Transcription
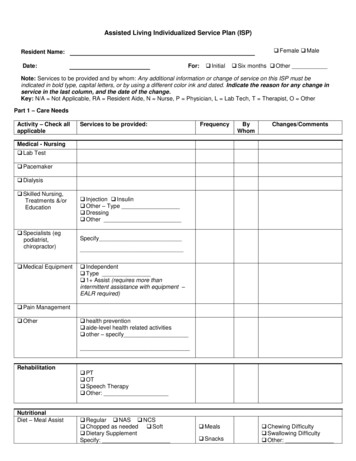
Assisted Living Individualized Service Plan (ISP) Female MaleResident Name:Date:For: Initial Six months OtherNote: Services to be provided and by whom: Any additional information or change of service on this ISP must beindicated in bold type, capital letters, or by using a different color ink and dated. Indicate the reason for any change inservice in the last column, and the date of the change.Key: N/A Not Applicable, RA Resident Aide, N Nurse, P Physician, L Lab Tech, T Therapist, O OtherPart 1 – Care NeedsActivity – Check allapplicableServices to be provided:FrequencyByWhomChanges/CommentsMedical - Nursing Lab Test Pacemaker Dialysis Skilled Nursing,Treatments &/orEducation Specialists (egpodiatrist,chiropractor) Medical Equipment Injection Insulin Other – Type Dressing OtherSpecify Independent Type 1 Assist (requires more thanintermittent assistance with equipment –EALR required) Pain Management Other health prevention aide-level health related activities other – specifyRehabilitationNutritionalDiet – Meal Assist PT OT Speech Therapy Other: Regular NAS NCS Chopped as needed Soft Dietary SupplementSpecify: Meals Snacks Chewing Difficulty Swallowing Difficulty Other:
Resident Name:Activity – Check allapplicableServices to be provided:Fluid Restrictions/Encouragement None Dietary Supplements Other Specify:FunctionalPersonal HygieneContinence Independent Shower Bath Equipment Hearing Aide: R L Eyeglasses Reading AlwaysHair: Shampoo Grooming Shave Teeth Care Denture Care Nail Care Foot Care Independent Assist with bathroom Assist with protective garment change Ostomy Care Chronic unmanaged incontinence(chronically unwilling or unable toparticipate, with help from staff, so thatcleanliness and sanitation can bemaintained - EALR required)Skin Care None Location & Type:Dressing Independent Coordinate Upper Lower OtherMedications Self AssistTransfer Independent 1 Assist (chronically chairfast and/orchronically needs one person assist totransfer – EALR required)Mobility Independent Walker Cane Wheelchair Crutches Escort: 1 Assist (chronically needs one personto assist to walk or to climb/descend stairsEALR required) No Known History Other:Falls Risk ReductionRespiratory Therapy& Oxygen None Self-managed Type:Equipment None Self-managed Prosthesis Braces OtherDate:FrequencyByWhomISP Page 2 of 5Changes/Comments
Resident Name:Activity – Check allapplicableCognitiveOrientationSpecialized ServicesServices to be provided: N/A Remind Cue Supervise Accompany N/A Dementia Care, Secured Unit (requiresSNALR) Environmental modifications Supervision/MonitoringSensory None Hearing Vision Speech Other:Mental Health Diagnosis: Treatment Required Yes No Substance Abuse Coordination with SAproviderSocialEducation &EmploymentDesire for continued or future education: Yes NoIf yes, specify:Desire to work or volunteer Yes NoIf yes, specify:IntellectualDesire for new or continued intellectualactivity Yes NoIf yes, specify:RecreationalDesire for new or continued recreationalactivity No Yes, Specify: Need assistance of ALR staffSpecify:SpiritualDesire for new or continued spiritual activity No Yes, Specify: Need assistance of ALR staffSpecify:CulturalDesire for new or continued cultural activity No Yes, Specify: Need assistance of ALR staffSpecify:FinancialAssistance with access to financial benfits(i.e. Medicare, Medicaid, Social Security,Veteran’s Admin., Pensions, etc.) Managed Independently Assistance of family, resident rep. orlegal rep. Specify: Need assistance of ALR staffSpecify:Date:FrequencyByWhomISP Page 3 of 5Changes/Comments
Resident Name:Date:ISP Page 4 of 5OtherComments:Print Name, Title and Organization of Individuals ParticipatingResidentResident’s RepresentativeResident’s Legal Representative (if applicable)ALR Provider’s RepresentativeWas the Resident’s Primary Physician Consulted? YesIndicate physician’s name and date: NoHome Care Services Agency Rep. Signature(if applicable)ALR Provider’s Representative SignatureDateDocumentation of ISP Review: For 6-month ISP reviews please consider and review any changes in the followingareas: Communication/Dental/Vision/Hearing; Customary Routine, Continence Status/Management, Physical Function,Cognitive Impairment Screen, and Admission Decision. I am confirming the ISP services as listed above, including any changes that have been made since the last review. I have reviewed the ISP services as listed above and recommend the following change(s) in service:NameTitleDateSignatureDocumentation of ISP Review: For 6-month ISP reviews please consider and review any changes in the followingareas: Communication/Dental/Vision/Hearing; Customary Routine, Continence Status/Management, Physical Function,Cognitive Impairment Screen, and Admission Decision. I am confirming the ISP services as listed above, including any changes that have been made since the last review. I have reviewed the ISP services as listed above and recommend the following change(s) in service:NameTitleDateSignatureAttach Documentation of additional ISP Reviews as Necessary
Resident Name:Date:ISP Page 5 of 5Assisted Living Individualized Service PlanAddendum for Enriched Housing Program/Assisted Living Residences(If applicable)Note: Services to be provided and by whom: Any additional information or change of service on this ISP must beindicated in bold type, capital letters, or by using a different color ink and dated. Indicate the reason for any change inservice in the last column, and the date of the change.Key: N/A Not Applicable, RA Resident Aide, N Nurse, P Physician, L Lab Tech, T Therapist, O OtherThe following information pertains to additional tasks not included on the ISP relating to the enriched housingprogram functional assessmentActivityInstrumentalActivities of DailyLiving TransportationServices to be provided: independent, drives own car or accessestransportation on own & chooses to do so wants or needs someone to drive them,but does not require an escort must be accompanied by an escort requires special transportationspecify Laundry is able & chooses to do own laundry is able & chooses to do light laundry, butwants/needs assistance with heavy laundry needs or chooses ALR to do all laundry Housekeeping is able & chooses to do all housekeepingtasks in room/apartment is able & chooses to do lighthousekeeping, but wants/needs assistancewith heavier cleaning tasksSpecify needs or chooses ALR to do allhousekeeping is able & chooses to shop on their own &carry or transport packages on their own is able & chooses to do light shopping ontheir own, but wants/needs assistance withmajor shoppingSpecify needs or chooses ALR staff or otherperson (i.e. family member) to do all of theirshopping Independent-has phone & dials numbersand answers calls without assistance has specially adapted phone and dialsnumbers and answers calls withoutassistance chooses or needs ALR staff to help themmake calls or make the calls on their behalf Shopping Ability to usetelephoneFrequencyByWhomChanges/Comments
Assisted Living Individualized Service Plan (ISP) Resident Name: Female Male Date: For: Initial Six months Other _ Note: Services to be provided and by whom: Any additional information or change of service on this ISP must be indicated in bold type, capital letters, or by using a different color ink and dated.