Transcription
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 801Review ArticleThe Method of Checking Medications Prior To Administration:An Evidence ReviewEfstratios Athanasakis, BSc, RNStaff Nurse, Royal Albert Edward Infirmary, Wrightington, Wigan and Leigh NHS Foundation Trust, Wigan,United KingdomCorrespondence: Efstratios Athanasakis, 6 Newton Close, WN1 2LH, Wigan, Lancashire, United Kingdom.E-mail: stratosathan@yahoo.co.uk.AbstractBackground: Checking medications before their administration by nurses is a basic preventive action formedication errors. Due to the fact that nurses perform medication checking in the everyday clinical practice,either on their own (single) or with another nurse (double) and are responsible for what they administer to thepatients, checking is directly related to nursing. Mostly the last years, queries around multiple issues aboutchecking have been raised.Aim: The present review was undertaken in order to collect and appraise research evidence about the method ofmedication checking (single and double) prior their administration.Methodology: A literature search was undertaken to PUBMED, SCIENCE-DIRECT, BRITISH NURSINGINDEX and CINAHL databases using specific keywords for relevant articles (of qualitative, quantitative, mixedmethodology) published in English from January 1990 to March 2015. For the introduction of an article to thereview, specific inclusion criteria were set. Additional data obtained through relevant reports from institutionsand the articles’ references. The selection process of the articles was based on the flowchart which wasrecommended in the PRISMA statement.Results: Twenty primary research studies and three reviews were included in the review and their data wasclustered according to the analysis of studies’ findings: definition inconsistency, single-checking, doublechecking, cases of checking application, benefits and drawbacks of checking, medication errors and promotingand supporting ways for checking method.Conclusions: The present review gathers current evidence about medication checking prior their administration,either single or double. Yet data is limited and ambiguous, implying the need for additional research in the field,so that the subject would be investigated in depth with safer and accurate conclusions.Keywords: nursing, medication preparation, medication administration, single checking, double checking,medication error.IntroductionThe procedures which are entailed in themanagement of patients’ medication comprisefields of clinical practice where the risk ofmedication errors is high (Schelbred and Nord,2007). The lack of checking habits is consideredto be one of the contributing factors formedication errors and specifically those relatedto staff. Importantly, the implementation ofdouble-checking method should be stressed atthe undergraduate level of iences.orgeducation (World Health Organization, 2011). Inorder to prevent medication errors’ occurrenceduring medication preparation and administrationa variety of specific methods and techniques isfollowed (Choo et al, 2010; Athanasakis, 2012).Towards to the direction of safety insurance andcare quality, the utmost measure that is adheredby nurses during medication administration is theappliance of the five rights: right patient, rightmedication, right dose, right route, right time,even though the last few years some researchers
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 802tend to consider as vital more rights than the fivementioned above (Wilson et al, 2004; Elliot andLiu, 2010). Alongside with the five rights goesthe measure of checking (single or double),which is used as a system-based strategy toaddress the combination of the health systemcomplexity and the human factor that lead toerrors. Strategies to prevent medication errors it’sbetter to be applied ‘concurrently with and neverin isolation of other strategies’ (Paparella, 2013,p. 632). The main objective of the abovemethods’ appliance is to follow every step of themedication procedure effectively and minimiseany potential harmful medication errors,particularly the medication administration errors.Double-checking was evidenced as a mode todiscover actual errors and near misses or preventserious medication errors (e.g. route medicationerror: preparation of intravenous (IV)metronidazole instead of oral) (Manias et al,2005; Sheu et al, 2009). In addition, medicationchecking was the third category of nurses’thinking during medication administration(Eisenhauer et al, 2007). Besides, the checkingmethod is directly related with nurses, since theyhold key-role in the medication procedures, thusit is possible to identify the error in time beforethe medication will be administered to the patient(Tran and Johnson, 2010).Guidelines of professional bodies and policiesThe British Nursing and Midwifery Council firstpublished in 1986 a medication administrationguideline. According to this, the second personshould be involved in the medicationadministration with a first-level practitionerwhen ‘that practitioner is instructing a learner orthe patients’ condition makes it necessary or insuch other circumstances as are logicallydetermined’. Also, it is recommended that thatthe second-level practitioner (i.e. the enrollednurse) should have undertaken medicationtraining and assessment in order to participate inthe medication administration process (Nursingand Midwifery Council-NMC, 1986).In 2010 in its report about safe medicinemanagement, stated that prior medicationadministration every registrant (registered nurse,midwife, specialist community public healthnurse) should check with another one atients’ allergies, inform patients and ask theirconsent, check the details of the prescription(substance, timing, strength, dose, frequency,route, date), check the way it is written (legible,clear, reasonable, authorized signature) andpatients’ identity (NMC, 2010).Another published medication safety alert,coming from Canada and published over adecade ago by the Institute for Safe MedicationPractices (ISMP Canada, 2003), discussing thevirtues of independent double checks. Since then,various publications came out by the sameinstitute and provided further insights to thesubject, by expanding the knowledge of theindependent double-checking definition, whilstproviding steps about its performance, byproviding examples of the clinical practice,relevant thoughts and nurses’ perspectives (ISMPCanada, 2005; 2009; ISMP USA, 2008).In the last concerning report of USA ISMP,independent double checks were characterized as‘undervalued’ and ‘misused’. However, it wassuggested that the method ‘can be part of avaluable defense’ for the medication , independent use, judiciouslyand has been standardized (ISMP USA, 2013).Beyond all these, the conduction of a cognitivereview of the prescription and the medicationpreparation by the professionals-checkers is afactor which is interfered in the double-checkingprocess (ISMP USA, 2014).Furthermore, an investigation of an effectivemethod for independent double-checking ofhigh-risk clinical procedures published by theCanadian Patient Safety Institute (CPSI). Thesurvey conducted at a post-anaesthetic care unitand a chemotherapy daycare centre in a teachinghospital in Toronto. The main conclusions of theinvestigation were the: acceptance of the methodby the staff, double-checking was performedeffectively, avoidance of certain types ofmedication errors (wrong drug in pump, wrongpatient, documentation mismatch between orderand label, clinically inappropriate orderprescribed for a patient), detection of medicationerrors after bedside patient identificationincluded as part of the independent doublechecking procedure and necessity of modified
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 803steps of double-checkings in different settings(Easty et al, 2008).Two recently published Canadian guidelines arereferring to the independent double-checkingmethod, as well (College and Association ofRegistered Nurses of Alberta, 2014; College ofNurses of Ontario, 2014). It mentioned that thechecking of medication should be independent,applied at high risk medications (insulin, heparin,chemotherapy), at each step (check prescription,perform calculations) and document all actions inpatients’ notes. In another chapter an alternatemeasure is proposed, that one of detecting thepatient separately by nurses (College andAssociation of Registered Nurses of Alberta,2014).The issue of double-checking of medications hasdrawn the attention of Australian Commission onSafety and Quality in Health Care (2013), byproviding evidence briefings supporting thatdouble-checking strategy can be performedselectively, independently; however, increasingnurses’ workload. In brief, across the world, themajority of the hospitals have establishedpolicies about medication administration to thepatients, including the steps of double-checking.Most of them can be found at the official pagesof the hospitals.Concepts’ clarificationChecking has been defined as the ‘verification ofthe correctness and appropriateness of acomponent of the medication administrationprocess’ (Eisenhauer et al, 2007). Singlechecking is a procedure of checking the steps ofmedication preparation by a single nurse.Whereas, double-checking or called otherwise asindependent double-checking concerns theprocedure of recheck/verification of themedication preparation steps, not from a singlebut from two nurses separately, before theadministration phase begins. It is of lessenimportance whether the first nurse is present ornot in the performance of the procedure from thesecond one, provided that the two particularcolleagues have not discuss about this subjectbefore the completion of the procedure (ISMPCanada, 2005; Australian Commission on Safetyand Quality in Health Care, The New South Wales Therapeutic AdvisoryGroup (NSW TAG) defined the independentdouble-checking precisely as ‘a procedure inwhich two individuals, preferably two registeredpractitioners, separately check each componentof the work process’. The Ministry of Health ofAustralia concretized the policy: ‘a secondperson should check the drug, dose, calculation,IV fluid, and the patient’s identity prior toadministration’ (Australian Commission onSafety and Quality in Health Care, 2013).Worth mentioning that the point of the checkingprocedure is that nurses are expected to findsimilarities in the information they manage. Incase that a nurse find different results, theresolving of the differences emerged should bedone before the medication would beadministered to the patient (ISMP Canada,2005). In a report by the CPSI in the context ofdouble-checking, researchers added one moresubcategory. If this is the case, the second nursewho applies the verification step is informedabout the data around the medical order(dependent double-checking) (Easty et al, 2008).AimThe present review was undertaken in order tocollect and appraise research evidence about themethod of medication checking (single anddouble) prior to their administration.MethodologyA literature search was undertaken to PUBMED,SCIENCE-DIRECT,BRITISHNURSINGINDEX and CINAHL databases for relevantarticles published in English from January 1990to March 2015, independently of the techniquesthe authors used to interpreted data (qualitative,quantitative, mixed). The following keywordswere used: ‘nursing’, ‘medication preparation’,‘medication administration’, ‘single checking’,‘double checking’. An additional key word:‘medication errors’ was added because of the factthat previous studies investigated potential corelation between any of the checking methodsand medication errors.The literature review included articles whichanalyzed single or double-checking as part of theinvestigation of other issues (e.g. medicationadministration process) or as the main subject
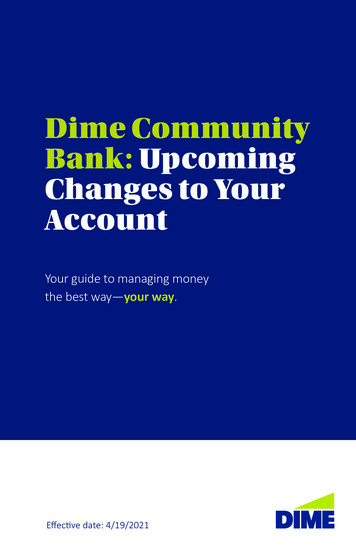
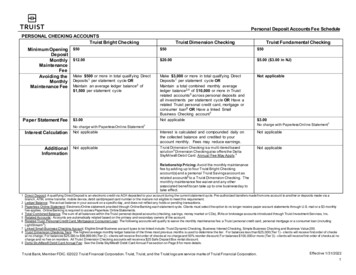
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 804(e.g. examine factors that foster and/or ions and organizations which discussedpatient safety and medication administrationsubjects have been taken into account to supportthe literature review.Another inclusion feature was that one of thesample, to be consisted entirely or partly ofregistered nurses. However, the literature searchrevealed that there were studies in which theirsample was based for example, on medicationerrors reports or medication administration cases.In this case, these studies were included providedthat they investigated the method of checking inrelation with the medication errors within thenursing context.Moreover, the references of the articles whichadhered the inclusion criteria were explored inorder to retrieve any potential new studies thatwere not retrieved in the first stage of the search.The majority of the detected articles weresuitable to enter the review in the stage of titleand abstract screening. In case of the existence ofarticles with no provision of their abstract, thentheir full-text has been ordered with the help oflibrarians and assessed. The selection process ofthe articles was based on the flowchart whichwas recommended in the PRISMA statement(Moher et al, 2009). The flow of articles’inclusion and exclusion in the literature review ispresented in Figure 1.Figure 1. Flowchart of literature search strategy.Studies found through the searchesin PUBMED (n 114), BNI (n 11),CINAHL (n 74) and SCIENCEDIRECT (n 129)Studies found through handsearch and references (n 6)Rejected at duplicate stage (n 68)-Articles for further screening (n 266)-Full text of articles screened for eligibility(n 126)Rejected at title and abstractstage (n 140) because examinedthemes concerned:reviews/other papers-not related(n 48)reference to pharmacy (n 21)reference to settings other thanhospital (n 23)checking method analyzed inother field than medication one(n 48)Rejected after checking: becausegave a report to single/doublechecking and not analyzed (n 103)Total number of primary research studies that included (n 20) and review papers (n 3)www.internationaljournalofcaringsciences.org
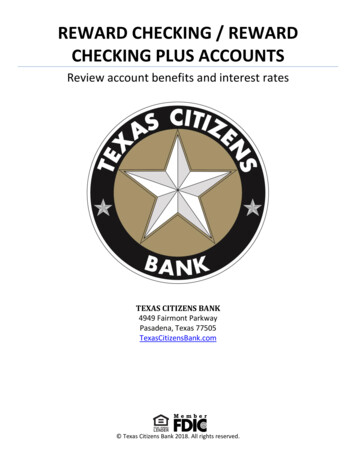
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 805Table 1. Summary of key features of the research articles that were included in the present review.Authors,year andcountryWinson(1991)UKKruse et al.(1992)AustraliaRoss et al.(2000)UKJarman etal. (2002)AustraliaManias etal. (2005)AustraliaObjectiveMethodologyMajor findingsTo examine nurses’ attitudestowards single MA.N 328 RNs and ENs from 6 specialitiesfrom 2 hospitals in one district healthauthority. Use of questionnaire (8 structuredquestions with qualitative data).The majority of nurses consideredthemselves as able to administermedications alone. After the research, theMA policy received clarifications.319 MEs found for 129.234 MA cases.ME rate when MA was done by a singlenurse was: 2.98 (95% CI: 2.45-3.51) and2.12 (95% CI: 1.69-2.55) by 2 nurses per1000 MA cases.Additional nursing time of 17.1 h/1000MA cases, when MA was done by 2 RNs.Statistically significant (29%) reduction inerrors. Unclear advantages of doublechecking.195 MEs/5 years.Nurses were responsible for 59% of theMEs. The most common ME concernedthe IV route (56%) and the most commondrug involved were antibiotics (44%).Double-checking policy for allmedications by pharmacy decreased MEsfrom 9.8 to 6 MEs/year. Change to lesspunitive reporting of MEs resulted in theirincreased reporting rate.The application of a checking ofmedications by one nurse considered to besafe and contributed to the saving of timeand enhances their responsibility. Duringthe period of study 4 MA errors werereported, while the same period of theprevious year happened 5 MA errors.To assess the implicationand the cost of using 2nurses administering nonrestricted medications.To determine the incidenceand type of ME andascertain whether any MEprevention programmes hadinfluenced their prevention.The evaluation of the levelof nurses’ awareness of theirresponsibility following theintroduction of singlechecking of medications,their level of confidence intheir checking technique andtheir level of satisfactionwith the change.The assessment of the use ofa MA protocol by graduatenurses in their medicationmanagement activities.Cross-over study.46 weeks study period.3 wards of geriatric and rehabilitation unit ofa hospital.Retrospective study of MEs documented fora 5 years period.Paediatric wards of a teaching hospital.Review of MEs reports.Qualitative study, descriptive design.Use of a questionnaire and record ofmedication incident records.Implementation of a single-person checkingprotocol for 7 months.N 129 RNs who were working in multipleclinics of a hospital.Descriptive prospective qualitative study.Use of in depth interviews, observationsduring MA and information from medicationprotocols.N 12 recently graduate nurses who wereworking in multiple clinics of a universityhospital.For data analysis qualitative and quantitativetechniques were he MA protocol included the doublechecking. Nurses adhered to protocols ifthey perceived not to impede with othernursing activities. 97% of the sampledouble-checked the preparation ofdesignated medications in 97% ofsituations, while they double-checkedmedications to the patient’s bedside in
International Journal of Caring SciencesGosbee(2006)CanadaHospodar(2007)USAConroy etal. (2007)UKO'Connell etal. (2007)AustraliaArmitage(2008)UKDavis et al.(2010)AustraliaDickinson etal. (2010)NewZealandTo compare theeffectiveness of 2 methodsof independent doublechecking.To imply a creative timesaving project of improvingdocumentation compliancefor double-checking insulinadministration.To identify MEs occurringand develop methods toreduce their recurrence risk.To examine nurses’perceptions towards thesingle-checking ofmedications, before and afterits application.The research of the doublechecking procedure ofmedications using data fromanother larger studyconcerned MEs etiology andtheir report.The evaluation of theimportance of contextualand policy factors on nurses’judgment about MApractice.To assess nurses’understanding and thepractice of double-checkingof medications, the factorsthat foster and impede theSeptember-December 2015 Volume 8 Issue 3 Page 806Usability test. Use of 2 methods to performdouble-checking: a flow sheet and the verbalread-back method.N 2 teams of 4 nurses. Checking of 12 PCApump set-ups against 12 order forms, usingeach method for 6 checking times.80% of situations.Both methods were effective. The MEdetection rate was 88%.Participated nurses from 2 inpatients nursingunits in a 50-bed rehabilitation center. Useof posters and staff education. Recording ofinsulin administration times.Pre-intervention: 187 administrations ofinsulin/65 double checks.Post-intervention: 230 administrations ofinsulin/167 double checks.Increase of the double checkingcompliance from 35 to 72% .Observational study which lasted over 6weeks in a children’s’ hospital.139 prescription and MA in 253 patientswere checked. Over than 60 drugadministration rounds.63 interruptions were recorded.9 actual errors and 141 violations ofprocedure. Failure to follow doublechecking in 16% of the patients it was notperforming.After the implementation of singlechecking nurses’ confidence (43%),accountability (44%), and drug awareness(33%) have been increased. 22% of nurses‘did not feel confident to their skills tocheck drugs independently’.Overall, nurses’ perspectives aboutmedication single-checking becamepositive, after their training relevant withthe application of this method.Double-checking procedure should beapplied selectively, when there is plenty oftime and when the staff can comprehendthe procedure.4 themes emerged: deference to authority,reduction of responsibility, automaticprocessing and lack of time.Intervention study (prior and after theimplementation of single-checkingprocedure). Two questionnaires used in twoseparated phases, approximately 18 months.N 124 nurses prior and n 122 after theimplementation of this method, who wereworking in multiple clinics of a hospital with16 years of experience on average. Dataanalyzed descriptively.Mixed methodology.Study of 991 reports of MEs and 40 in depthinterviews with health professionals from auniversity hospital.Quantitative study. Questionnaire survey.Applied a number (6) of factorial vignettes.N 185 nurses, who were working inmultiple clinics of a tertiary pediatrichospital (medical, emergency, surgical,intensive care) with 6 years of experience.Descriptive qualitative study.N 19 nurses who were working in wards ofa pediatric hospital.Data collected via 3 focus groups andthematic analysis was used for their orgThe double check of patients’ identity, themedication and the verification of medicalorder were the factors that affect nurses’actions during MA.The independent double-checking wasdeemed as a practice particularly essentialin pediatric clinics. There were factors thataffected its implementation during MA.
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 807application of independentdouble-checking.White et al.(2010)CanadaPopescu etal. (2011)AustraliaConroy etal. (2012)UKGill et al.(2012)AustraliaVan Veen(2012)CanadaO’Connellet al.(2013)AustraliaAlsulami etal. (2014)UKTo determine the elementsof a list which contributed tothe effective detection ofMEs.To explore the multifactorialinfluences on medicationquality and safety in thecontext of single-checkingpolicy for MA acute care.To establish what policiesthere are in the UKchildren’s units of checkingmedications and to discussevidence on the differentprocesses in use.The study of nurses’compliance with theadherence of a MA protocoland the reasons of noncompliance with it.To implement independentdouble-checking in 2different methods.To examine the reliabilityand validity of the SCAMS.To evaluate how closelydouble-checking policies arefollowed by nurses inpaediatric areas and also toidentify the types, frequencyand rates of MA errors thatoccur despite the double-High fidelity simulation study.N 13 nurses, who were working inoutpatient chemotherapy clinics.Exploratory/descriptive study.Non participant observations.Follow-up semi-structured interviews.N 11 RNs.30 medication episodes observed in amedical and surgical ward in a tertiaryreferral centre. Use of thematic and contentanalysis.Survey of 105 questionnaires from 59 NHSTrusts with 69 hospitals.N 41 pharmacists and n 26 nurses fromneonatal and children’s units.Mixed methodology design.N 72 RNs who answered the questionnaireand n 24 RNs that participated in focusgroups, who were working in a NICU in atertiary pediatric hospital.Pilot study in an outpatient oncology unitwith oncology nurses as participants. 1stmethod of double checking: the resourcenurse applied it for all chemotherapymedications, 2nd method: each nurse wasresponsible to performed it upon request.Secondary analysis of data retrieved fromlongitudinal questionnaire on nurses’attitudes to single check MA by using a 13item SCAMS.N 503 nurses with 5 years of experiencefrom 38 wards of a large healthcare centre.Exploratory and confirmatory factoranalysis.Prospective, direct and undisguisedobservational study.Pediatric nurses had been observed for 4months for the double-checking process forn 2000 MA cases at PICU, NICU, medicaland surgical paediatric inpatients, totaln e explicit determination of the steps of anursing intervention is a preventivemeasure for specific error types, whennurses are required to perform a longseries of mechanistic tasks under a highcognitive load.MA safety and quality were influenced bythe therapeutic relationship, ward designand deviation from best practiceguidelines.During medication rounds nursesexperienced fewer interruptions and theiroverall duration was decreased.A role for single and double-checkingdepends on risk assessment. Doublechecking was performed for certainmedications.Differences were found between the levelof nurses’ experience and their compliancewith the protocol adherence. Nurses’ noncompliance with the medication protocolobserved more in the checking of patients’identity and the medications’ doublechecking.Nurses were concerned about certain areasof the effectiveness of checkingimplementation. The 2nd method seemed tobe more suitable. Modifications in patientsflow and in the nursing schedule havedone.Authors recommended SCAMS as a validand reliable tool before and after theimplementation of single-checking policy.The lowest (30%) double-check adherencerate concerned the ‘dose calculation’ step.A statistically significant difference foundfor double-checking medications in ninesteps during weekends rather thanweekdays. The MA error rate was 9.6% of
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 808checking process.the total MA cases, with the most of thecases the MA by parents while the nursewas absent.Three limitations mentioned: studyconducted in a single hospital, possibleeffect of the observer at nurses’performance and not all singleadministrations observed.Cross-sectional and descriptive design.Bülbül et al. To determine the levels ofInterruption/distraction rate acetoface(2014)medication preparation was 92.9%.and MA errors of nurses.interview.TurkeyChecking adherence of high riskN 98 nurses from paediatric wards:medications by 2 nurses was 64.3%. 5 years 71% and 5 years 27% of theUndergraduate nurses were more able tonurses.calculate paediatric doses.Common errors: lack of calculation of setportion and errors related medicationconcentrations and dosage.MA: Medication Administration, RN: Registered Nurse, EN: Enrolled Nurse, ME: Medication Error, PCA:Patient-Controlled Analgesia, SCAMS: Single Checking Administration of Medication Scale, PICU: PediatricIntensive Care Unit, NICU: Neonatal Intensive Care Unit.Table 2. Summary of key features of the non research papers (systematic/literature/policy review)that were included in the present review.Authors, yearand countryAlsulami et al.(2012)UKAustralianCommission onSafety andQuality inHealth Care(2013)AustraliaKellett &Gottwald(2015)UKObjectiveTo evaluate the evidence fordouble-checking theadministration of medicines.MethodologyMajor findingsLiterature search at 6 databases.3 quantitative, 2 mixed methods,9 qualitative methods, 2systematic reviews were included.There were major practical difficultiesin double-checking.Need for further research and scientificevaluation of the double-checkingmethod was expressed.Double-checking was correlated withincreased workload for nurses.Not enough evidence about theeffectiveness of double-checking, butcarried it out in certain situations.Literature search at 5 databases.17 studies included.Does double-checking bynurses reduce medicationadministration errors andimprove safety?To provide evidence aboutdouble-checking high-riskmedications and supportnurse managers to theirdecision making on safemedication administrationpractice in clinical settings.Critical literature review whichwas undertaken as part of an MSc.11 primary research ciences.orga) Evidence for double-checking,b) processes to support doublechecking,c) human factors affect doublechecking.
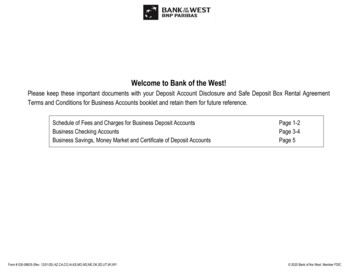
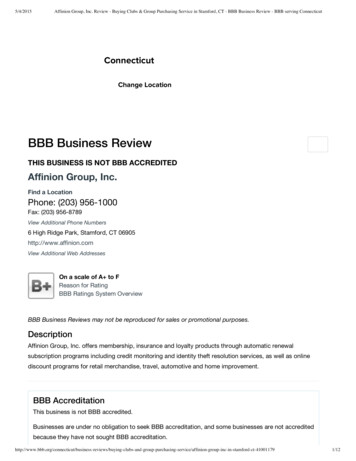
International Journal of Caring SciencesSeptember-December 2015 Volume 8 Issue 3 Page 809FindingsThe total number of retrieved studies from theliterature search was 23. Specifically, 20 primaryresearch articles and 3 review articles (includingone systematic review) were detected. The keyfeatures of the research articles are presented inTable 1 and that of the reviews in Table 2. stage B: calculation of medication dosology(independently-each nurse separately orsimultaneously-doing the calculation togetheror the second nurse observes the first whiledoing the calculation or the first nurse showsthe calculation result and the other checks if itright or not),From the total number of articles, the method ofchecking during medication preparation and/oradministration was investigated as the mainresearch topic in thirteen articles: singlechecking was explored in five studies (Winson etal, 1991; Jarman et al, 2002; O’ Connell et al,2007; Popescu et al, 2011; O’Connell et al,2013), double-checking in seven (Gosbee, 2006;Hospodar et al, 2007; Armitage, 2008; Dickinsonet al, 2010; Van Veen, 2012; Alsulami et al,2014; Kellett and Gottwald, 2015) and checking(in general) in one (Conroy et al, 2012). Whilst,in the rest research studies the checking methodwas analyzed in the context of another basictheme e.g. nurses’ compliance with theimplementation of a medication administrationprotocol (Manias et al, 2005). stage C: medication preparation (medicationis prepared by both nurses or by a singlenurse whose actions are observed from thesecond one),The findings of the present review were clusteredin the follow categories: definition inconsistency,single-checking, double-checking, cases ofchecking application, benefits and drawbacks ofchecking, medication errors and promoting andsupporting ways for checking method.Another crucial aspect of the double-checking isthat one which concerned the professionals whowere involved in it. Manias et al. (2005)supported that ‘double-checking involved theprocess of having two nurses ding to the hospital pro
Checking has been defined as the 'verification of the correctness and appropriateness of a component of the medication administration process' (Eisenhauer et al, 2007). Single-checking is a procedure of checking the steps of medication preparation by a single nurse. Whereas, double-checking or called otherwise as