Transcription
CALIFORNIAHealth Care AlmanacREGIONAL MARKETS SERIESDECEMBER 2020San Joaquin Valley: Despite Poverty and CapacityConstraints, Health Care Access Improves Summary of Findingspitals, some independent hospitals struggled. SeveralCalifornia’s San Joaquin Valley is geographically and eco-smaller hospitals have struggled financially, leading onenomically diverse. Known for rich irrigated farmland anddistrict hospital to close permanently and another toagricultural output, the region is home to Fresno, a city ofcede management to a larger hospital system aftermore than 500,000 residents. Across the region, which spansclosing temporarily. Given the large and growing share ofthe counties of Mariposa, Madera, Fresno, Kings, and Tularethe region’s Medi-Cal population, almost all hospitals playin the San Joaquin Valley, more than 20% of the 1.8 milliona significant role in the fabric of the region’s safety net.residents have incomes below 100% of the federal povertylevel (FPL). At the same time, there are pockets of affluenceWhile financial performance improved in larger hos- While many physicians continue to practice indepen-in the region, primarily in north Fresno, where providers viedently in solo or small practices, some are choosingfor privately insured and Medicare patients.to affiliate with hospitals. The pace at which physicianIn 2019, nearly half of the residents in the San Joaquinpractices have aligned with hospitals has been slowerValley were covered by Medi-Cal (44%), and 8% werethan in other regions. However, the physician practiceuninsured. Despite the expansion of the safety net afterlandscape continues to shift as financial pressures, marketimplementation of the Affordable Care Act (ACA), includingconditions, and demographics all combine to make inde-growth of Federally Qualified Health Centers (FQHCs) andpendent practice less attractive.Rural Health Clinics (RHCs), the San Joaquin Valley continuesto face problems with access to care, especially for behavioral region, sparking competitive tensions in some areas.health services, and struggles to recruit physicians and otherFQHCs now provide services to more than half of thehealth care professionals. The COVID-19 pandemic — whichregion’s Medi-Cal enrollees. Both FQHCs and RHCs arehit the region particularly hard, though later than the rest ofworking with hospitals to improve care integration andCalifornia — has compounded these challenges.access to specialty services for Medi-Cal patients.The region has experienced a number of changes sincethe previous study in 2015–16 (see page 23 for more informa-FQHCs and RHCs continue to expand across the While several hospitals have taken a leap towardtion about the Regional Markets Study). Key developmentsglobal risk contracts, the movement toward risk-include:based arrangements for other providers has been1slow. Most providers are developing the infrastructure toThis paper is one of seven included in CHCF’s 2020 Regional Markets Study. Visit our website for the entire Almanac Regional Markets Series.
manage risk-based payment, but the market, particularlyworse outcomes if affected individuals contract the virus.for specialty care, remains heavily tied to fee-for-serviceThe regional economy’s heavy reliance on agriculture and(FFS) payment.food processing may have softened the pandemic’s initialeconomic impact in the region but put workers at higherShortages of physicians and other health care pro-risk of contracting and spreading the virus.fessionals continue to plague the region, even withscholarships, loan repayments, and other recruit-Market Backgroundment incentives. Shortages exist across a range ofThe San Joaquin Valley is a study in contrasts. Known for itsspecialties, notably psychiatry (especially pediatric psy-bountiful farmland, the region also is home to the city ofchiatry), dermatology, optometry, pain management,Fresno, where more than a quarter of the region’s 1.8 millionand orthopedics. The San Joaquin Valley’s relatively lowresidents live (see Table 1, page 3). About halfway betweenrankings on a range of quality-of-life measures mayInterstate 5 to the west and the Sierra Nevada mountaininhibit recruitment and retention of clinicians. range to the east, Highway 99 runs through the heart of theData sharing among San Joaquin Valley providersregion, connecting Fresno to the region’s second-largest cityremains challenging despite the presence of a health— Visalia, with a population of about 134,000 — to the southinformation exchange (HIE) serving the region’s twoin Tulare County. Just west of Visalia is Hanford, the largestlargest counties, Fresno and Tulare. While hospitalsKings County city, with a population of about 53,000. Northreport participating in the HIE, many outpatient provid-of Fresno, up Highway 99, the city of Madera, in the county ofers reported limited use. Barriers to adoption includethe same name, is home to about 61,000 people. Outside ofperceived challenges of integrating practices’ electronicthese population centers, the region is predominantly ruralhealth record (EHR) systems with the platform and a lackfarmland or undeveloped, including Yosemite National Park,of staff resources.which spans Madera and Mariposa Counties.The region’s economy is largely agricultural; nearly 400Access to mental health and substance use disor-different crops, ranging from fruits and vegetables to hayder (SUD) services for Medi-Cal enrollees has beenand cotton, are grown there. While composing less than 1%improving, though significant gaps in care remain.of the nation’s farmland, the region’s farms supply 8% of theInpatient psychiatric beds are in short supply. This short-nation’s agricultural output, in a contribution valued at moreage may be offset by a new 128-bed inpatient psychiatricthan 17 billion annually. Against this backdrop of agricul-facility slated to open in Madera County in 2023. Countytural production, more than one in five people (21.5%) inspecialty mental health plans in the region have adoptedthe region had incomes in 2020 below the FPL of 26,200more holistic approaches to addressing behavioral healthfor a family of four.2 The share of people in the region livingneeds, developing partnerships with health plans andin poverty declined 6 percentage points from 2014 butadding new services. remained 50% higher than the statewide average. Moreover,Health and income disparities, as well as otherthe Fresno metropolitan area has the second-highest con-sociodemographic factors, have worsened the impactcentrated poverty rate — a measure of families living inof the COVID-19 pandemic in the San Joaquin Valley.neighborhoods with a poverty rate exceeding 40% — in theThe region’s residents suffer disproportionately from risknation.3 Median household income in the region, at 52,621,factors, such as obesity and asthma, that can lead tois two-thirds of the statewide median. In the city of Fresno,California Health Care Foundation2www.chcf.org
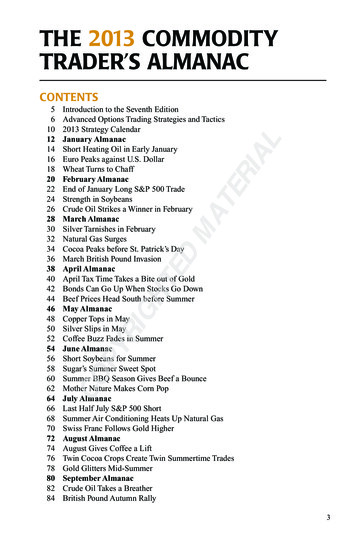
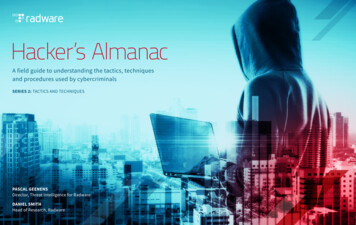
legacies of segregation and stark health differences remainTABLE 1. D emographic CharacteristicsSan Joaquin Valley vs. California, 2018between the more affluent and mostly White residents to theSan Joaquin ValleyCalifornia1,786,77039,557,0453.2%3.2%north and the poorer and mostly Black and Latinx residentsPOPULATION STATISTICSTotal populationFive-year population growthto the south and southwest. From one zip code to another,life expectancy can drop by 20 years.4While the region’s population grew rapidly following theAGE OF POPULATION, IN YEARSUnder 1828.6%22.7%Great Recession, the pace has slowed in recent years. Of the18 to 6459.2%62.9%seven study markets, Latinx residents account for the highest65 and older12.2%14.3%percentage of residents in the San Joaquin Valley — at 56.7%,Latinx56.7%39.3%White, non-Latinx29.9%36.8%Black, non-Latinx3.7%5.6%age 18. Educational attainment in lower compared to theAsian, non-Latinx7.1%14.7%rest of the state: among San Joaquin Valley residents, 74.3%Other, non-Latinx2.6%3.6%hold a high school diploma and 28.1% have college degrees.21.7%25.5%High school diploma or higher74.3%83.7%College degree or higher28.1%42.2%RACE/ETHNICITYwell above the 39.3% statewide average. The region’s population skews young, with nearly 29% of residents younger thanWhile these indicators have improved in recent years, theyBIRTHPLACEForeign-bornare still well below the statewide averages of 83.7% andEDUCATION42.2%, respectively.Despite sharing in the state’s economic growth prior tothe COVID-19 pandemic, high unemployment (8.1%) remainsECONOMIC INDICATORSBelow 100% federal poverty level (FPL)21.5%12.8%a major challenge, as it was nearly double the statewide100% to 199% FPL23.8%17.1%unemployment rate (4.2%) in 2018. The region also lags onHousehold income 100,000 22.6%38.0%other quality-of-life measures. The five counties are ranked 52,621 75,2778.0%4.2%as having among the highest air pollution levels in the state.50.0%31.0%Median household incomeUnemployment rateAble to afford median-priced home* (2019)San Joaquin Valley residents benefit from relatively affordablehousing stock: 50% of the region’s households earn enoughSources: “County Population by Characteristics: 2010–2019,” Education by County, FPL by County,Income by County, US Census Bureau; “AskCHIS,” UCLA Center for Health Policy Research (confidenceintervals are large for Humboldt County and are included in the table); “Employment by IndustryData: Historical Annual Average Data” (as of August 2020), Employment Development Dept., n.d.;and “Housing Affordability Index - Traditional,” California Association of Realtors. All sources accessedJune 1, 2020.California Health Care Foundationto purchase a median-priced home in the region, a measure19 percentage points higher than the statewide statistic.53www.chcf.org
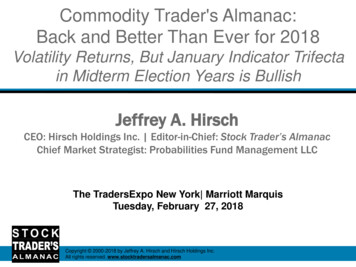
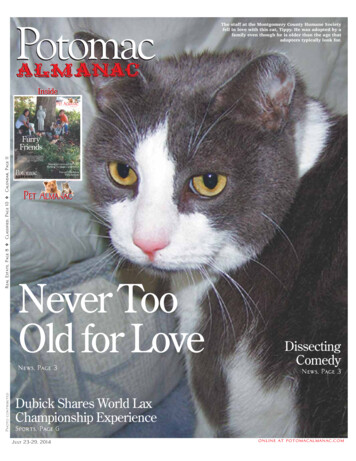
San Joaquin Valley Reports Worse Health Status thanOther RegionsMedi-Cal Dominates Health Insurance CoverageThe physical health of San Joaquin Valley residents is amongimproving economy, continued to reduce the share of Santhe poorest in the state (see Table 2). When compared withJoaquin Valley residents without health insurance. Betweenaverages for all Californians, San Joaquin Valley residents are2015 and 2019, the uninsured rate declined from 9.6% tomore likely to report that they are in fair or poor health, have8.0% (see Table 3).8 At 44.1%, the proportion of residents withheart disease, or have asthma, in part because of the region’sMedi-Cal coverage is higher in the San Joaquin Valley than inpoor air quality, especially in and around the city of Fresno.6any of the other markets studied and higher than the state-Both the obesity rate, above 41%, and the infant mortalitywide rate of 28.7%. The share of people with private insurancerate, at 0.6% of all live births, are about 50% higher than cor-also grew slightly from 33.6% in 2015 to 33.9% in 2019 — stillresponding rates statewide.well below the rate of 47.7% statewide. Another 14.0% of SanThe expansion of Medi-Cal under the ACA, along with an7Joaquin Valley residents are covered by Medicare, comparedTABLE 2. Physical Health IndicatorsSan Joaquin Valley vs. California, 2018with 15.9% of Californians statewide.San Joaquin ValleyCaliforniaFair/poor health21.5%18.5%Diagnosed with diabetes11.5%10.1%Has asthma21.4%15.7%Has heart disease8.2%6.8%Medicare*Preterm births*9.4%8.8%Medi-CalInfant mortality rate*0.6%0.4%Private insurance41.0%27.3%ObesityTABLE 3. Trends in Health Insurance, by Coverage SourceSan Joaquin Valley vs. California, 2015 and 2019SAN JOAQUIN VALLEYUninsured* “Preterm and Very Preterm Live Births” (2018), “Infant Mortality, Deaths Per 1,000 Live Births(LGHC Indicator)” (2017), California Dept. of Public Health, accessed September 1, 0%8.6%7.7%* Includes those dually eligible for Medicare and Medi-Cal. Includes any other insurance coverage (excluding Medicare and Medi-Cal).†Source: California Health Interview Survey, 2018 data except where noted, accessed January 21, 2020.Source: Calculations made by Blue Sky Consulting Group using data from the US Census Bureau, theCenters for Medicare & Medicaid Services, and the California Department of Health Care Services.Health and income disparities, as well as other sociodemographic factors, have likely worsened the impact of theFour of the region’s five counties participate in Medi-Cal’sCOVID-19 pandemic in the San Joaquin Valley (see “AfterTwo-Plan Model, under which a public managed care plan,Delayed Impact, COVID-19 Spreads Rapidly” on page 18).known as a local initiative, competes with a commercial plan.The region’s residents suffer disproportionately from key riskCalViva Health operates the local initiative plan for Fresno,factors, such as obesity and asthma, that can lead to worseKings, and Madera Counties and subcontracts all services tooutcomes if affected individuals contract the virus. Moreover,Health Net, a subsidiary of Centene, a large national plan thatthe region’s heavy reliance on agriculture and food process-specializes in Medicaid. CalViva covers 71% of the three coun-ing apparently softened the pandemic’s economic impactties’ 518,000 Medi-Cal managed care enrollees, while Anthem— the unemployment rate increased by a smaller amountBlue Cross, the commercial plan, serves the remainder.in the San Joaquin Valley than statewide — but put manyTulare also operates under the Two-Plan Model, with theworkers at higher risk of contracting and spreading the virus.local initiative contracted to Anthem Blue Cross. Unlike otherlocal initiatives, Tulare’s is not overseen by a county healthauthority; instead, the Tulare County Health and HumanServices Agency has a contract with Anthem Blue Cross.California Health Care Foundation4www.chcf.org
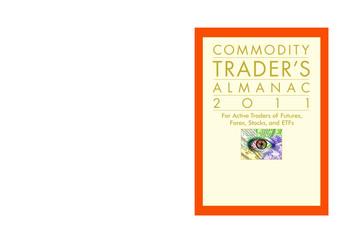
Health Net serves as the private plan and covers about 55%For the one-third of the San Joaquin Valley’s populationof the 210,000 Medi-Cal managed care enrollees. Mariposawith private insurance, the major commercial plans are Kaiser,County, where the total population is about 17,500, is partAnthem Blue Cross, Blue Shield of California Promise Healthof the state’s regional model for rural areas. Anthem coversPlan, Health Net, and Humana. For Medicare, only 29% of theabout 85% of the county’s 4,200 Medi-Cal managed careregion’s beneficiaries are enrolled in Medicare Advantageenrollees, while California Health & Wellness, another Centene(MA) managed care plans, compared with 44% statewide.subsidiary, serves the remainder.However, San Joaquin Valley Medicare beneficiaries increas-Covered California, the state’s health insurance exchange,ingly are choosing the MA option, with enrollment growingaccounts for a lower share of insurance coverage in the San5 percentage points since 2014. Kaiser is the dominant MAJoaquin Valley than statewide (see Table 4). Silver plans forplan in Fresno and Madera Counties, accounting for nearlyCovered California Region 11 — Madera, Fresno, and Kings40% and 60% of enrollees, respectively, in each county. InCounties — are only slightly less expensive than the averageMariposa, where Sierra Health is the plan for more than halfplan cost statewide, while average incomes in the regionof the MA market, Kaiser’s share is 27%. Arcadian Health Plan,are far lower than the state average. Across the Region 11a subsidiary of national carrier Humana, accounts for 52%counties, Blue Shield of California accounts for most Coveredand 57% of the MA market, respectively, in Kings and TulareCal enrollees, with Kaiser Permanente — the only other planCounties.available — covering a minority share.Hospital Sector Mostly StableIn Region 10, which includes Tulare and MariposaCounties — as well as the counties of San Joaquin, Stanislaus,Geographically segmented, mostly along county lines, theand Merced — average premiums are far higher. In MariposaSan Joaquin Valley hospital market has remained relativelyCounty, Blue Shield holds the dominant share of the Coveredstable since the previous study except for the financial strug-California market. In Tulare County, Anthem Blue Cross hasgles of several small district hospitals. The region is dominatedcaptured more than 80% of the market, with Blue Shieldby five hospitals or systems — Community Medical Centersand Kaiser covering the remainder. According to a recent(CMC), Saint Agnes Medical Center, Adventist Health, Kaweahhealth care market analysis, the difference in premium costsDelta Medical Center, and Valley Children’s Healthcare. Kaiser,between these two rating regions reflects an underlyingwhich is a dominant player in many markets elsewhere in thedifference in health care prices. Routine inpatient and out-state, operates a 169-bed hospital in Fresno and accounts forpatient hospital procedures in Region 11 cost less than inonly a small fraction of all hospital discharges in the market.Region 10, at least on a wage-adjusted basis.9There are four district hospitals — one closed in 2018, andTABLE 4. Covered California Premiums and Enrollment, San Joaquin Valley (Regions 10 and 11) vs. California, 2015 and 2019REGION 10*REGION 11*CALIFORNIA201520192015201920152019Monthly premium* (Silver Plan on the exchange for a 40-year-old individual) 299 502 315 387 312 454Percentage of population enrolled2.2%2.2%1.9%2.4%3.0%3.1%* Region 10 includes Mariposa and Tulare Counties, as well as Merced, San Joaquin, and Stanislaus Counties (which are not considered part of the San Joaquin Valley for purposes of this report). For this rating region,the weighted average monthly Silver Plan premium reflects premiums paid across all five counties (since the provided estimate of the percentage of the population enrolled is isolated to Mariposa and TulareCounties). Region 11 includes Fresno, Kings, and Madera Counties.Source: Blue Sky Consulting Group analysis of data files from “Active Member Profiles: March 2019 Profile” (as of May 31, 2020) and “2019 Covered California Data: 2019 Individual Product Prices for All Health InsuranceCompanies,” Covered California.California Health Care Foundation5www.chcf.org
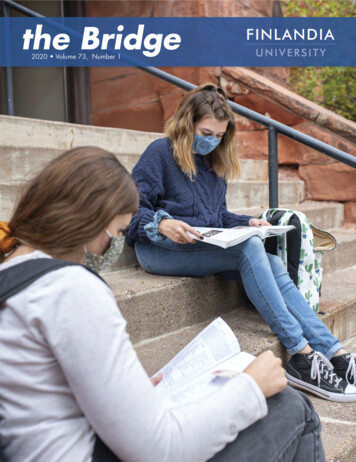
another is managed by Adventist Health — but there areand is the only hospital in Visalia, the region’s second largestno county public hospitals. Given that more than half of thecity. Kaweah Delta offers a full range of services, including aregion’s population is covered by Medi-Cal or uninsured,Level III trauma center. Medi-Cal accounted for 39% of themost hospitals play a significant safety-net role. Table 5hospital’s discharges in 2018.Valley Children’s Hospital. Part of the extensive Valleysummarizes discharges across the region’s hospitals. MajorChildren’s Healthcare system, the 358-bed Valley Children’shospitals and systems in the region include the following:Community Regional Medical Center (CRMC). As theHospital in Madera is the only children’s hospital in the Sanregion’s largest hospital with 909 beds and the area’s onlyJoaquin Valley and also serves many central California coastalLevel I trauma center and burn unit, CRMC anchors the Sancounties and the Sacramento area. Medi-Cal accounted forJoaquin Valley safety net, especially for specialty services,76% of the hospital’s discharges in 2018.and accounts for 52% of Medi-Cal discharges in FresnoThe region also is home to several smaller and indepen-County and 43% of Medi-Cal discharges across the region.dent hospitals. They include 106-bed Madera CommunityPart of Fresno-based Community Medical Center HealthcareHospital, two district hospitals in Tulare County — 167-bedNetwork — an independent nonprofit system with two otherSierra View Medical Center in Porterville and 101-bedacute care hospitals, a psychiatric hospital, a cancer institute,Adventist Health Tulare, which was formerly Tulare Regionaland several long-term care, outpatient, and other facilities —Medical Center — and, in Mariposa County, an 18-bedCRMC accounts for 62% of all Fresno County discharges andcritical access hospital, which is eligible for enhanced pay-38% of all discharges across the five counties.ments from Medicare and Medi-Cal, operated by the John C.Adventist Health. Part of a system with more than 20Fremont Healthcare District.hospitals across California, Hawaii, and Oregon, Adventisthas three hospitals in the region; the largest is 230-bedTABLE 5. Acute Care Hospitals, by Share of Discharges, San Joaquin Valley, 2018Adventist Health Hanford in Kings County, followed by57-bed Adventist Health Selma and 49-bed Adventist .9%26.3%6.4%100.0%FresnoReedley, both in Fresno County. Adventist also leases andoperates Tulare Regional Medical Center, a district hospital,which is now known as Adventist Health Tulare. Medi-Calaccounted for nearly 40% of Adventist Health’s dischargesacross the region in 2018. Adventist Health Community Medical Centers Kaiser Foundation Hospital Saint Agnes Medical Center (Trinity Health)KingsSaint Agnes Medical Center. Part of Michigan-based Adventist HealthMaderaTrinity Health, a large Catholic nonprofit health system with92 hospitals and hundreds of other facilities across 22 states,Fresno-based Saint Agnes has 436 beds and offers a full Madera Community Hospital2.6%24.4% Valley Children’s riposarange of services. In 2018, nearly half (49%) of Saint Agnes discharges were Medicare patients and 33% were Medi-Cal.John C. Fremont Healthcare DistrictTulare*Saint Agnes accounts for about 16% of all hospital discharges Kaweah Delta Health Care Districtin the region. Sierra View Local Health Care DistrictKaweah Delta Medical Center. Operated by the Kaweah* Tulare Regional Medical Center was closed for most of 2018.Source: “Hospital Annual Financial Data - Selected Data & Pivot Tables,” California Office of StatewideHealth Planning and Development, accessed June 1, 2020.Delta Health Care District, the hospital is licensed for 448 bedsCalifornia Health Care FoundationRegionalDischarges6www.chcf.org
District Hospitals Struggle FinanciallyIn part as a result of a slight reduction in beds, the region’sinpatient occupancy rate increased substantially betweenWhile the financial status of most hospitals across the region2014 and 2018, from 59.4% to 65.7%. The San Joaquin Valley’shas improved since 2014, respondents note that several dis-inpatient occupancy rate is now more than 10 percentagetrict hospitals have struggled. Adventist Health now leasespoints higher than the statewide average. Concurrent withand operates Tulare Regional Medical Center, a district hos-this shift, across the region, hospitals’ financial conditionspital, which closed due to bankruptcy in October 2017, buthave improved, with the average operating margin at 6.2%then reopening a year later under Adventist management.in 2018, up from 2.3% in 2014 and well above the statewideThe move reportedly strengthened Adventist’s market posi-rate of 4.4% (see Table 6). This increase was primarily drivention in the southern part of the region, where Adventist alsoby improved financial performance at the region’s larger hos-operates a hospital in Kings County. Another district hos-pitals (see Table 7).pital, Coalinga Regional Medical Center in southern FresnoCounty, also struggled financially and closed permanently inTABLE 6. Hospital Performance (Acute Care)San Joaquin Valley vs. California, 2018late 2018. Respondents noted that weak governance comSan Joaquin ValleyCaliforniabined with the burden of financing repairs from earthquake157178damage contributed to Coalinga’s deteriorating financialOperating margin*6.2%4.4%Paid FTEs per 1,000 adjusted patient days*12.215The three other district hospitals — Kaweah Delta, Sierra 2,696 4,488View, and John C. Fremont — had operating margins belowBeds per 100,000 populationTotal operating expenses per adjusted patient day*performance.*Excludes Kaiser.the regional average in 2018,11 with Sierra View reporting aNote: FTE is full-time equivalent.negative operating margin, declining to –3.29 from in 2018Sources: “Hospital Annual Financial Data - Selected Data & Pivot Tables,” California Office of StatewideHealth Planning and Development; “County Population by Characteristics: 2010–2019,” US CensusBureau. All sources accessed June 1, 2020.from 2.35 in 2014. In late 2018, Kaweah Delta and SierraView entered into a joint powers agreement that allows theTABLE 7. O perating Margins at Select HospitalsSan Joaquin Valley, 2014 and 2018two districts to remain independent but partner on various20142018activities, including purchasing drugs and other supplies,Community Regional Medical Center2.8%5.4%recruiting physicians, and operating clinics. This partnershipAdventist Health3.1%11.9%has also fostered creation of an integrated delivery networkKaweah Delta Medical Center0.1%4.9%to take global risk-based contracts, known as SequoiaSaint Agnes Medical Center2.3%10.8%Integrated Health.Source: “Hospital Annual Financial Data - Selected Data & Pivot Tables,” California Office of StatewideHealth Planning and Development, accessed June 1, 2020.The district hospitals have attempted to rely on voters tofinance construction of new facilities that meet state seismicOn a per-patient-day basis, net operating expense acrosssafety requirements. In 2016, voters rejected a bond measurethe region’s acute care hospitals is roughly 40% lower thanto finance construction of a new Kaweah Delta hospital tothe statewide average. And, according to one recent analysismeet 2030 seismic requirements.12 On November 3, 2020,of health care prices across California counties, the averageMariposa County voters passed Measure N, a 1% countywideprices for common procedures in the San Joaquin Valley —sales tax to fund a new facility that meets seismic require-even on a wage-adjusted basis — are among the lowest inments for the John C. Fremont Healthcare District.13the state.10California Health Care Foundation7www.chcf.org
Some Hospitals Compete Across the RegionValley Children’s Healthcare includes the Valley Children’sWhile hospital markets roughly follow county lines, inter-Medical Foundation, which contracts with the two mainviewees stressed that patients, especially in the rural outlyinggroups: Valley Children’s Specialty Medical Group and Valleyareas, often travel significant distances and cross countyChildren’s Primary Care Group. Valley Children’s Specialtyboundaries for care. CRMC and Valley Children’s were inMedical Group also provides services at other hospitals innegotiations to collaborate and avoid duplication of neona-the region, such as Saint Agnes. The Valley Children’s Primarytal and pediatric intensive care, but the efforts failed. Instead,Care Group provides primary care, obstetrical care, andthe two hospital systems ended their contractual relation-regional hospitalist services. Valley Children’s two medicalship and began to compete for pediatric patients, with CRMCgroups added physicians by acquiring eight small pediatricadding neonatal beds and constructing a pediatrics medicalpractices from 2015 to 2018. ChildNet Medical Associates, anoffice building.14 To compete for patients, hospitals haveIPA with some 300 physicians and pediatric specialists in theenlarged their outpatient primary care and specialty capacityregion, also partners with Valley Children’s Hospital.by expanding their medical foundations (see the followingRecently, Community Medical Centers established itssection), affiliating with FQHCs, or adding RHCs.own medical foundation, Community Health Partners,which includes neurosurgery, pediatric, and oncologyPhysicians Slowly Align with Hospitalsclinics. The medical foundation is part of CMC’s CommunityIn recent years, San Joaquin Valley physicians and practicesProvider Network (CPN), described as a physician supporthave continued to affiliate with hospitals, although thedivision within CMC. The CPN also contracts with medicalpace has been slower than in other regions. Absent stronggroups, such as the Central California Faculty Medical Groupmarket forces, such as widespread risk-based payment and(CCFMG), to deliver services to CMC patients and to membershigh levels of managed care, that tend to spur physician con-of CMC’s health plan, Community Care Health (described insolidation, many primary care physicians, especially in Fresnoa later section). According to a regional expert, the creationand Tulare Counties, continue to practice in small groups andof this foundation contributed to contract tensions with theare significantly less consolidated than other counties state-CCFMG, which spilled over in September 2020 and threat-wide. Specialist consolidation in the region is, on average, inened CRMC’s Level I trauma center accreditation.16line with the statewide average, although in this context asCCFMG has 230 faculty physicians affiliated with thewell, the region’s more populous counties tend to have lessUniversity of California, San Francisco School of Medicine’sspecialist consolidation.Fresno campus, UCSF Fresno, representing some 65 special-15In 2018, Saint Agnes Medical Center created a medicalties, and CCFMG trains 300 medical residents and fellowsfoundation, Saint Agnes Medical Providers, a corporate sub-each year. CCFMG provides physician services in outpatientsidiary that owns and operates clinics offering numerouscenters as well as inpatient care at CMC hospitals and Saintspecialty services. The medical foundation partners with SanAgnes Medical Center.Joaquin Valley Medical Providers (MedPro), a 700-physicanKaweah Delta established its medical foundation inindependent physician association (IPA) serving Fresno andNovember 2016 and has about 50 physicians and plans toMadera Counties, to deliver integrated services, particularlyadd staff. The foundation is part of the integrated providerfor MA plans. Saint Agnes Medical Center established MedPronetwork for Kaweah Delt
San Joaquin Valley: Despite Poverty and Capacity Constraints, Health Care Access Improves Summary of Findings California's San Joaquin Valley is geographically and eco-nomically diverse. Known for rich irrigated farmland and agricultural output, the region is home to Fresno, a city of more than 500,000 residents. Across the region, which spans