Transcription
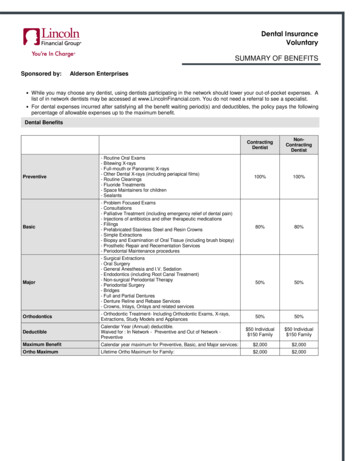
Dental InsuranceVoluntarySUMMARY OF BENEFITSSponsored by:Alderson Enterprises While you may choose any dentist, using dentists participating in the network should lower your out-of-pocket expenses. Alist of in network dentists may be accessed at www.LincolnFinancial.com. You do not need a referral to see a specialist. For dental expenses incurred after satisfying all the benefit waiting period(s) and deductibles, the policy pays the followingpercentage of allowable expenses up to the maximum benefit.Dental ventive- Routine Oral Exams- Bitewing X-rays- Full-mouth or Panoramic X-rays- Other Dental X-rays (including periapical films)- Routine Cleanings- Fluoride Treatments- Space Maintainers for children- Sealants100%100%Basic- Problem Focused Exams- Consultations- Palliative Treatment (including emergency relief of dental pain)- Injections of antibiotics and other therapeutic medications- Fillings- Prefabricated Stainless Steel and Resin Crowns- Simple Extractions- Biopsy and Examination of Oral Tissue (including brush biopsy)- Prosthetic Repair and Recementation Services- Periodontal Maintenance procedures80%80%Major- Surgical Extractions- Oral Surgery- General Anesthesia and I.V. Sedation- Endodontics (including Root Canal Treatment)- Non-surgical Periodontal Therapy- Periodontal Surgery- Bridges- Full and Partial Dentures- Denture Reline and Rebase Services- Crowns, Inlays, Onlays and related services50%50%Orthodontics- Orthodontic Treatment- Including Orthodontic Exams, X-rays,Extractions, Study Models and Appliances50%50%DeductibleCalendar Year (Annual) deductible.Waived for : In Network - Preventive and Out of Network Preventive 50 Individual 150 Family 50 Individual 150 FamilyMaximum BenefitCalendar year maximum for Preventive, Basic, and Major services: 2,000 2,000Ortho MaximumLifetime Ortho Maximum for Family: 2,000 2,000
Dental Benefits Cont'd.Waiting PeriodLincolnDentalConnect Service TypeBenefit Waiting PeriodLate Entrant Waiting PeriodBasic Services:0 Months0 MonthsMajor Services:0 Months0 MonthsOrthodontics:0 Months0 MonthsBy enrolling in the dental plan you and your enrolled family members will have access toLincoln DentalConnect , our free on-line dental health information Web site.Predetermination Allows you to find the amount covered prior to having a dental procedure. We recommend that you use thisof Benefitsservice when expenses are expected to exceed 300.Enrolling for CoverageEmployeeIf you do not want to enroll at this time, submit the completed waiver form to your plan administrator. If youwaive coverage now and want to enroll at a later date, you will be subject to the plan’s Late Entrantprovision which may limit covered services and Prior Carrier Credit will not be available.DependentDependent children may be covered up to age 26.BenefitTerminationThis coverage terminates when you terminate employment with this policyholder, or at your retirement.Exclusions and Other Limitations This highlights policy exclusions and limitations, see the policy for a full list. The plan does not cover services started before coverage begins or after it ends. Benefits are limited to those appropriate andnecessary procedures listed in the policy and any additional procedures required by state law. Benefits are not payable forduplication of services. Covered expenses will not exceed the policy’s usual and customary allowances. Plan benefits are not payable for a condition for which the claimant is eligible for benefits under worker’s compensation or asimilar law; are attributed to employment, military service; or are related to self-inflicted injury, involvement in an illegaloccupation, felony, or riot. If benefits for orthodontia are included, the plan does not cover any treatment plan started before coverage begins or duringthe benefit waiting period unless the member was receiving orthodontia benefits from this employer’s previous group dentalpolicy. In that case, Lincoln Financial will continue orthodontia benefits until the combined benefit paid by the two policies isequal to this policy’s lifetime orthodontia. Plan benefits are not payable if the orthodontic appliance was installed after the ageof 19. Alternative benefits provision: In certain situations there may be more methods of treating a dental condition. Your policyincludes an alternative benefits provision that may reduce benefits to the lowest cost, generally effective and necessary form oftreatment.For assistance or additional information Contact Lincoln Financial Group at(800) 423-2765; reference ID: ALDERSONENwww.LincolnFinancial.comThis policy does not include coverage of pediatric dental services as required under federal law. Coverage of pediatric dental services is available for purchase in the State ofColorado, and can be purchased as a stand-alone plan, or as a covered benefit in another health plan. Please contact your insurance carrier, agent, or Connect for HealthColorado to purchase either a plan that includes pediatric dental coverage, or an Exchange-qualified stand-alone dental plan that includes pediatric dental coverage.NOTE: This is not intended as a complete description of the insurance coverage offered. Controlling provisions are provided in the policy, and this summary does not modifythose provisions or the insurance in any way. This is not a binding contract. A certificate of coverage will be made available to you that describes the benefits in greater details.Should there be a difference between this summary and the contract, the contract will govern.Insurance products are issued by The Lincoln National Life Insurance Company (Fort Wayne, IN), which does not solicit business in New York, nor is it licensed to do so.Product availability and/or features may vary by state. Limitations and exclusions apply. Not for use in New York. 2015 Lincoln National Corporation- ALDERSONEN-LFG - 11/15-FLEX - PPO - Voluntary- Gen -7/17/2017
Group Vision InsuranceVoluntarySUMMARY OF BENEFITSSponsored by:Alderson EnterprisesProvider Network Lincoln VisionConnect proudly partners with SpecteraEyecare Network for all of your needs.Be sure to advise your provider your benefits arecovered under Spectera!In-NetworkOut-of2NetworkExam 10 CopayN/AMaterials 25 CopayN/A100% after CopayUp to 40100% (Up to 130)Up to 45Single Vision100% after CopayUp to 40Bifocal100% after CopayUp to 60Trifocal100% after CopayUp to 80Lenticular100% after CopayUp to 801CopaysEye Examination3FramesYou may choose any provider; however using providers inour network should lower your out-of-pocket expenses.A list of participating providers may be accessed athttp://lvc.lfg.com or by calling toll-free at 1-800-440-8453.Eyeglass Lenses4Contact LensesOnline Member InformationPlease visit the member website for more details on the Lincoln VisionConnect plan. The website will provide anup-to-date directory of In-Network providers, printable IDCards and more.Covered contact lens selectionElective contact lensesMedically necessary contactlenses5Please follow these helpful hints to register online: Visit http://lvc.lfg.com and select ‘Register Now’Under the section Enter your identifying informationenter the last 4 digits of your social security number anddate of birth.The password will need 1 alpha, 1 numeric, 1character (!,#, ,%,*, ).Complete all other areas, as required.Eligibility Employee – a full-time employee, actively at workDependent – Spouses and Dependent children maybe covered up to age 26.Popular Lens OptionsScratch resistant coating100% after CopayUp to 125Up to 125Up to 125100% after CopayUp to 210Member CostNo CostN/APolycarbonate Children*(*Under Age 20)Standard progressive lensesNo CostN/AUp to 70N/AStandard anti-reflective coatingUp to 40N/APolycarbonate (Age 20 )Up to 33N/ALASIK Vision CorrectionDiscount offered through Laser Vision Network of America (LVNA). Visit www.lincolnvisionlasik.com Free initial consultation to all in-network providers Up to 15% off standard prices Up to 5% off promotional pricingSee description of Footnotes on Page 2Service FrequenciesService may be provided once within the below period, as defined by the last date ofservice. Contact Lens would be provided in lieu of eyeglass lensesExamLensFramesExclusionsPage 1 of 4 2016 Lincoln National Corporation - ALDERSONEN - 10/16-LVC9 - Voluntary-TX12 months12 months24 months
The following services and materials are excluded from coverage under the Policy: Post cataract lenses; Non-prescriptionitems; Medical or surgical treatment for eye disease that requires the services of a physician; Worker’s Compensation servicesor materials; Services or materials that the patient, without cost, obtains from any governmental organization or program;Services or materials that are not specifically covered by the Policy; replacement or repair of lenses and/or frames that havebeen lost or broken; Cosmetic extras, except as stated in the Policy’s Table of Benefits.Footnotes1. In-Network Benefits: Exam and materials copays and patient options are paid to the network provider by the planparticipant at time of service.2. Out-of-Network Benefits: The plan participant pays full fee to the provider at time of service and the member submits aclaim for reimbursement of services rendered up to maximum allowance. There are no copays.3. Frame Benefit: Our frame allowance can be used to cover many popular frames on the market today. The member isonly required to pay the remaining balance after the 130 retail frame allowance is used. Up to a 30% discount is appliedin excess of the allowance at participating Providers.4. Contact Lenses: Contact lenses are provided in lieu of eyeglasses (lenses and frame). Benefits may only be appliedunder one of the three benefit options. When purchasing from the Covered Contact Lens Selection, the benefit is covered-in-full (after copay if applicable).This includes fitting/evaluation fees, contacts (including up to 4 boxes of disposables, depending on prescription andplan selected) and up to two follow-up visits. The Covered Contact Lens Selection is not available at Wal-Mart,Sam’s Club or Costco. All other elective contact lenses are covered up to a 125 allowance and the materials copay does not apply. Medically necessary contact lenses are determined at the eye care provider’s discretion. If an out-of-network providerconsiders contacts are necessary, members should ask their out-of-network provider to contact us concerning thereimbursement that we will make before they purchase such contacts.5. Popular Lens Options: A variety of lens types, coatings and other upgrades are available to the member. Members canreceive up to a 20-40% discount on lens options when visiting in-network providers. Please review the full list of coveredoptions on the attached Lens Flyer. All other lens options not listed are offered up to a 20% discount off the retail price atparticipating providers.Additional Discounts Additional materials, such as additional pairs of eyeglasses or contact lenses, requested by the member may be offered upto a 20% discount at participating providers. Members may also purchase mail order contact lenses online at a 10% discount. The member will visitwww.myvisionlenses.com and will be required to submit an Out-of-Network claim for reimbursement.Page 2 of 4 2016 Lincoln National Corporation - ALDERSONEN - 10/16-LVC9 - Voluntary-TX
In-network Lens OptionsEyeglass OptionsTypeCOATINGSStandard Scratch CoatingTintUV CoatingPhotochromicCostTypeCostN/C 14 16 67Scratch WarrantyStandard Anti-Reflective CoatingPremium Anti-Reflective CoatingPlatinum Anti-Reflective Coating 10 40 80 90LENSESStandard ProgressivePremium Progressive 70 150Deluxe ProgressivePlatinum ProgressiveRoll and Polish Edges 110 250 13MATERIALSHigh Index ( / 1.66)High Index (1.60-1.73) 53 63PolycarbonatePolycarbonate For Dependents(Dependent children under age 20) 33 0This list highlights the discounted cost on the most popular lens options. Most other lens options are offered at upto a 20% discount off retail (Options and prices are subject to change. Check with your provider. May not apply atsome locations.Contact OptionsDaily WearAlcon DAILIES AquaComfort Plus (30 lenses per box)Alcon Focus DAILIES Progressive ADC (30 lenses per box)Alcon Focus DAILIES Toric ADC (30 lenses per box)CooperVision Proclear 1 day (30 lenses per box)Vistakon 1 Day Acuvue Moist (30 lenses per box)Biweekly wearAlcon Freshlook Handling Tint (6 lenses per box)CooperVision Avaira (6 lenses per box)CooperVision Biomedics XC (6 lenses per box)CooperVision Biomedics 55 premier (6 lenses per box)Valeant Soflens38 (6 lenses per box)Vistakon ACUVUE 2 (6 lenses per box)Vistakon ACUVUE ADVANCE PLUS (6 lenses per box)Monthly WearAlcon AIR OPTX AQUA (6 lenses per box)CooperVision Biofinity (6 lenses per box)CooperVision Frequency 55 Aspheric (6 lenses per box)CooperVision Frequency 55 (6 lenses per box)CooperVision Proclear Sphere (6 lenses per box)Valeant PureVision (6 lenses per box)Valeant Ultra (6 lenses per box)Vistakon ACUVUE Vita (6 lenses per box)Eyeglass and Contact Selection list subject to change.Contact lenses not appearing on the Selection are considered non-Selection, unless otherwise specified on the individual plan outline. Anallowance is provided toward the purchase of non-Selection contacts.Contact Lens Selection list does not apply at Costco , Walmart or Sam’s Club locations. The non-Selection allowance will be appliedtoward the purchase of all contacts at Costco, Walmart and Sam’s Club.The eye doctor’s prescribed wearing schedule may affect replacement frequency. All trademarks are the property of their respective ownersPage 3 of 4 2016 Lincoln National Corporation - ALDERSONEN - 10/16-LVC9 - Voluntary-TX
Out-of-Network Claim SubmissionTo file a claim for reimbursement for Services rendered by a non-Network Provider, provide the following information: Your itemized receipts; Subscriber name; Subscriber's identification number; Patient name; and Patient date of birth.Submit a claim by mail to:Submit a claim by fax to:Claims Department – LincolnVisionConnectP.O. Box 30978Salt Lake City, UT 84130(248) 733-6060Questions? Please Contact our Customer Service Department at 1-800-440-8453If there is any discrepancy between this benefit summary and the policy, the policy shall control. Thissummary is not intended to contain a complete description of the coverage offered. This summary doesnot modify the policy. This is not a binding contract.The Lincoln VisionConnect program is marketed by The Lincoln National Life Insurance Company (Fort Wayne, IN), which does not solicitbusiness in New York, nor is it licensed to do so. In New York, this program is marketed by Lincoln Life & Annuity Company of New York(Syracuse, NY). Both are Lincoln Financial Group companies.Lincoln VisionConnect is a registered trademark of Lincoln National Corporation.Lincoln VisionConnect vision coverage is provided by or through UnitedHealthcare Insurance Company, located in Hartford, Connecticut;UnitedHealthcare Insurance Company of New York, located in Islandia, New York; or their affiliates. Administrative services are provided bySpectera, Inc.; UnitedHealthCare Services, Inc.; or their affiliates. Plans sold in Texas use policy form number VPOL.06.TX or VPOL.13.TXand associated COC form number VCOC.INT.06.TX or VCOC.CER.13.TX. Plans sold in Virginia use policy form number VPOL.06.VA orVPOL.13.VA and associated COC form number VCOC.INT.06.VA or VCOC.CER.13.VA. This policy has exclusions, limitations and termsunder which the policy may be continued in-force or discontinued. For costs and complete details of the coverage, contact LincolnVisionConnect.The contracting entity for Spectera Eyecare Networks is Spectera, Inc.UnitedHealthcare Insurance Company is not a Lincoln Financial Group company. Lincoln Financial Group is the marketing name for LincolnNational Corporation and its affiliates. Affiliates are separately responsible for their own financial and contractual obligations.Page 4 of 4 2016 Lincoln National Corporation - ALDERSONEN - 10/16-LVC9 - Voluntary-TX
2015 Lincoln National Corporation - ALDERSONEN-LFG - 11/15-FLEX - PPO - Voluntary- Gen -7/17/2017 Dental Benefits Cont'd. Waiting Period Service Type Benefit Waiting Period Late Entrant Waiting Period Basic Services: 0 Months 0 Months Major Services: 0 Months 0 Months Orthodontics: 0 Months 0 Months Lincoln DentalConnect