTION, DATAEXTRACTION, EVALUATION ANDSYNTHESISBoth peer-reviewed and grey literature wereexamined to minimize bias and identify all relevantinformation. Multiple databases were utilised, thesewere the Web of Science (WoS), CINAHL, EconLit,Medline, ProQuest, Cochrane Library and Scopus. Acombination of broad and policy key words were usedto ensure that all relevant literature was captured. Allsynonyms and different phrasings of ERP or ExternalPrice Referencing were included in the search. Thesearch run was (“Pharmaceutical Price Regulation” OR“Pharmaceutical Regulation” OR “Cost Containment”OR “Pharmaceutical Pricing” OR “External PriceReferencing” OR “External Price Referencing” OR“International Price Comparisons” OR “InternationalReference Pricing” OR “International PriceReferencing”) AND (drug OR drugs OR medicine ORmedicines OR pharmaceutical OR pharmaceuticals).The search was restricted to keywords present withinabstracts only, to limit the number of irrelevantpapers being returned. When searching the WoS,the search terms were restricted to title only, as theoption to restrict to abstract was not available. Thisstudy includes only papers in English. There were norestrictions in terms of country in the initial searchto ensure that evidence is representative of a widegeographical range. However, once the search wasconcluded, the study was limited to the followingcountries: Austria, Belgium, Bulgaria, Czech Republic,Estonia, France, Germany, Greece, Hungary, Italy,Latvia, Poland, Portugal, Romania, Russia, Slovakia,Slovenia, Spain, Turkey, Brazil, Egypt, Jordan, Kuwait,Lebanon, Qatar, Saudi Arabia, South Africa, SouthKorea and United Arab Emirates. Our study includedliterature published from 2000 to 2016.The results were filtered according to title andabstract relevance to the topic. Papers with relevanttitles were downloaded for further examination. Inorder to arrive at a final set of studies, the main bodyof these texts was assessed according to the followingcriterion: mention of ERP implementation relating toat least one of the selected endpoints. The numberof studies based on evidence at each endpoint wasnoted with cases where some papers related tomultiple endpoints, and were therefore referencedmultiple times, being taken into account.We also completed a targeted and comprehensivesearch of the WHO, the WHO collaborating Centre forPharmaceutical Pricing and Reimbursement policiesand the OECD online databases to ensure that novaluable reports were excluded. The key words usedto search these were “External Price Referencing”OR “External Price Referencing” OR “InternationalReference Pricing” OR “International PriceReferencing”. Relevant information was recorded andcombined with the results of the systematic literaturereview. Finally, additional literature gathered fromcontacts was also included.An excel spreadsheet was used to extract therelevant information on each endpoint for theselected studies. It includes paper titles in therows, endpoints in the columns and significantinformation from the texts being extracted andentered into the respective cells. A comprehensivesynthesis of the literature was carried out to identifykey trends related to ERP implementation acrosscountries. Results from other systematic literaturereviews were included if the selected endpointsin the review were different to the respectiveendpoints in this study. This process is significantin order to minimize bias of results.2.4 PRIMARY DATA COLLECTIONAs evidence drawn from the systematic literaturereview was not conclusive, primary evidence wascollected to complement the secondary evidencefindings. Primary evidence was gathered viaquestionnaires distributed to key stakeholders inall study countries, from which there were returnsfrom 21 countries i.e.: Belgium, Bulgaria, Jordan,Qatar, Italy, Brazil, South Africa, Romania, Slovenia,Spain, Germany, Egypt, Latvia, Poland, Portugal,Russia, Hungary, Greece, France, Estonia andSlovakia. Respondents included representativesfrom government agencies, industry representativesand academics, all of whom expressed personalviews on how ERP is implemented in their respectivecountries. Beyond understanding the characteristicsof ERP in different settings, other importantendpoints, such as the national and internationaleffects of implementing ERP, were addressed in thequestionnaires to increase understanding of howLONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
The Implementation of External Reference Pricing within and across Country Bordersdifferent ERP systems perform against 14 basicprinciples that each country should follow to achievean optimal ERP system (see Appendix 1) (Sullivan etal. 2017). The questionnaire was divided into foursections in order to address specific thematic areasaround ERP and its use within specific jurisdictions.These areas were (i) Objectives and Scope of ExternalPrice Referencing Systems, (ii) Administration andOperations, (iii) Methods for the Conduct of ExternalPrice Referencing, and (iv) Implementation ofExternal Price Referencing.12A combination of both primary and secondaryevidence is presented in the results section. Whenevidence from the systematic literature review wasused, primary data were used to validate the findings.In cases where minimal or outdated evidence wasdrawn from the systematic literature review, primarydata was used.Findings from both primary and secondary evidencewere then benchmarked against a framework of14 basic principles (Sullivan et al. 2017), whichcountries should follow in order to achieve anoptimal ERP system (Appendix 1).LONDON SCHOOL OF ECONOMICS AND POLITICAL SCIENCE
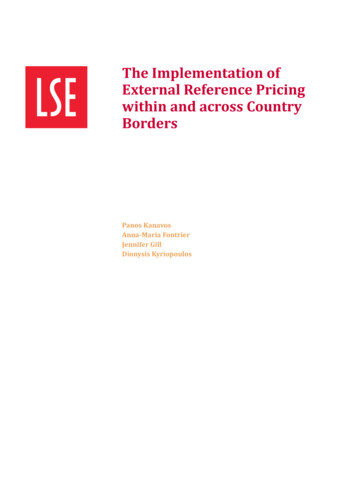
The Implementation of External Reference Pricing within and across Country Borders133. RESULTS3.1 RESULTS OF THE LITERATUREREVIEWThe database search yielded 6,877 studies and theresults of the systematic literature search werecombined with the results from the search of the WHO,the WHO Collaborating Centre for PharmaceuticalPricing and Reimbursement policies and the OECDonline databases. Additional literature was providedby our network. 3,979 studies remained and werescreened based on relevant titles and abstracts byremoving the duplicates using EndNote software(see Figure 1). From the 3,979 studies, 3,526 werepeer-reviewed papers and 453 were grey literature.549 papers were then downloaded and assessed foreligibility. Many studies were excluded because theydid not relate to ERP, others because they referredto internal reference pricing or because only theabstract was available, rather than the full text.The main body of 283 texts was then assessed. Thedetailed analysis of the studies providing evidence oneach of the endpoints included can be seen in Table2. 176 papers were included as final studies in thissystematic literature review, a significant proportionof which were grey literature (138 studies) with only38 peer-reviewed papers (Table 2). Throughout thetext, the evidence shown in the tables refers to thelatest available source.3.2 OBJECTIVE OF ERP ANDALIGNMENT WITH HEALTH SYSTEMOBJECTIVESERP is a commonly implemented pricing policy,related to the use of prices of similar drugs to set andbenchmark domestic prices (BMI Research, 2012).Generally, ERP has three main aims (Kanavos et al.,2010): (a) negotiate or set prices within a country,(b) negotiate coverage and reimbursement and (c)authorize product marketing. The use of ERP hasincreased significantly as a price control method(Kanavos and Vandoros, 2011) in in-patent medicinesand as a cost containment measure due to issues likethe global financial crash in 2008, the increase in lifeexpectancy and the increase in prevalence of chronicconditions (Rémuzat et al., 2015).The general aim of ERP is the attainment of lowdomestic prices to limit pharmaceutical spend. Forinstance, Greece implemented price controls throughFigure 1: PRISMA flow diagram with searchresults from the systematic literature reviewRecords identifiedthrough databasesearching (n 6,877)Additional recordsidentified throughother sources (n 143)Records after duplicates removed (n 3,979)Records screened(n 3,979)Full text articlesassessed for eligibility(n 549)Number of articlesassessed relative tothe inclusion criteria(n 283)Records excluded ofirrelevance of title orabstract (n 3,430)Full text articlesexcluded(n 266)Articles excludeddue to poor evidence(n 107)Final studies included(n 176)ERP to limit pharmaceutical and budget spending(Economou, 2010), Turkey introduced ERP in orderto control drug expenditure (BMI Research, 2016),Slovenia uses ERP as a tool to regulate the gro
4.1.1 Objectives and scope of external price referencing system 31 4.1.2 Administration and operations 31 4.1.3 Methods for the conduct of external price referencing 32 4.1.4 Implementation of external price referencing 33 4.2 Country Adherence to 14 Best Practice Principles 33