Transcription
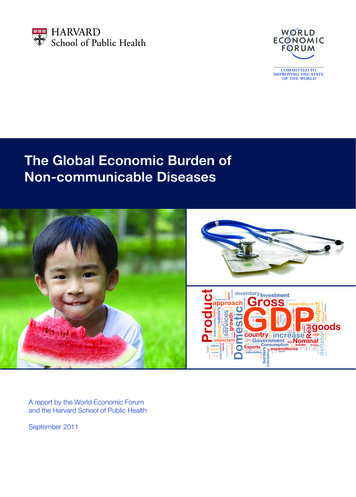
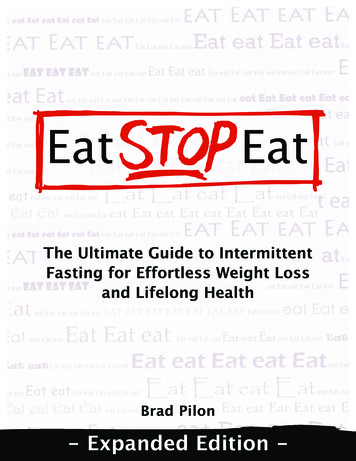
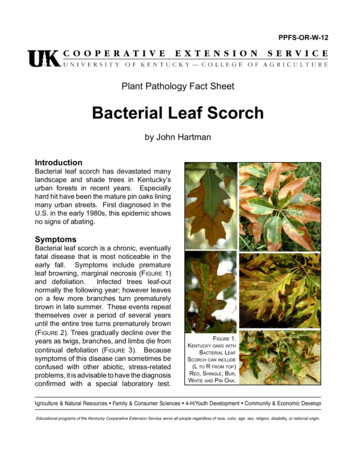
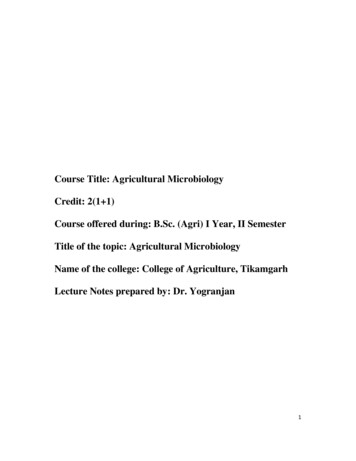
Clinical RESEARCH/AUDITIncreased bacterial burden andinfection: NERDS and STONESThe purpose of this article is to provide practitioners with an overview of wound infection/inflammation and bacterial balance and to offer a guide to the assessment and treatment of chronicwounds. Assessing the wound for clinical signs and symptoms of inflammation and infection is animportant part of preparing the wound bed for healing. This article presents easy-to-use clinicalcriteria for diagnosing superficial bacterial burden and deep tissue infection (NERDS and STONES)as well as an organised approach to the selection of appropriate topical and systemic treatments.R Gary Sibbald, Kevin Woo, Elizabeth AyelloKEY WORDSInfectionInflammationNERDSSTONESThe wound bed preparationparadigm allows the clinicianto optimally evaluate a patientwith a chronic wound to delineatean accurate diagnosis and initiatetreatment. It requires a holistic, teamapproach to assessing the wholepatient, treating the underlyingcause(s), and addressing patientcentered concerns, all of which mustbe considered before examiningthe wound itself (Sibbald et al,2003). Clinical documentation ofR Gary Sibbald, BSc, MD, FRCPC (Med) (DERM), FAPWCA, MEdis Professor of Public Health Sciences and Medicine, Universityof Toronto and Toronto, Ontario, Canada and Director of theWound Healing Clinic and The New Women’s College Hospital,Toronto, Ontario, Canada and Clinical Associate Editor, Advancesin Skin and Wound Care, Ambler, PA. Kevin Woo, RN, MSc, ACNPGNC(C) is Clinical Scientist/Nurse Practitioner, Wound HealingClinic and The New Woman’s Hospital, Toronto, Ontario, Canada.Elizabeth A Ayello, PhD, RN, APRN,BC, CWOCN, FAPWCA, FAANis Faculty, Excelsior College of Nursing, Albany, NY and SeniorAdvisor, The John A Hartford Institute for Geriatric Nursing, NewYork and President, Ayello, Harris and Associates, New York, andClinical Associate Editor, Advances in Skin and Wound Care,Ambler, PA.the wound characteristics (debris ornecrosis, increased bacterial burdenor persistent inflammation, and theamount of exudate) serves as thebenchmark for the selection oftopical treatment.This article focuses specifically onpersistent inflammation and infection, andit is the first in a four-part series that willaddress the local wound components ofwound bed preparation (debridement,infection/inflammation, moisture balance,and the edge effect as a marker for activeand advanced therapies). The debateabout appropriate terms to describeinfection and inflammation, as well asthe use of clinical enablers for improvedpractice, will also be described.Examine the evidenceEvidence-based medicine (Sackett,2000) is fast becoming a requirement inwound care, with clinicians demandingevidence before the introduction ofnew products or a change in woundcare practices (Ryan et al, 2003).Sackett (2000) defined evidence-basedwound management as ‘the integrationof best research evidence with clinicalexpertise and patient values.’ Scientificevidence should be translated forcurrent practice. For example, despitethe findings in the 1960s that woundstreated according to moist woundhealing principles will heal at a fasterrate, toxic local antiseptic agents orsaline wet-to-dry dressings that inhibithealing are still commonly prescribed.The wound bed preparation conceptwas first described in 2000 by Sibbald etal (2000) and Falanga (2000). The Sibbaldet al (2000) model encourages theclinician to examine the whole patient,treating the cause and patient-centeredconcerns before focusing on the holein the patient. Local wound care can beoptimized using moist healing principlesby addressing three components:debridement, bacterial balance orpersistent inflammation, and moisturebalance. The algorithm in Figure 1combines the components necessary forobtaining maximal benefits from today’swound care products (Sibbald et al,2003; Sibbald et al, 2000) and applies theprinciples of evidence-based medicine.The authors of the present articlehave used the wound bed preparationmodel to develop a practical clinicalguide to the treatment of criticalcolonization and infection in chronicwounds.Balance and resistanceAll chronic wounds contain bacteria.But whether the wound is in bacterialbalance (contamination with organismson the surface or colonization withorganisms in the tissue arranged in microcolonies without causing damage) orbacterial imbalance (critical colonizationand infection) is of primary importanceto healing (Figure 2). A continuum ofbacterial presence progressing frombacterial balance to bacterial damage ina chronic wound is illustrated in FigureWounds25-46NERDS 1UK,2007, Vol 3, No 22512/6/07 3:38:37 pm
Clinical PRACTICE DEVELOPMENTChronic ulcerTreat causeLocal wound carePatient-centered concernsTissue-Debridement ofdevitalized tissueSuperficial Infection/Chronic InflammationMoisture balanceWatch bacterial burdenRole of ionized silverOther topical dressings and antisepticsEdge-Non-healing woundFigure 1. New wound bed preparation model. Source: Reprinted courtesy of Wound Care Canada, the officialpublication of the Canadian Association of Wound Care, http://www.cawc.net. Copyright 2006. All rights reserved.3. The diagnosis of infection shouldbe made clinically based on signs andsymptoms in and around the local woundbed, the deeper structures, and thesurrounding skin. The potential damagecaused by invading wound bacteria isdetermined by the following equation:infection number of organisms x organismvirulence. The most important factor inthis equation is host resistance, whichis defined as the ability of the host toresist bacterial invasion and damageby mounting an immune response(increased bacterial burden or infection).Systemic and local factors can decreasehost resistance. Systemically, an adequateblood supply is needed for woundhealing. A decreased or inadequateblood supply favors bacterial proliferationand damage that may prevent or delayhealing. Uncontrolled edema, smoking,poor nutrition, diabetes with a poorlycontrolled blood glucose level, excessalcohol intake, drugs that interfere withthe immune system, or immunodeficiencydiseases may all challenge wound healing.Local factors inhibiting healing mayinclude a large wound size, local presenceof foreign bodies (prosthetic joints,retained thread of gauze, or suture), andan untreated deeper infection, such asosteomyelitis (Dow, 2001).ContaminationorcolonizationCritical colonizationorinfectionBacterial balanceBacterial balanceWound bed preparationFigure 2. Balancing bacterial burden. Copyright Ayello, 2006.2625-46NERDS 30WoundsUK,Most bacteria enter the wound bedthrough external contamination fromthe environment, dressings, the patient’sbody fluids, or the hands of the patientor health care provider. If the surfaceorganisms attach to the tissue andmultiply, colonization is established but abacterial balance remains.However, if bacteria continue tomultiply, critical colonization or localinfection (covert infection, increasedbacterial burden) may develop.Wound-related bacteria can releasemetalloproteases and other mediatorsof inflammation that will lead to localtissue damage. The first sign of criticalcolonization or local infection may bea delay in the healing process so thatthere is no change in the wound sizemeasured with a simple length x widthmeasurement (longest length and thewidest width at right angles). Exudateon the surface can increase at thisstage as an inflammatory reaction tothe surface tissue damage. The exudatemay be clear or serous before it isfrankly purulent or hemorrhagic.Gram-positive organisms maybe the first to invade a wound withdecreased host resistance, followedby Gram-negative bacteria and thenanaerobic species. A foul odor mayaccompany the exudate due to tissuebreakdown caused by the presence ofthese Gram-negative and anaerobicorganisms. Small areas of yellow tobrown slough may be present on thesurface of the wound as a result ofa hostile local environment, leadingto surface cell death and local tissuenecrosis. The granulation tissuemay bleed easily due to bacterialstimulation of vascular endothelialgrowth factor (VEGF), resulting in anexcess formation of new blood vessels.Exuberant (beefy red) granulationbuilds up on the surface; bacterialinterference results in a poor quality ofcollagen matrix that will not supportre-epithelialization and healing. Thesesigns are localized in the superficialwound bed and are potentiallytreatable with topical agents, includingantimicrobial dressings (Gardner et al,2001; Cutting et al, 1994; Schultz et al,2003).2007, Vol 3, No 212/6/07 3:38:39 pm
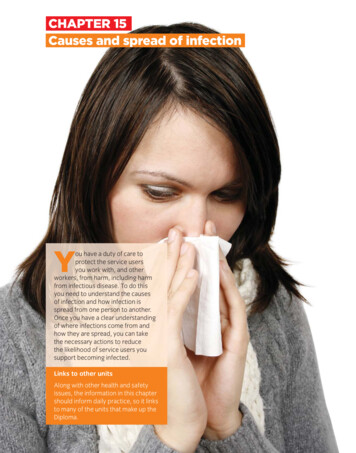
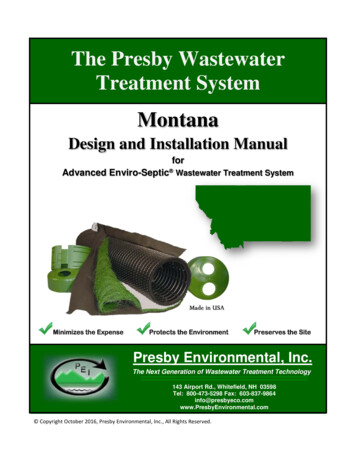
Clinical PRACTICE DEVELOPMENTContaminated or colonized Low Bacteria are present on the wound surface(contaminated). A steady state of replicatingorganisms are attaching to the wound tissueand multiplying but they are not associated withtissue damage or delayed healing (colonization). Critically colonized(local infection, covert infection,increased bacterial burden) Medium 8The bacterial burden in the wound bed isincreasing.8Initiates the body’s immune response(inflammation).8The wound is no longer healing at theexpected rate: wound size is not decreasing.8Look for the signs outlined in the enablerNERDS. Infected High 8Bacteria are present within the wound and havespread to the deeper and surrounding tissue.They are multiplying and causing tissue damage.8There is an associated host inflammatoryresponse that has now spread to the deepertissue and surrounding skin.8The wound is painful and may increase in sizewith potential satellite areas of breakdown.8Look for the signs outlined in the enablerSTONES.Figure 3. Progression of bacterial balance to bacterial damage in a chronic wound.Table 1Compartment model of chronic wound bacterial burden and infectionCompartmentTreatmentAbove wound and dressingInfection control andantibacterial contentSuperficial wound surface (NERDS)Topical antimicrobialDeep and periwound compartments (STONES)Systemic agentsSystemic infectionParenteral agentsManaging infectionBacterial damage can extend beyondthe local wound bed with a lowerhost resistance. More extensivebacterial damage results in a deeperand surrounding skin compartment2825-46NERDS 32WoundsUK,infection that usually requires systemicantimicrobial treatment (Table 1).The presence of surrounding skin pain,warmth, and swelling should alert theclinician to the possibility of a coexistingsoft tissue cellulitis. If the deep portion ofthe ulcer probes to bone, osteomyelitisis a possibility, especially in persons withdiabetes and neurotrophic foot ulcers(Grayson et al, 1995). With infection ofthe surrounding or deeper structures, thewound often increases in size and satelliteareas of breakdown may occur (Figure 4).At this stage, bacterial testing proceduresmay be useful.The gold standard forbacterial damage in a wound is the tissuebiopsy for culture. More than 1.0 x 106(Dow, 2001) colony-forming organismsper gram of tissue is indicative of sufficientbacteria to usually cause infection in thedeep compartment. A bacterial swabcan be performed to give an accuratesemiquantiative estimate of bacterialumbers.The swab should be taken afterthe wound has been adequately cleaned,2007, Vol 3, No 212/6/07 3:38:41 pm
Clinical PRACTICE DEVELOPMENTand the Levine method should be utilized.The swab is placed on healthy granulationtissue and enough pressure is applied toextract fluid.The swab is then rotated360 degrees and placed in the transportmedia. Surface slough and debris shouldbe avoided. If the wound surface is dry,the swab can be premoistened in thetransport media before swabbing thewound. A heavy growth or 4 bacteriafrom the swab culture can often beequated to approximately 105 colonyforming units of bacteria per gram oftissue. Bacterial culture can help todetermine antimicrobial sensitivities forselection of appropriate oral or parentalantimicrobial treatment and to identifycolonization with resistant organismssuch as methicillin-resistant Staphylococcusaureus (MRSA). Clinicians often mustmake treatment decisions before theswab results are available and fine-tunethe treatment if the patient does notrespond or if an unsuspected organismis isolated. In general, wounds of lessthan one month’s duration should betreated for Gram-positive organisms.If the wound has been present formore than one month or the patient isimmunocompromised (including personswith diabetes), the patient will need tobe protected against Gram-positive,Gramnegative, and anaerobic organisms(Dow et al, 1999).Clinicians can apply this newunderstanding of bacterial balanceand imbalance by using the followingrecommendations or enablers of bestpractice for wound infection.1. Identify and correct the cause and cofactorsthat may inhibit healing as well as address patientcentered concernsIt is important to make an accuratediagnosis of the underlying cause of thewound and correct the cause of impairedhealing as a first step. For example:8 Venous disease without coexistingarterial disease should receiveappropriate compression for edemacontrol.8 A pressure ulcer requires not onlypressure offloading but also nutritionalassessment and treatment, correctionof friction and shear, optimizationof mobility and incontinencemanagement.3025-46NERDS 34WoundsUK,8 Assess the vascular supply of patientswho have a foot ulcer and diabetes toensure adequate circulation for woundhealing.8 Evaluate for infection as classicallydefined by pain, erythema, edema, andwarmth.8 In persons with neuropathy (diabetesand other causes) check for callusformation on the feet to determineif pressure offloading is needed.Thepresence of callus indicates excesslocal pressure. If a blister is present,consider frictionand shear. An easyway to remember the approach toa person with neuropathy (usuallydue to diabetes) is to remember themnemonic ‘VIPs’, not meaning veryimportant persons but, alternatelyrepresenting Vascular supply, Infectioncontrol and Pressure downloadingalong with Sharp Surgical debridement.Patients with acute ulcers andpostsurgical wounds require the sameholistic assessment to determineinhibitors to healing, including infections,coexisting diseases, and lifestyle choices.In addition to treatment of thecause, a paradigm shift is needed inthe plan of care to make the patientcentral to all treatment decisions. Thispatient-centered approach representsa paradigm shift moving away fromcompliance (to obey an order orcommand) to adherence (to followthrough on a treatment plan fromthe patient’s perspective) and, finally,to coherence (to have a negotiatedtreatment with both the patient andhealth care provider perspective). Askpatients what their expectations andgoals are for their care.if there is adequate blood supply, thecause is corrected, and patient-centeredconcerns have been addressed. Amaintenance wound has enough bloodsupply to heal but the patient cannotadhere to treatment due to personal orsystem-related factors (e.g. they cannotafford shoes and inserts or a removablecast walker for offloading).A wound is nonhealable if the causecannot be corrected. For leg and footulcers with a palpable pulse, the bloodsupply is usually adequate for healing(80mmHg and higher). If the pulse is notpalpable, Doppler examination of theankle-brachial pressure index (ABPI) isnecessary to determine if the woundis healable. The pressure in the dorsalispedis artery should be at least 50% ofthe pressure in the brachial artery, or anABPI of 0.5. Some patients have calcifiedvessels in the leg producing a falselyhigh ankle brachial pressure ratio (20%of all patients and 80% of patients withdiabetes).A full arterial Doppler of the lowerextremity with toe pressures is usuallyrecommended when an ABI is morethan 1.2. Toe systolic pressure providesan accurate vascular assessmentbecause the artery in the large toeis of a small caliber without a fullydeveloped adventitial layer to facilitatecircumferential calcium deposits. Forhealability, a person with diabetesshould have a toe pressure of morethan 50mmHg. Healing may occur if thepressure is between 30 and 50mmHgand if all other factors are optimized.Clinicians must also consider paincontrol and issues around the quality oflife and activities of daily living that maybe affected by the presence of a chronicwound. These aspects of care are oftenmore important to the patient than tothe clinician.Many hyperbaric oxygen centersalso measure transcutaneous oxygensaturation. This test requires expensiveequipment and is labor intensive. Valuesover 40mmHg are normal; values of30 to 39mmHg indicate some oxygenimpairment. Values of 20 to 29mmHgindicate moderate impairment, and avalue below 20mmHg indicates severeischemia; healing is unlikely.2. Differentiate the wound’s ability to heal: classify ashealable, maintenance, or nonhealable woundThe approach to a chronic wounddepends on the ability of the wound toheal. A wound is considered healable3. Use topical antiseptics for nonhealable ormaintenance woundsMoist interactive healing is the goldstandard for patients with adequateblood supply who can produce healthy2007, Vol 3, No 212/6/07 3:38:42 pm
Clinical PRACTICE DEVELOPMENTgranulation tissue, reepithialization, andmature healing.In a wound that does not have theability to heal (e.g. inadequate vascularsupply or gangrene), moisture balance andactive debridement are contraindicated.Instead, clinicians should focus on the useof topical antimicrobial and antiseptics todecrease the local bacterial count andsubsequent invasion of organisms intoproximal viable tissue (Table 2).The lowest tissue toxicity inthis group of agents occurs withchlorhexidine and povidone-iodine(Schultz et al, 2003). Both of theseagents have a low sensitization potentialand a broad spectrum of antibacterialaction. Povidone-iodine applicationmay be associated with local stingingand should be used with caution onvery large wounds and in persons withthyroid disease because of the potentialfor absorbed iodine to interfere withthyroid gland function. Both of theseagents can be used long term with alow incidence of tissue toxicity. Aceticacid (0.5 to 1.0%) is toxic to granulationtissue but is very effective as a compressor soak (often for 5 to 10 minutesat the time of dressing change) forPseudomonas with green discolorationand a distinctive sickeningly sweet odoron the wound surface. This agent may beused short term when bacterial burdenis of more concern than tissue toxicity.Aniline dyes, such as scarlet red,Proflavine, and crystal violet, will treatGram-positive organisms but have hightissue toxicity and may act as carcinogens.Use of these dyes is not recommended.Sodium hypochlorite solutions consistof bleach and are appropriate fordecontaminating inanimate objects,but they are not ideal on wounds;they combine high tissue toxicity withantibacterial action. Quaternary ammoniacompounds have the highest tissuetoxicity of all topical agents in this group.4. Determine if the wound is in bacterial balance, ifit has an increased bacterial burden in the superficialcompartment or infection in the deep compartment,or both the superficial and deep compartments areaffectedEarly recognition of bacterial imbalance,3225-46NERDS 36WoundsUK,including infection, is crucial to woundmanagement. Criteria to identify subtleclinical signs of infection have beensuggested by two independent teams ofresearchers (Gardner et al, 2001; Cuttinget al, 2005). Both identify exudate andfriable granulation tissue as indicators ofinfection (Gardner et al, 2001; Cutting etal, 2005).Interestingly, both sets of researchersfound a change in wound pain to bea leading indicator of infection. Usinga Delphi process, Cutting et al (2005)extended their research to determine amore precise wound-type identificationof infected wounds. They determinedthe following clinical indicators ofinfection to be common to all wounds:cellulitis, malodor, pain, delayed healing,wound deterioration or breakdown,and increase in exudate volume (exceptfor acute wounds healing by primaryintention and full-thickness burns)(Cutting et al, 2005).Cutting et al (2005) noted crepitusfor pressure ulcers, phlegmon forneuropathic/diabetic ulcers, increase inlocal skin temperature for venous ulcers,and dry necrosis that may turn moistand boggy at the edges of the necrotictissue for arterial disease associatedtissue breakdown.Clinicians may find the mnemonics,or enablers, NERDS and STONES helpful in making wound infectionassessments (Figures 4–5). For superficialinfection, think of NERDS:8 Nonhealing wounds8 Exudative wounds8 Red and bleeding wound surfacegranulation tissue8 Debris (yellow or black necrotictissue) on the wound surface8 Smell or unpleasant odor from thewound.For deep infection, think of STONES:8 Size is bigger8 Temperature is increased8 Os probe to or exposed bone8 New or satellite areas of breakdown8 Exudate, erythema, edema8 Smell.By using this superficial and deepseparation, clinicians can identify woundswith increased superficial bacterialburden that may respond to topicalantimicrobials and deep infections thatusually require the use of systemicantimicrobial agents. Also, rememberthat bacterial swabs can guide therapyor identify resistant organisms, butthe diagnosis of increased superficialbacterial burden or deep infection ismade clinically. The bacteria in NERDScan be thought of as misbehaving. Treatsuperficial increased bacterial burdentopically. Clinicians often need to lookfor two or three of the signs andsymptoms of NERDS before makinga diagnosis of increased superficialbacterial burden.When considering whether thepatient has a deeper compartmentinfection, remember that STONES sinkTable 2Effects of topical agentsAntiseptic agentEffectsChlorhexidine*Broad spectrum/low toxicityPovidone-iodine*Broad spectrum/low toxicityAcetic acid**Effective against PseudomonasDyes: scarlet red, proflavineEffective against Gram-positive bacteria,ineffective against Gram-negative bacteriaSodium hypochlorite: Dakin’s, EusolToxic to granulation tissueHydrogen peroxideEffective only when it is effervescentQuaternary ammonia: CetrimideVery high toxicity* preferred; ** selected use2007, Vol 3, No 212/6/07 3:38:42 pm
Clinical PRACTICE DEVELOPMENTLetterKey information to knowCommentsNonhealing wound8To determine a healing trajectory, the8The wound is nonhealing despitewound size should decrease 20–40%appropriate interventions (healableafter four weeks of appropriatewound with the cause treated andtreatment to heal by week 12.patient-centered concerns addressed). 8If the wound does not respond to8Bacterial damage has caused antopical antimicrobial therapy, considerincreased metabolic load in the chronica biopsy after 4 to 12 weeks to rulewound creating a proinflammatoryout an unsuspected diagnosis, such aswound environment that delays healing.vasculitis, Pyoderma gangrenosum, ormalignancy.NExudative woundE8An increase in wound exudate can beindicative of bacterial imbalance andleads to periwound maceration.8Exudate is often clear before itbecomes purulent or sanguineous.8Increased exudate needs to trigger theclinician to assess for subtle signs ofinfections.8Protect periwound area using theLOWE memory jogger (liquid filmforming acrylate; ointments; windoweddressings; external collection devices)for skin barrier for wound margins.8When the wound bed tissue is brightred with exuberant granulation tissuesand bleeds easily, bacterial imbalancecan be suspected.8Granulation tissue should be pink andfirm. The exuberant granulation tissuethat is loose and bleeds easily reflectsbacterial damage to the formingcollagen matrix and an increasedvasculature of the tissue.8Necrotic tissue and debris in thewound is a food source for bacteriaand can encourage a bacterialimbalance.8Necrotic tissue in the wound bed willrequire debridement in the presenceof adequate circulation.8Debridement choice needs to bedetermined based on wound type,clinician skill, and resources.8Smell from bacterial byproductscaused by tissue necrosis associatedwith the inflammatory response isindicative of wound related bacterialdamage. Pseudomonas has a sweetcharacteristic smell/green color;anaerobes have a putrid odor due tothe breakdown of tissue.8Clinicians need to differentiatethe smell of bacterial damagefrom the odor associated with theinteraction of exudate with differentdressing materials, par ticularly somehydrocolloids. Odor may come fromsuperficial or deep tissue damage,and this should not be relied onalong with exudate alone as the onlysigns of increased superficial bacterialburden.Red and bleeding woundRDebris in the woundDSmell from the woundSFigure 4. NERDS: superficial increased bacterial burden.3425-46NERDS 38WoundsUK,2007, Vol 3, No 212/6/07 3:38:44 pm
Clinical PRACTICE DEVELOPMENTKey information to knowLetterCommentsSize is bigger8Size as measured by the longest length8Clinicians need to have a consistentand widest width at right angles to theapproach to measurement.longest length. Only very deep wounds8An increased size from bacterialneed to have depth measured with adamage is due to the bacteriaprobe.spreading from the surface to the8An increased size may be due tosurrounding skin and the deeperdeeper and surrounding tissue damagecompartment. This indicates that theby bacteria or alternately because thecombination of bacterial number andcause has not been treated or there isvirulence has overwhelmed the hosta systemic or local host factor impairingresistance.healing.STemperature increasedTOs (probes to orexposed bone)O8With surrounding tissue infection,temperature is increased. This may beperformed crudely by touch with agloved hand or by using an infraredthermometer or scanning device. Thereshould be a high index of suspicionfor infection if 3ºF difference intemperature exists between 2 mirrorimage sites.It is important to distinguish betweeninfection and the other 2 potential causesof temperature change:8A difference in vascular skin supply(decreased circulation; is colder)8Inflammatory conditions are not usuallyas warm, but they can demonstratea marked increase temperature withextensive deep tissue destruction(acute Charcot joint).8There is a high incidence ofosteomyelitis if bone is exposed or ifthe clinician can probe to the bone in aperson with a neurotrophic foot ulcer.8An MRI is probably the mostdiscriminating diagnostic test whenavailable and considered necessary fordiagnostic dilemmas.8Radiographs and bone scans are lessreliable for diagnosis of osteomyelitiswith loss of bone mass that occurswith neuropathy. Radiographs of wellcalcified bone, such as pressure ulcersof the pelvis, may be more reliable. Themajority of ulcers that probe to bonein other locations are less likely to beassociated with osteomyelitis.8Note the satellite areas of skinbreakdown that are separated fromthe main ulcer.8It is important to remember this maybe due to the cause of the wound,infection, or local damage being leftuncorrected.8Search for the cause of the satelliteareas of breakdown and the need tocorrect the cause.8Check for local damage and considerinfection, increased exudate, or othersources of trauma.New areas of breakdownNFigure 5. STONES: deep compartment infection.3625-46NERDS 40WoundsUK,2007, Vol 3, No 212/6/07 3:38:45 pm
Clinical PRACTICE DEVELOPMENTExudate, erythema, edemaESmellS8For exudate control, determine thecause and then match the absorbency8All of the features here are due to theof the dressing (none, low, moderate,inflammatory response. With increasedheavy) to the amount of exudate frombacterial burden, exudate oftenthe wound.increases in quantity and transforms8Assess surrounding skin to evaluatefrom a clear or serous texture to frankfor maceration. Again, use the LOWE purulence and may have a hemorrhagicmemory jogger (liquid film-formingcomponent. The inflammation leadsacrylate; ointments; windowedto vasodilatation (erythema), and thedressings; external collection devices)leakage of fluid into the tissue willfor skin barrier for wound margins.result in edema.8For erythema and edema control, thecause or the tissue infection needs tobe treated.8Make sure the smell is from organisms8Bacteria that invade tissue have a ‘foul’and not from the normal distinct odorodor. There is an unpleasant sweetfrom the interaction of exudate withodor from Pseudomonas Gram-negativesome of the dressing material.organisms and anaerobe organisms8Systemic antimicrobial agents arecan cause a putrid smell from theindicated that will treat the causativeassociated tissue damage.organisms, and devitalized tissue shouldbe aggressively debrided in woundswith the ability to heal.Figure 5. Cont.to the bottom, that is, the characteristicsof STONES are found when bacteria aredeep within the chronic wound tissueor have penetrated the surrounding skin.Early recognition of infection is crucial sothat appropriate systemic treatment canbe started and further damage can beprevented.5. Obtain a bacterial swab in selected patients.The diagnosis of infection is made throughclinical assessment; however, the clinicianmay find the information gathered throughbacterial swab cultures helpful in makingtreatment-based decisions.The results ofthe swab culture may assist the clinicianin selecting antibiotic therapy and inruling out bacterial resistance.The use ofthe Levine method of rotating the swabover 1 cm2 of tissue while applying gentlepressure seems to be the best approachto obtaining a semiquantitative sample(Dow et al, 1999; Levine et al, 1976).After obtaining the swab, the clinicianshould follow the protocol for storage anddelivery of the swab to the laboratory.Diagnostically, the semiquantitativemethod for assessing burden is acceptablein most clinical settings (Dow et al, 1999;Levine et al, 1976). Systemic treatment3825-46NERDS 42WoundsUK,plans need to be reviewed once theresults of the swab culture are available.6. Select the appropriate topical treatment forsuperficial increased bacterial burden and benchmarkcriteria for monitoring respon
(Grayson et al, 1995). With infection of the surrounding or deeper structures, the wound often increases in size and satellite areas of breakdown may occur (Figure 4). At this stage, bacterial testing procedures may be useful. The gold standard for bacterial damage in a wound is the tissue biopsy for culture. More than 1.0 x 106