Transcription
Delivery System Design: MentalHealth, Substance AbuseTreatment, DevelopmentalDisabilities ServicesMedicaid Pathway to an Integrated Health Care SystemWork Group Discussion April 21st 2016Funding for this report was provided by the State of Vermont, Vermont Health Care Innovation Project, underVermont's State Innovation Model (SIM) grant, awarded by the Center for Medicare and Medicaid Services (CMS)Innovation Center (CFDA Number 93.624) Federal Grant #1G1CMS331181-03-01.
Discussion Topics & Goals Project Update Objective for Reform Planning Objective for Delivery System Design Delivery System Design Next Steps2
Project Update Status of Model Design: Objective Scope of Services Delivery System Payment/Cost Modeling Funding/Savings Opportunities State Operations Communications Participants and Advocates Providers State Staff3
Objective for Reform PlanningDevelop an organized delivery system for serving individualswith mental health, substance abuse treatment anddevelopmental service needs and promote integration of: Mental Health Substance Abuse Treatment Long-Term Services and Supports for individuals withdevelopmental service needs Physical Health Long-Term Services and Supports for individuals withphysical disabilities and older Vermonters4
Delivery System Design ObjectivesA delivery system design and governance structure thatsupports the following: Adoption of Vermont’s Integrated Model of Care,including advancement of primary care andprevention Service Delivery Reform, including population-basedhealth and prevention and development of bestpractices Quality Framework Payment Reform, including value based purchasing Efficient Operations and Oversight Medicaid’s Pathway for Alignment with the All-PayerModel5
Discussion of Broad Design OptionsCoordination ModelObjectiveAdoption of theVermont IntegratedModel of Care(Person-Centered Care,Integrated ServiceDelivery,Interdisciplinary CareTeam, Single CaseManager, InformationSharing)Service DeliveryReform(Population-BasedHealth, Adoption ofBest Practices)How Model SupportsObjectiveOpportunities/Challenges Each provider willhave coordinationagreements withother providers aswell as ACO Numerous processeswill need to bedeveloped to supportModel of Care Unclear how todeploy resources forinformation sharing Some servicesprovided by DAs, SSAsand PreferredProviders overlapbetween draft scopeand ACO scope Will requiregovernance/decisionstructure forassignment of casemanager Potential duplicationof processes andfunctions Unclear howinformation sharingwill be advanced Some paymentmodels could provideadditional flexibility Continues existingroles for providers;unclear howIntegration ModelHow Model SupportsObjectiveOpportunities/Challenges Governance structurewould provideoperational supportfor achieving theModel of Care Care planning andservice coordinationsupports could bestreamlined Requires additionaladministrative layerthat would be lessefficient to the extentthe same functionscontinue at theprovider level Requires coordinationand consensus at theprovider levelregardinggovernance/operations Coordination andaccountability at thecommunity levelpromotes innovation Opportunity todemonstrate savingsfor traditionalservices Requires coordinationand consensus at theprovider levelregardinggovernance/operations Risk/liability concerns6
Discussion of Broad Design OptionsCoordination ModelObjectiveQualityFrameworkPayment ReformHow Model SupportsObjectiveOpportunities/Challenges State andstakeholders coulddevelop qualityframework Payment modelsbased on eachprovider’s existingserviceresponsibilities Does not supportpayment reform forfull scope of services Unclear how paymentmodels can supportintegration orincentives based onbroad qualitymeasures Most DA/SSA servicesalready based on caserates Avoids conflict amongproviders regardingresource allocation Could consolidateexisting fundingstreamsIntegration ModelHow Model SupportsObjectiveOpportunities/Challenges State andstakeholders coulddevelop qualityframework Quality reportingcould be centralized Model may promotecommunity-basedquality model Opportunity todevelop incentivesbased on broadquality objectives Opportunity to directresources inaccordance withquality objectives Payment modelsbased on draft scopeof services Greater flexibilityregarding allocationdecisions atcommunity level Requires structure tosupport decisions atthe community level Opportunity tocoordinate with APM Agreement onfunding decisionswould be challengingand may impedeother coordinationefforts7
Discussion of Broad Design OptionsCoordination ModelObjectiveEfficientOperations andOversightAlignment withAll Payer ModelHow Model SupportsObjective Additional resourcesand coordinationactivities to achieveModel of Care Adoption ofVermont’s IntegratedModel of Care willproducedemonstrablebenefits andopportunities forcoordination withAPMOpportunities/Challenges Preserves existingfunctions at bothstate and providerlevel Providersindependentlycoordinate withAPM contractorsand serviceprovidersIntegration ModelHow Model SupportObjectiveOpportunities/ Challenges Consolidation offunctions atprovider and statelevel Administrative functionscould be duplicated acrossproviders and newentity/Fiscal Agent Significant implementationinvestment State oversight could bestreamlined to extentcommunity adopts robustquality framework Oversight and reportingdue to grant requirementswould continue Could provide asingle interface withAPM Creates accountablemodel that alignswith APM reformefforts Enhanced opportunity todemonstrate traditionalcare savings and developinvestment agreements Creates single entity withineach region (or statewide)accountable for Vermont’sIntegrated Model of Careand responsible forcontracting, coordinatingand supporting APM Streamlines opportunity todevelop care coordinationplatform across all services8
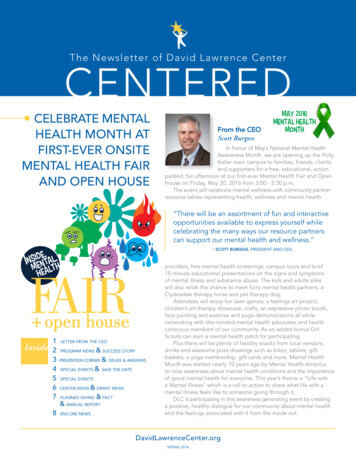
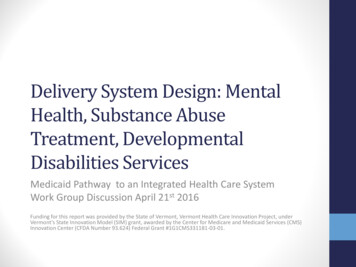
Delivery System Design:Service Coordination ModelDAAHS andDepartmentsCurrently multipledepartments; State oversightand funding potentially couldbe streamlinedHome HealthAgencyPreferred ProviderUnclear whether providerswould coordinate with APMindividually or collectivelyAll-Payer ModelAlignmentCoordinationAgreements Care planningCase manager assignmentData sharingQuality monitoringSimilar to some current provider arrangements Care coordinationData sharingLinkage to primary careTransition planningDevelopment of community needs assessmentsIncentive arrangements9
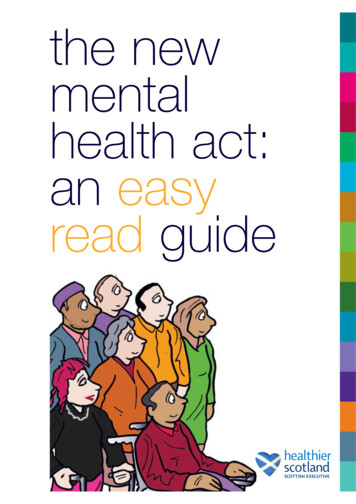
Delivery System Design:Integration ModelAHS andDepartmentsGovernanceConsolidatedfunding andoversightDADAOrganizationHome HealthAgencyPreferredProviderPaymentHome HealthAgency(Regional orStatewide) AllocationsFiscal iderAll-PayerModelAlignmentSimilar to the VCRYP, IFS and CIS Delivery ModelsCare coordinationData sharingLinkage to primary careTransition planningDevelopment of community needsassessments Incentive arrangements 10
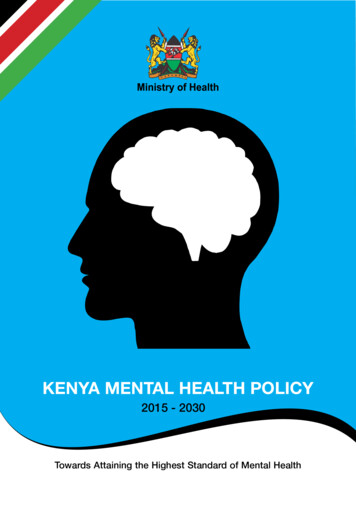
Delivery System Design: Partial IntegrationAHS andDepartments DAPaymentContractingOversightCurrently multiple departments;State oversight and fundingpotentially could be streamlined Home HealthAgencyQuality MonitoringIncentivesPopulation Health InvestmentsPreferredProviderOrganization(Regional orStatewide)All-PayerModelAlignment Quality ReportingData/SoftwarePopulation Health InitiativesGovernanceProcess DevelopmentCare coordinationData sharingLinkage to primary careTransition planningDevelopment of community needsassessments Incentive arrangements 11
Discussion of Structural Design What model best supports reform objectives and is feasiblefor both providers and the State? Does the model provide flexibility regarding how it isimplemented within each community as well as thetimeline for implementation?12
Next Steps Finalize Draft Delivery System Design (AprilJune) Evaluate Payment Reform Options (May/June) Revisit delivery system design and scope,as needed Develop Quality Framework (May/June) Evaluate Infrastructure and FundingRequirements (June/July) Obtain Stakeholder Feedback (Ongoing) Finalize Delivery System and PaymentReform Model (June/July) Identify Key Milestones and ImplementationTimeline (July) Develop Detailed Model Design andImplementation Plan ortunitiesfor SavingsScope andOversight13
Delivery System Design Objectives. 5. A delivery system design and governance structure that supports the following: Adoption of Vermont's Integrated Model of Care, including advancement of primary care and prevention Service Delivery Reform, including population -based health and prevention and development of best practices Quality Framework