Transcription
Value-Based Health Care Deliveryand the Role of Outcome MeasurementProfessor Michael E. PorterWorking Party on Health Care Quality and Outcomes (HCQO)OECD Conference CenterParis, FranceThursday, May 17, 2018This presentation draws heavily on Professor Porter’s research in health care delivery including Redefining Health Care (with Elizabeth Teisberg), What is Value in Health Care, NEJM, and The Strategy That Will Fix Health Care, HBR (with Thomas Lee).A fuller bibliography is attached. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means — electronic, mechanical, photocopying, recording, or otherwise — without the permission of MichaelE. Porter. For further background and references on value-based health care, see the website of the Institute for Strategy and Competitiveness.
Incremental “Solutions” Have Had Limited Impact Evidence-based medicine Safety/eliminating errors Prior authorization for expensive services Patients as paying customers Electronic medical records Introducing “lean” process improvements Care coordinators Retail clinics/urgent care Programs to address generic high cost areas(e.g. readmissions, post acute) Mergers and consolidation Restructuring health care delivery is needed,not incremental improvements2Copyright 2018 Professor Michael E. Porter
Value-Based Health Care is Rapidly DiffusingPeer Reviewed Literature 1990-2017140020171200JournalArticlesRelatedTo 990199520002005201020152020YearFrom: Science Direct; accessed October 2016, Patrick Clapp, Baker Research Services and Meredith Alger, Institute for Strategy andCompetiveness, Harvard Business School3Copyright 2018 Professor Michael E. Porter
Solving the Health Care Problem The fundamental goal and purpose of health care is toimprove value for patientsValue Health outcomes that matter to patientsCosts of delivering these outcomes Delivering high value health care is the definition ofsuccess Value is the only goal that can unite the interests of allsystem participants Improving value is the only real solution The question is how to design a health care delivery systemthat substantially improves patient value4Copyright 2018 Professor Michael E. Porter
Principles of Value-Based Health Care Delivery Value cannot be understood at the level of a hospital, a care site,a specialty, an intervention, a primary care practice or a broadpopulation Value is created in caring for a patient’s medical condition (acute,chronic) over the full cycle of careValue The set of outcomes that matter for the conditionThe total costs of delivering these outcomes over the full care cycle In primary and preventive care, value is created in servingsegments of patients with similar primary and preventive needs The most powerful single lever for reducing cost and improvingvalue is improving outcomes5Copyright 2018 Professor Michael E. Porter
Creating Value-Based Health Care DeliveryThe Strategic Agenda1. Re-organize care around patient conditions, into integratedpractice units (IPUs) For primary and preventive care, IPUs serve distinct patientsegments2. Measure outcomes and costs for every patient3. Move to value-based reimbursement models, and ultimatelybundled payments for conditions and primary care segments4. Integrate multi-site care delivery systems5. Expand or affiliate across geography to reinforce excellence6. Build an enabling information technology platform6Copyright 2018 Professor Michael E. Porter
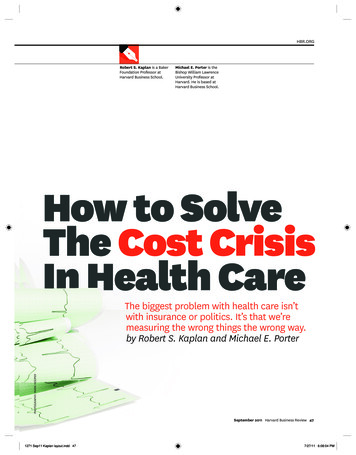
Re-organize Care Around Patient Medical ConditionsHeadache Care in GermanyOrganize by Specialtyand Discrete ServiceIntegrated Practice Unitfor the ConditionAffiliatedImaging reatmentand DetoxUnitsPrimaryCarePhysiciansWest GermanHeadache CenterNeurologistsPsychologistsPhysical Therapists“Day ed “Network”NeurologistsOutpatientPsychologists IPUs include care for common comorbidities and complicationsSource: Porter, Michael E., Clemens Guth, and Elisa Dannemiller, The West German Headache Center: IntegratedMigraine Care, Harvard Business School Case 9-707-559, September 13, 20077Copyright 2018 Professor Michael E. Porter
The Emerging Playbook for Integrated Practice Units (IPUs)1.Organized around a medical condition, or group ofclosely related conditions. And defined patient segments for primary care2.Care is delivered by a dedicated, multidisciplinary teamdevoting a significant portion of their time to the condition In-house staff as well as affiliated staff with strong working relationships3.͏Co-located in dedicated facilities. Hub and spoke structure coveringmultiple or affiliated sites, and incorporating telemedicine where appropriate4.Takes responsibility for the full cycle of care5.͏ atient education, engagement, adherence, follow-up, and preventionPare integrated into the care process6.The unit has a clear clinical leader, a common scheduling and intakeprocess, and unified financial structure (single P L)7.A physician team captain, clinical care manager or bothoversees each patient’s care8.The IPU routinely measures outcomes, costs, care processes,and patient experience using a common platform9.The team accepts joint accountability for outcomes and costs10. The team regularly meets formally and informally to discuss individual10.patient care plans, process improvement, and how to improve results8Copyright 2018 Professor Michael E. Porter
The Journey to Value Based Primary Care1. Segment the population based on primary care needs2. Develop primary care teams around patientsegments (IPUs)3. Create shared infrastructure across primary careIPUs to increase efficiency and enhance value4. Measure outcomes and costs by segment5. Integrate primary care and with specialty care6. Move toward value based payments by segment‒ Risk adjustment will differ by segment9Copyright 2018 Professor Michael E. Porter
Shared Primary Care InfrastructurePrimary Care Practices (Population Segmented)Sites for Low Cost,ConvenientRoutine ServicesAfter Hours Access Clinics in retailstores or otherconvenient, lowcost sites After hours clinicsin primary care oroutpatientspecialty sites Shared walk-inclinics in primarycare or specialtycare sites 24 hour nursehotlinesPrevention HubsSupport ServicesReflecting Socialand BehavioralEffects on Health Smokingcessation Housing Alcohol addiction Nutrition support Weight loss Domestic violence Other complexaddiction (e.g.opioids) Transportation Income support Close contact withsocial servicesorganizations10Copyright 2018 Professor Michael E. Porter
Integrating Primary With Specialty Care to Improve ValueSpecialty IPUsEmbeddedspecialists inareas prevalentin thepopulationSpecialistrotation ocols andtraining to shiftappropriatecare to lowercost settingsPCC teamrelationships withaffiliatedspecialists ts toefficientlyaccessspecialistsPrimary careembedded inspecialty IPUsfor complexconditionsPrimary Care Practices (Population Segmented)11Copyright 2018 Professor Michael E. Porter
Value-Based Primary CareOak Street Health Focuses low-income older adults living in under-served urbancommunities– Four severity tiers Multidisciplinary team covering the full care cycle: physicians, PAs,NPs, RNs, medical assistants, scribes, care managers, socialworkers, clinical informatics specialists, and others Co-located in dedicated facilities. 19 sites across the Midwest Explicit processes to engage patients and reduce obstaclesto accessing care such as free rides/home-visits, in-housepharmacy and selected events for community residents Selected in-house specialty services such as behavioral health andpodiatry. Close relationships with preferred outside specialistsand imaging partners Meet daily and weekly to discuss patient care plans and processimprovement Measure and accountable for outcomes, cost, and patientexperience Single risk-adjusted payment covering overall care– Includes specialty and post-acute care12Copyright 2018 Professor Michael E. Porter
Measure Outcomes for Every PatientThe Quality Measurement LandscapePatientExperience/Engagement/ AdherencePatient InitialConditions,Risk omesE.g., PSA, surgicalmarginStructureE.g., Staffcertification,facilities standards13Copyright 2018 Professor Michael E. Porter
Measure Cost for Every PatientPrinciples Properly measuring the cost of care requires different costaccounting methods than prevailing approaches such asdepartmental, charge-based, or RVU-based costing Cost should be measured for each patient over the full cycleof care for the condition, or by primary care segment Cost is the actual expense of patient care, not the sum ofcharges billed or collected Cost is driven by the use of all the resources involved in apatient’s care (personnel, facilities, supplies,and support services)– Time and actual costs, not arbitrary allocations Understanding costs requires mapping the care processSource: Kaplan, Robert and Michael E. Porter, “The Big Idea: How to Solve the Cost Crisis inHealth Care”, Harvard Business Review, September 1. 201114Copyright 2018 Professor Michael E. Porter
New Slide on Cost15Copyright 2018 Professor Michael E. Porter
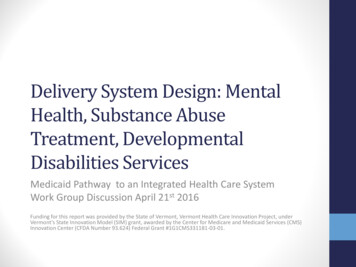
Mapping Resource UtilizationMD Anderson Cancer Center – New Patient VisitRegistration and VerificationIntakeClinician VisitPlan of CareDiscussionReceptionist, Patient AccessSpecialist, InterpreterNurse,ReceptionistMD, mid-level provider, medicalassistant, patient servicecoordinator, RNRN/LVN, MD, midlevel provider, patientservice coordinatorPlan of CareSchedulingPatient ServiceCoordinatorDecision PointTime (minutes)Source: HBS, MD Anderson Cancer Center16Copyright 2018 Professor Michael E. Porter
Major Cost Reduction Opportunities in Health Care Utilize physicians and skilled staff at the top of their licensesEliminate low- or non-value added services or testsReduce process variation that increases complexity and raises costReduce cycle times across the care cycleInvest in additional services or higher costs inputs that will lower overallcare cycle costMove uncomplicated services out of highly-resourced facilitiesReduce service duplication and volume fragmentation across sitesRationalize redundant administrative and scheduling unitsIncrease cost awareness in clinical teamsDecrease cost of claims management process Our work reveals typical cost reduction opportunities of 20-30 %Many cost improvements also improve outcomes17Copyright 2018 Professor Michael E. Porter
Move to Value-Based Payment ModelsVolumeValueFee for ServiceCapitation/PopulationBased PaymentsPay for care for a lifeGlobal BudgetsBundled PaymentPay for care for conditions(acute, chronic) andprimary care segments Both approaches create positive incentives for reducing costsand separate payment from performing particular services Capitation at the hospital or system level can coexist withbundle payment at the condition level18Copyright 2018 Professor Michael E. Porter
Emerging Value-Based Payment ModelsBundled PaymentCapitation (Population-Based) A single risk-adjusted payment for theoverall care for a life A single risk adjusted payment for theoverall care for a condition Not for a specialty, procedure, or shortepisode Responsible for all needed care inthe covered population Covers the full set of services needed overan acute care cycle, or a defined timeperiod for chronic care or primary care Accountable for population levelquality metrics Contingent on condition-specificoutcomes Including responsibility for avoidablecomplications At risk for the difference between thesum of payments for the population andoverall spending At risk for the difference between thebundled price and the actual cost of allincluded services Limits of responsibility for unrelated careand outliersProviders take disease incidence risk,not just execution/outlier risk Accountable for costs and outcomes,patient by patient, and condition bycondition Accountable for overall cost andpopulation level quality measures19Copyright 2018 Professor Michael E. Porter
Bundled Payment in PracticeHip and Knee Replacement in Stockholm, Sweden Components of OrthoChoice bundle-Pre-op evaluationLab testsAll RadiologySurgery & related admissionsProsthesisDrugsInpatient rehab-All physician and staff fees and costs1 follow-up visit within 3 monthsResponsible for complications and anyadditional surgery to the joint within 2 yearsIf post-op deep infection requiringantibiotics occurs, guarantee extends to 5years Initially applied to all relatively healthy patients (i.e. ASA scores of 1 or 2) Mandatory reporting by providers to the joint registry plus supplementary reporting The Stockholm bundled price for a knee or hip replacement is about US 8,300Results:‒ Complications fell 18% after 2 years‒ Functional outcomes remained constant‒ Length of stay fell 16%‒ Volume shifted toward specialty hospitals and away from full service acutehospitals‒ Standardization and improvement of care processes and efficiency took place‒ Patients were exceptionally satisfied20Copyright 2018 Professor Michael E. Porter
Adoption of Bundled Payments Providers– American Hospital Association survey indicated 59% of large hospitals and 33% ofsmall hospitals testing bundles Employers– 20% of surveyed employers have adopted bundled payments– Leaders such as Walmart contract directly with multiple health systems across thecountry Government– Medicare and Medicaid programs leading implementation CMS’s BPCI alone covers 48 medical areas and involves 1300 providers Numerous state Medicaid programs are moving to bundles Private Insurers– Slow in moving to bundles, with exceptions including Horizon Blue Cross Blue Shieldin NJ, Cigna, and United HealthCare Results– Equal or better outcomes, such as shorter length of stay and fewer readmissionsleading to improved patient satisfaction– Significant cost reduction is common The Bundled Payment Playbook is emerging21Copyright 2018 Professor Michael E. Porter
Integrate Multi-Site CareShifting The Strategic Logic of Health SystemsConfederation ofStandaloneUnits/FacilitiesClinically IntegratedCare DeliverySystem Increase volume Increase value Broad service line in eachfacility More clout in contracting andpurchasing Spread “fixed overhead” costs Use owned or affiliatedprimary care practices to“guarantee” referrals Value-based deliverymodels Concentrate, allocate, andintegrate care across theproper sites of care via IPUs The system is more than thesum of its parts22Copyright 2018 Professor Michael E. Porter
Four Levels of Provider System Integration1. Defining the overall scope of services for each unit, and for thefacility/system as a whole, where it can deliver high value Affiliate when this creates value2. Concentrate volume of patients by condition in fewer locationsto improve outcomes and efficiency3. Perform the right services in the right locations based on acuitylevel, resource fit, and the benefits of patient convenience forrepetitive services– E.g., move less complex surgeries out of tertiary hospitals to smallerfacilities and outpatient surgery centers4. Integrate the care cycle across sites via an IPU structure– Common scheduling– Digital services and telemedicine can help tie together the carecycle23Copyright 2018 Professor Michael E. Porter
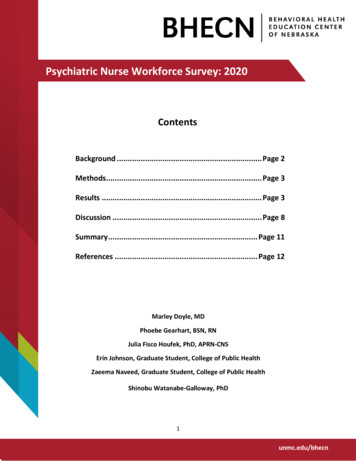
Delivering the Right Care at the Right LocationRothman Institute, PhiladelphiaFacility CapabilityLowest ComplexityAmbulatory Surgery CenterLowMediumHighest ComplexityCost of Total HipReplacement: 12,000 USDRothman OrthopaedicSpecialty HospitalBryn MawrCommunity HospitalCost of TotalHipReplacement 45,000 USDJefferson UniversityAcademic Medical CenterPatient Risk Factors: Age, Weight, Expected Activity, General Health, and Bone Quality24Copyright 2018 Professor Michael E. Porter
Children’s Hospital of Philadelphia Care NetworkWholly-Owned Outpatient UnitsPrimary Care PracticesSpecialty Care CentersSpecialty Care Center, Surgery Center& After-Hours Urgent CareSpecialty Care & Surgery CentersSpecialty Care Center, Surgery Center, AfterHours Urgent Care & Home CareCommunity Inpatient PartnershipsCHOP Newborn CareCHOP Pediatric CareCHOP Newborn & Pediatric CareHospital & IntegratedSpecialty Program25Copyright 2018 Professor Michael E. Porter
Broad Based Affiliations Across a RegionVanderbilt Health Affiliated Network (VHAN) A Clinically Integrated System12 health systems45 hospitalsOwnership remains with each institutionJoint efforts to improve outcomes and lower costReferrals across organizationsJoint ventures on selected service linesShared support servicesCommon health plan with 100K lives covered26Copyright 2018 Professor Michael E. Porter
Expand Geographic ReachThe Cleveland Clinic Cardiac Affiliate ProgramRochester General Hospital, NYCardiac SurgeryChester County Hospital, PACardiac SurgeryCLEVELAND CLINICCentral DuPage Hospital, ILCardiac SurgeryThe Bellevue Hospital, OHCardiac SurgeryFisher-Titus Medical Center,OHCardiac SurgeryPikeville Medical Center, KYCardiac SurgeryCape Fear Valley Medical Center, NCCardiac SurgeryMcLeod Heart & Vascular Institute, SCCardiac SurgeryCleveland Clinic Florida Weston, FLCardiac Surgery27Copyright 2018 Professor Michael E. Porter
Build an Enabling IT PlatformAttributes of a Value-Based IT Platform1. Combines all types of data for each patient across the full care cycle (notes, labtests, genomics, imaging, costs) using standard definitions and terminology2. Tools to capture, store, and extract structured data and eliminate free text3. Data is captured in the clinical and administrative workflow4. Data is stored and easily extractable from a common warehouse. Capability toaggregate, extract, run analytics and display data by condition and overtime5. ͏Full interoperability allowing data sharing within and across networks, EMRplatforms, referring clinicians, and health plans6. Platform is structured to enable the capture and aggregation of outcomes,costing parameters, and bundled payment eligibility/billing7. Leverages mobile technology for scheduling, PROMs collection, secure patientcommunication and monitoring, virtual visits, access to clinical notes, and patienteducation28Copyright 2018 Professor Michael E. Porter
The Imperative of Outcome Measurement Outcomes encourage multidisciplinary IPUs andfacilitate care improvement Outcomes highlight and validate value-enhancingcost reduction Outcomes enable shifting to true value-basedbundled payments Outcomes guide the delivery of the right servicesat the right locations Outcomes define areas for service line choicesand areas for affiliation Outcomes define success for the patient, theclinical team and the payor Standardization of outcomes by condition unlockscomparison and improvement29Copyright 2018 Professor Michael E. Porter
Evolution of Outcome MeasurementEmergence of OutcomesFocus on QualityFocus on SafetyFocus on High QualityHospitalsFocus on PerformanceImprovement1910s – 1940s1950s – 1980s1980s – 2000s1990s1990sErnest Codman Father of outcomemeasurement Tracked patients withend result cards Surgeons refused toparticipate Codman’s hospitalprivileges revokedAvedis Donebedian Described thedimensions of healthsystem quality asstructure, process,and outcomes Led to widespreadmeasurement ofstructure and process Little progress onoutcome measurement Significant publicpressure to improveafter high profile neverevents (e.g Libby Zion,Betsy Lehman, JosieKing) The Institute ofMedicine released tworeports – “To Err isHuman” & “Crossingthe Quality Chasm” –outlining new aims forcare delivery thathighlighted safety andprocess Institute for HealthcareImprovement (1991)founded to lead theimprovement of healthcare throughout theworldU.S. News – BestHospitals First prominent effortto benchmark Structure, process &outcomes adopted asthe measurementframework Systematicmeasurement ofstructural indicators Process qualityinferred fromreputation surveys Outcomes limited toinpatient mortality Healthcare looked toother industry to guideimprovement includingSix Sigma and LeanManagement Despite recognition of its importance, outcome measurement limited or nonexistent30Copyright 2018 Professor Michael E. Porter
Evolution of Outcome Measurement: New Era of ValueIntroduction of the ValueAgendaCreation of StandardOutcome Sets20062011 Outline six stepsneeded to achievevalue Spearheadedsignificant effortsaround the world toimplement valuebased health care Non-profitorganizationfounded byindividuals fromthree esteemedinstitutions Purpose totransform healthcare systemsworldwide bymeasuring andreporting patientoutcomes in astandardized way31Copyright 2018 Professor Michael E. Porter
What is a Health Outcome?The Quality Measurement LandscapePatientExperience/Engagement/ AdherencePatient InitialConditions,Risk omesE.g., PSA, surgicalmarginStructureE.g., Staffcertification,facilities standards32Copyright 2018 Professor Michael E. Porter
Principles of Outcome Measurement Outcomes should be measured by condition or primary care segment– Not for specialties, procedures, or interventions Outcomes are always multi-dimensional and include what matters most to patients, not justto clinicians– Patient reported outcomes are important in every condition Outcomes cover the full cycle of care Should be continuously collected over time Outcome measurement includes initial conditions/risk factors to control for patientdifferences Outcomes should be standardized for each condition to maximize comparison, learning, andimprovement Outcomes should be measured in the line of care Value-based principles differ from the historical focus on provider behavior versus overallpatient success33Copyright 2018 Professor Michael E. Porter
The Outcome Measures HierarchyTier1Health StatusAchievedor RetainedSurvivalDegree of health/recovery Achieved clinical status Achieved functional status Time to diagnosis and treatmentTier2Process ofRecoveryTime to recovery and return to normal activities Time to return home Time to return to normal activitiesDisutility of the care or treatment process (e.g., diagnostic errors and ineffectivecare, treatment-related discomfort, complications, or adverse effects, treatmenterrors and their consequences in terms of additional treatment) Care-related pain/discomfort Complications Re-intervention/readmissionTier3Sustainabilityof HealthSource: NEJM Dec 2010Sustainability of health/recovery and nature of recurrences Long-term clinical status Long-term functional statusLong-term consequences of therapy (e.g., care-induced illnesses)34Copyright 2018 Profe
Source: Porter, Michael E., Clemens Guth, and Elisa Dannemiller, The West German Headache Center: Integrated Migraine Care, Harvard Business School Case 9707--559, September 13, 2007 . Organize by Specialty and Discrete Service. Re-organize Care Around Patient Medical Conditions. Headache Care in Germany