Transcription
Pharmacy Practice Advancement CommitteeA primer on pharmacybenchmarking andproductivity monitoringPharmacy NetworkAugust 2018 2018 Vizient, Inc. All rights reserved.
ContributorsPhil BrummondFroedtert and The Medical College of WisconsinLisa ForsythBeaumont Hospital – Royal OakMarshall JohnsonFroedtert and The Medical College of WisconsinKerry MooreOregon Health and Sciences University HealthcareChristy NormanEmory HealthcareKristin O’ReillyFroedtert and The Medical College of WisconsinCelia ProctorThe Johns Hopkins HospitalTyler VestUniversity of North Carolina HospitalsTara B. VlasimskyDenver Health and Hospital Authority 2018 Vizient, Inc. All rights reserved.A primer on pharmacy benchmarking and productivity monitoring – Aug. 20182
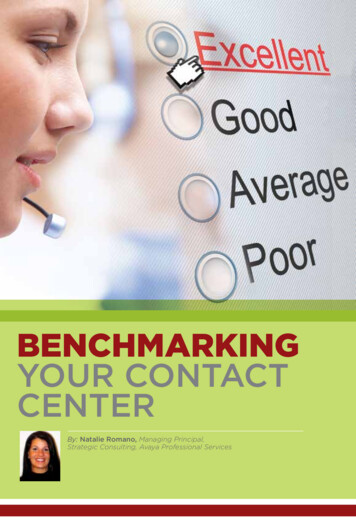
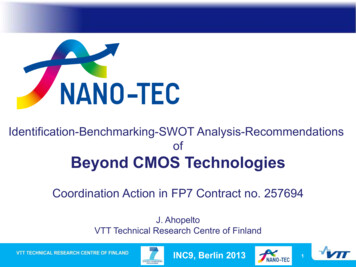
Pharmacy Benchmarking and ProductivityMonitoringThe best metric (goal) to monitor pharmacy productivity isa combination of workload, labor, cost, and outcomesExternalBenchmarking:Comparing yourinstitution to othersover timeInternal Benchmarking:Comparing to oneself23%Individuals rate overallknowledge and understandingof internal productivity monitoringas very high12%Individuals rate overall knowledgeand understanding of externalproductivity monitoring as veryhigh87%Respondents reportingdepartment currently usesan internal productivitymonitoring process(n 101/116)74%37%Respondents indicate organizationflexes staffing based uponproductivity metricsChallenges33%Identifying an appropriatecomparison groupSurvey respondents heldaccountable to externalproductivity metrics in theirorganization’s annual budgetingprocess (n 94/127)59%Most commonly used externalproductivity monitoring vendor:Truven/Action OI22%Organization/senior leadershipunderstanding of metrics and buy-inPharmacy Intensity Score resource-based relative valueintensity (R‐BRVI) grouping systemthat utilizes pharmaceutical resourceconsumption data to produce DRGspecific drug use requirements(weights) 2018 Vizient, Inc. All rights reserved.16%No perfect metric to capture clinicalservices vs. dispensing activitiesA primer on pharmacy benchmarking and productivity monitoring – Aug. 20183
Benchmarking 1011, 2Benchmarking made its first appearance in thehealthcare system in 1990, when standards andrequirements were implemented by the Joint1Commission on Accreditation of HealthcareOrganizations (Joint Commission). The JointCommission defined benchmarking as ameasurement tool for monitoring the impact ofgovernance, management, clinical, and logisticalfunctions. Benchmarking has become an area ofstrategic focus over the past decade with threeaims: to control healthcare costs; to mitigate riskand improve the quality of care; and improvepatient satisfaction. Benchmarking allows a healthcare team or organization to understand how theirperformance compares to a similar group with apurpose of identifying and implementing the bestpractices of peer organizations to improve theirperformance. Metrics used in benchmarking comefrom many sources but may be used tounderstand performance on standards set by aregulatory body or agency. 2018 Vizient, Inc. All rights reserved.While benchmarking is often thought of as simplycomparing financial, productivity, and qualityindicators between several organizations, it shouldrather be seen as part of a comprehensivecontinuous quality improvement (CQI) plan. Thereis no single metric that will adequatelydemonstrate the value a pharmacy departmentdelivers. In order to be successful in usingbenchmarking tools, a focus should be placed onunderstanding when to use internal versusexternal benchmarking, carefully identifying keyindicators, understanding the data that makes upeach metric, involving staff in processimprovement efforts, and communicating thebenchmarking results with stakeholders.A primer on pharmacy benchmarking and productivity monitoring – Aug. 20184
Benchmarking can be completed by taking thefollowing steps: Select the service or activity to be reviewedthrough benchmarking Determine whether internal or externalbenchmarking is most appropriate Identify key indicators to measure and setperformance targets Collect and validate the data Measure performance Identify and address challenges with data and/orperformance Implement changes to improve results Communicate results, including how to interpretperformanceOperational and Process MeasuresFrom an operational perspective benchmarking isa tool that can be utilized by pharmacy leaders tobetter understand the work that is being done andidentify potential opportunities to improveefficiency and reach of services. These measurestypically look at resource utilization to deliver careover time – either as labor (i.e., staff work effort),medications, or some combination.Work effort measures identify a time standard andvolume metric that can be measured over time.The mean time required to perform a task, or timestandard, can be developed by direct observation,self-reporting, work sampling, or adopting a timestandard from a similar organization. A volumeindicator, or frequency of reported task, can beobtained from the pharmacy’s inventorymanagement system, the organization’s electronichealth record, or the organization’s billing systems. 2018 Vizient, Inc. All rights reserved.Once metrics are defined, the determined timestandard (e.g., time required to enter a medicationorder) is multiplied by the volume indicator (e.g.,number of medication orders) to generate the totalstaff time required for each specified activity overa period of time (e.g., total time required to entermedication orders per day), usually in totalminutes or workload units (WLU). The measure isthen tracked over time to look for trends and beable to anticipate workload fluctuations.Suggested Pharmacy OperationalMeasures Labor-based:- Worked hours per unit of service- Labor expense per 1,000 doses billed- Pharmacist worked hours per dose- Labor cost per admission- Doses dispensed per admission- Pharmacist : Technician skill mix ratio Non-Labor based:- Drug cost per admission (can also be a clinicalmeasure)- Inventory turns per year Combination:- Total cost per admission- Pharmacy costs as a percentage of totalhospital costsClinical Measures3Due to the variation in services provided bypharmacy departments across the country, clinicalworkload measures and metrics have not beenwell defined. While utilizing pharmacists tocomplete clinical activities may increase overallcosts of the pharmacy department, thesemeasures should illustrate the impact pharmacistshave on judicious use of medications and optimalpatient outcomes. Thus organizations shouldstrive to tie clinical activities to patient andfinancial outcomes. A metric that is commonlyused to measure pharmacist workload is numberof clinical interventions. Examples of clinicalinterventions include I.V.-to-oral conversions,dosage adjustments for renal insufficiency, drugA primer on pharmacy benchmarking and productivity monitoring – Aug. 20185
information questions answered, pharmacokineticservices provided, avoidance of allergy andadverse drug reactions, order clarifications, andpatient educations completed. However, thismetric does not account for the various clinicalfunctions performed by pharmacists and requiresa significant amount of time to document.Furthermore, there is not a validated method tomeasure the economic impact of routinepharmacist clinical interventions and services.Incorporating quality-based measures into adepartment’s balanced scorecard can betterportray the overall value of a pharmacydepartment’s clinical services to senior leadersrather than just focusing on drug expense andwidgets. This can be challenging because thevalue of clinical interventions is not always clearlydefined in the literature, plus many organizationsdo not recognize the value of soft dollar “costsavoided”. There are hard dollar quality outcomesthat can be used which directly affectreimbursement such as readmission rates.However, organizations can have overlappingsystem interventions that target the sameoutcome, so it can be challenging to link apharmacy service specifically to a quality outcomechange. Thus, pharmacy leaders must be able toexplain how pharmacy services impact qualitymeasures in a way that is meaningful for theorganization.Internal BenchmarkingInternal benchmarking allows an organization, ordepartment, to compare process and performanceover time. Internal benchmarking requires an initialand ongoing internal comparison to establish andmaintain a system of measures with goals.Internal benchmarking assists pharmacydepartments in determining what resources arenecessary to provide optimal clinical anddistributive services within the pharmacydepartment. A good internal productivitymonitoring system will enable a pharmacy directorto trend productivity and performance bymonitoring workload and cost metrics in relation toa volume indicator. Internal benchmarking canalso be used to provide objective data whenimplementing a new service or modifying anexisting service. It can be especially useful whenadditional labor resources are needed as a resultof volume expansion or service expansion. Thereis no gold standard method for internal productivitymonitoring. The key is to identify metrics that arevalidated, accurate, and applied consistently overtime to assess the pharmacy department’ssuccess. 2018 Vizient, Inc. All rights reserved.Once the internal measures that will be trackedhave been identified, the next step is to collectdata to determine appropriate baselines. Identifythe core activities that constitute most of the totalstaff workload (e.g., obtaining medication histories,providing medication counseling, checkingmedication doses and adjusting them as needed,documenting and avoiding drug allergies orinteractions, participating in patient care rounds,and providing pharmacokinetic services).Departments can consider using a separateproductivity monitoring system for the variousservices provided. These may include: sterileproducts area, repackaging area, purchasingactivities, and decentralized clinical services.Then, determine how workload will be measuredfor each task (e.g., utilize pharmacy learners, timestudies, industrial engineering students, Delphiprocess, etc.) and how often the workload andvolume will be reported and trended.A primer on pharmacy benchmarking and productivity monitoring – Aug. 20186
External BenchmarkingWhen should we compare apples to oranges? Theanswer to this rhetorical question is “never”, butwhen doing external benchmarking that is exactlywhat pharmacy leaders do. Externalbenchmarking enables a department to comparetheir performance against other organizations.This comparison can bolster justification ofexisting services or growth of new services butthere are several key factors to consider whenusing external benchmarking in order toappropriately select comparator organizations.The key to success in this endeavor is to identify apharmacy department or organization that issimilar with respect to the patient populationsserved, pharmacy services provided (operationaland clinical), and performance metrics used. Forexample, it would not make sense for a small,rural community hospital to attempt to benchmarkagainst an urban, tertiary academic medicalcenter. Patient population comparisons are alsoimportant with respect to geography (rural vs.urban), but even more importantly in terms ofacuity level. Organizations that specialize incomplex service lines will have higher expensesand potentially additional pharmacy departmentneeds compared with those that do not. Forexample, organizations with transplant servicesnot only have higher medical and pharmaceuticalexpenses they also often have interdisciplinarycare teams that manage patients longitudinallyboth in the inpatient and ambulatory care settings.Or there may be other reasons necessitatingunique peer groups such as safety netorganizations who primarily provide care forunderserved populations with more cultural,language and literacy barriers. These patients maynot be as clinically complex but they often requiremore pharmacist time to provide medicationmanagement services that increase the cost ofcare.For this reason, a cost metric of total pharmacycost per patient day often does not accuratelyreflect the acuity of the patients being managed,especially in an acute care setting, and canunderestimate the impact of clinical pharmacyservices that are provided. Organizations must 2018 Vizient, Inc. All rights reserved.attempt to adjust for this limitation by using anadjustment factor; however, the adjustment factorused is critical. For example, Case-Mix Index(CMI) is commonly used, but is based on overall“resource” consumption and medically complexpatients are not always the same aspharmaceutically complex patients. A better acuityadjustment factor is the Pharmacy Intensity Score(PIS) which links together pharmaceuticalresource consumption with Disease-RelatedGroups (DRGs) to adjust ratios and allowimproved comparisons between pharmacyorganizations regardless of patient mix. Key toremember is to always report a labor metric with acorresponding cost metric – these are highlydependent on each other and should both bereported to demonstrate the value of pharmacylabor to drive down drug expense.When selecting external benchmarking metrics, itis also important to understand how these metricsare calculated. Doing so will help leadersunderstand their limitations. For example, a laborproductivity metric of full-time-equivalents (FTEs)per dose dispensed does not factor in that thelabor time required to dispense a unit-dosepackaged tablet is very different compared with asterile chemotherapy preparation. Anothercommon issue, especially with growing ambulatorypractice settings is when metrics combineinpatient and ambulatory practice settingstogether. There is no common denominator thatcan appropriately explain the performance of bothinpatient and ambulatory services because t
comparing financial, productivity, and quality indicators between several organizations, it should rather be seen as part of a comprehensive continuous quality improvement (CQI) plan. There is no single metric that will adequately demonstrate the value a pharmacy department delivers. In order to be successful in using benchmarking tools, a focus should be placed on understanding when to use .