Transcription
Success StoryHow Allina Saved 13 Million By OptimizingLength of StayEXECUTIVE SUMMARYLike most large healthcare systems throughout the country, AllinaHealth’s financial health improves dramatically by optimizinginpatient care for the patients it serves.HEALTHCARE ORGANIZATIONIntegrated Delivery HealthcareSystem & Pioneer ACOPRODUCTSLate-Binding DataWarehouseHealth Catalyst Analytics PlatformSERVICESInstallation ServicesAllina recognized optimizing length of stay (LOS) was one of thekey drivers of its inpatient financial performance and developedthe technical infrastructure and analytic capabilities to understandLOS performance by the minute and not the day; adjust LOS toaccount for patient acuity and compare performance to nationalbenchmarks; make LOS data available to clinicians across theorganization in near real-time; and estimate the financial impact ofLOS opportunities to enable targeted interventions for improvement.Allina leveraged its enterprise data warehouse (EDW) and analyticsplatform and optimized LOS, yielding the following results in the firsttwo years of its improvement efforts:26,000 inpatient days saved 13.4 million in direct operating expenses savedHospital capacity (bed availability) created for 5,000 admissionsAvoided adverse patient events and reduced the total costof careProfessional ServicesWHY LENGTH OF STAY MATTERSHospital inpatient care makes up nearly one-third of all healthcareexpenditures in the United States, and represents a significantimpact on the country’s economy.1 Length of stay (LOS) is anaspect of care that can be costly for most healthcare systems if notapproached the right way.As one of the largest healthcare systems in the Upper Midwest,serving 41 communities with 13 hospitals and 61 clinics, AllinaHealth knew that if it could reduce length of stay while continuing todeliver high quality care, it could realize significant cost savings.Copyright 2017 Health Catalyst1
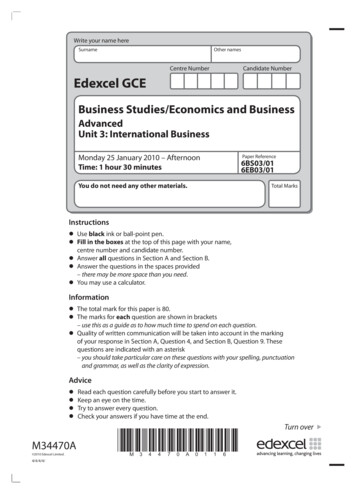
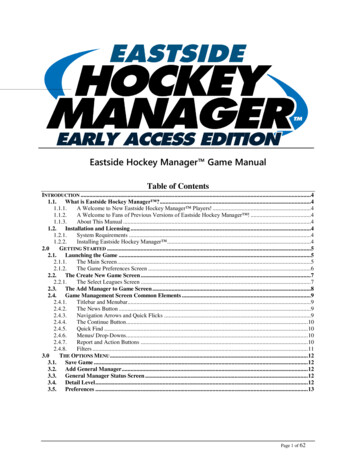
THE CHALLENGES OF IMPROVING LOSLOS improvement is aninitiative that has bothfinancial and qualitybenefits. It takes longterm commitmentfrom multidisciplinaryclinical teams who areprovided regular dataand dashboards to makesustainable improvement.There is no method thatadds capacity faster thanworking on progression ofcare. And most patients arenot asking to stay in thehospital longer!Dennis O’Hare, MDLOS Executive SponsorOptimizing LOS was a strategic priority for Allina, but there were twomain reasons its analytic and technical capabilities did not previouslyenable the organization to improve performance and reduce LOS:Meaningful opportunities for improvement could not beidentified across the organizationPerformance data could not be used to adjust clinical decisionmaking during patient hospitalizationIdentifying Opportunities for ImprovementAllina’s primary challenge was the inability to identify meaningfulopportunities for improvement across the organization. The threecontributing factors were Allina’s inability to (1) access detailed andaccurate LOS performance data, (2) adjust LOS opportunities forpatient severity of illness and benchmark its performance, and (3)estimate the financial impact of LOS opportunities.LOS calculation and reportingThe traditional method for calculating and reporting LOS in thepast 20 years was through the financial and claims infrastructure.Using this method, the finance LOS was calculated and reported inwhole days from admission date to discharge date. While accurate,this method did not take into account that patients enter and leavethe hospital at different times of the day. For example, a patientdischarged at 11 a.m. and a patient discharged at 10 p.m. on thesame day would both be calculated as one day, even though the 11a.m. discharge opened up hospital bed capacity for 11 additionalhours (see Figure 1).LOS IN DAYS3.503.002.502.001.501.000.500.00Actual LOSFinance LOSPATIENT A: Admitted on 2/1/13at 8 a.m. and discharged on2/4/13 at 11 a.m.PATIENT B: Admitted on 2/1/13at 8 a.m. and discharged on2/4/13 at 10 p.m.2.883.003.333.00Figure 1: LOS Calculation ExampleCopyright 2017 Health Catalyst2
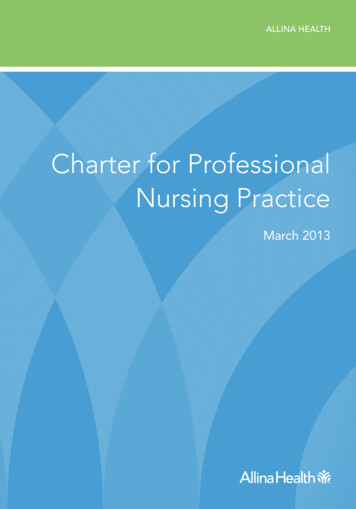
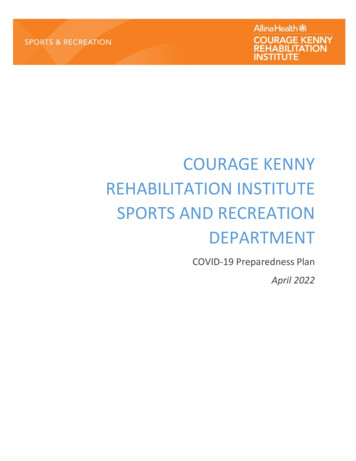
Due to the traditional method for calculating LOS, Allina was unableto understand true LOS performance and variation, and unable toidentify meaningful opportunities for improvement.Adjusting LOS for patient acuity or illness severityAllina was also unable to adjust for patient acuity or severity ofillness, a capability required for the organization to deploy itsresources appropriately and to identify LOS opportunities thatcompared similar patients. Allina’s traditional method to adjust forpatient acuity for each diagnosis-related group (DRG) of patientswas to divide the average LOS by the average case-mix index (CMI),a value that reflects the clinical complexity and resource needs foreach DRG of patients. This method was ineffective because althougha relationship existed between LOS and CMI, it wasn’t linear. Forexample, pneumonia patients without a complicating diagnosis andspinal fusion patients without a complicating diagnosis have a similaraverage LOS nationally, but very different CMIs (see Figure 2).Medicare SeverityDiagnosis RelatedGroup (MS-DRG)Simple Pneumoniawithout acomplicatingdiagnosis(MSDRG 195)Spinal fusionwithout acomplicatingdiagnosis(MSDRG 455)Geometric MeanLOS (GMLOS)2.8 days3.0 daysCase-Weight Index(CMI)0.7116.193Figure 2: Variability of Case Mix Index of Patient Groups with SimilarAverage Lengths of StayThis example demonstrates that CMI is indicative of how expensiveeach patient group is and not just the expected LOS. Using thismethod, Allina was unable to adequately adjust for patient acuity andbenchmark its performance against others, leading to an inability toidentify meaningful opportunities for improved LOS.Estimating financial impact of LOSFinally, Allina could not estimate the financial impact of LOSopportunities. Without knowing the financial impact of various LOSopportunities, it was unable to target interventions for improvementin areas that made sense clinically—and financially—forthe organization.Copyright 2017 Health Catalyst3
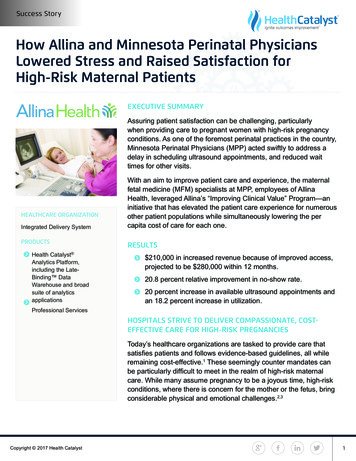
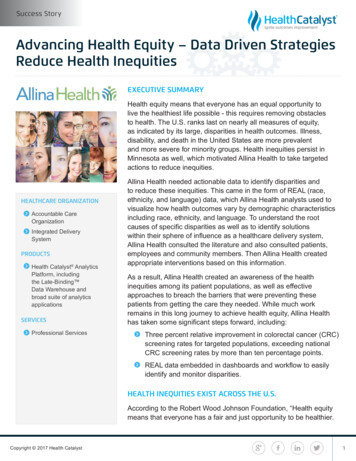
Using Performance Data for Clinical Decision MakingLength of stay is one ofthe most critical areas offocus within a critical caredelivery organization. It isone of the few initiativesthat can have a positiveimpact on all threeaspects of the Triple Aim.Organizational cost ispositively impacted both ina traditional fee-for-service,prospective paymentmodel as well as in a payfor-quality or capitationmodel. Organizations cansee increases in qualitybecause fewer days inthe hospital means feweropportunities for hospitalacquired adverse eventslike infections or falls.Finally, patient engagementis improved as days aredecreased because patientsare spending additionalnights in their own bedrather than in a hospital.Mark NelsonDirector of CorporateBusiness DevelopmentAllina was unable to improve performance and reduce LOS becauseit could not adjust its clinical decision making while patients werehospitalized. The majority of providers, care team members, andleaders across Allina lacked access to LOS data.There was also limited demand for the data because it was notclinically relevant. The process for gathering and sharing LOSdata was very resource intensive and Allina lacked the staffingresources needed to adequately disseminate available dataacross the organization. In addition, when LOS data was availableand provided, it was often provided several weeks or monthsafter patients were discharged from the hospital. Significant lagtimes prevented improved performance while patients were stillhospitalized and resulted in limited provider engagement.A NEW APPROACH TO LOS: SIX KEY CHANGESLeveraging a Late-Binding Enterprise Data Warehouse (EDW)and Health Catalyst Analytics Platform, Allina deployed six keychanges during the course of one year to address the shortcomingsof previous approaches.Accessing DataFirst, Allina developed the inpatient data mart so relevant data wasavailable to the organization. The inpatient data mart held individualpatient information from the electronic health record (EHR), includingdata on demographics, diagnoses, timestamps throughout careprocesses and pathways, and billing information. Key stakeholders,such as the hospitalists, were easily engaged in developingthe inpatient data mart because it provided access to clinicallyactionable data previously unavailable.Accurately Measuring PerformanceSecond, Allina implemented a new method for measuring performancethat adjusted for the severity of illness for one patient compared toanother. This method ensured LOS of a very sick patient was notcompared to the LOS of a healthier patient. The new performancemeasurement method used groups of related patients in the hospitalor Medicare-Severity Diagnosis Related Groups (MS-DRGs). EachMS-DRG had a national average LOS, known as the geometric meanLOS (GMLOS), and the GMLOS was used as a benchmark for Allinato compare its acuity-adjusted performance externally. Allina comparedits LOS performance with the national average to identify improvementCopyright 2017 Health Catalyst4
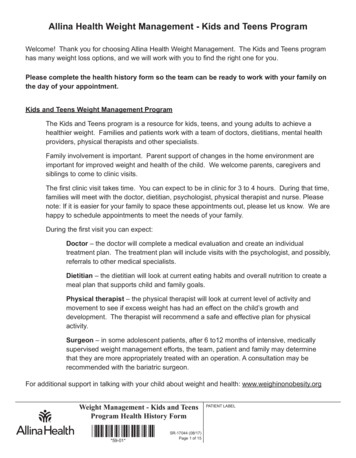
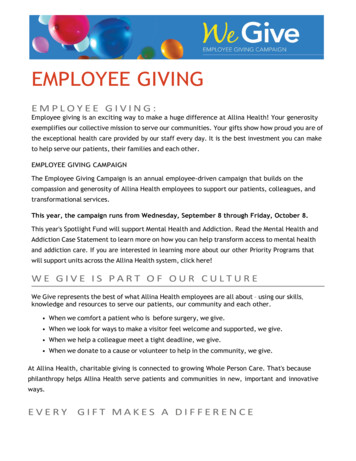
opportunities by dividing each patient’s actual LOS with the MS-DRGspecific GMLOS to identify LOS opportunities (see Figure 3).110%100%90%}}LOS longer than National AverageGMLOS (National Average LOS)LOS Shorter than National AverageFigure 3: LOS Performance Compared to the National Average for each MS-DRGIdentifying Meaningful Opportunities for ImprovementThird, Allina created performance reports for individual sites, providergroups and individual providers, clinical service lines, nursing unitsand ancillary departments, quality departments, and leadershipacross the organization. Through the analytic capabilities madepossible by Allina’s EDW and inpatient data mart, Allina identified thefollowing opportunities for improvement.Discharge OrdersThrough its performance reports, Allina discovered that the timedischarge orders were written had a smaller impact on the actualdischarge time than previously thought. Prior to having data at thisspecificity, LOS improvement initiatives were focused on having thehospitalists write discharge orders first thing in the morning beforethey rounded on the rest of their patients. Performance reportsrevealed that many hospitalists already completed discharge ordersin the early morning, but patients were rarely discharged before noonregardless of when orders were completed (see Figure 4). Throughobservation of clinical workflows and discharge processes, Allinaidentified opportunities including the following:Inconsistent or ineffective communication on the dayof discharge between the hospitalists, nurses, socialworkers, and transportation services. Many multidisciplinaryteam members were unaware of when discharge orders werewritten and/or when patients were ready to leave the hospital.Copyright 2017 Health Catalyst5
Average Time in Discharge (bar)04:00 PM06:0003:00 PM02:00 PM05:0001:00 PM12:00 AM04:0011:00 AM03:0010:00 AM9:00 AM02:008:00 AM7:00 AM01:006:00 AM5:00 3:0Average Time From Order to Discharge (line)07:0005:00 PMTime Discharge Order Was WrittenFigure 4: Relationship between Discharge Order and Time of Actual DischargeNurses and social workers were often unaware of eachpatient’s anticipated discharge date prior to the day ofdischarge. Hospitalists didn’t consistently communicate theanticipated discharge date, which meant nurses and socialworkers had insufficient time to prepare for the patient’sdischarge. Delays in ordering medical equipment for thepatient’s home, finding a patient bed at a skilled nursing facility(SNF), or confirming a ride for the patient resulted in delayeddischarges and avoidable time in the hospital.Practice Pattern VariationPerformance reports confirmed significant practice pattern variationof the hospitalists with LOS differences across all clinical conditions.The ability to view specific performance data down to the individualprovider level motivated providers and their peers to achieve higherperformance, thus enabling Allina to identify achievable opportunitiesfor improvement with strong provider buy-in.Delayed DischargesPerformance reports revealed that LOS varied by day of theweek. Data suggested inconsistent resources and more avoidablehospitals days on the weekends. Through detailed analysis, Allinaidentified limited availability of diagnostic procedures and difficulty indischarging patients to SNFs on the weekends as two key reasonsfor delayed discharges.Copyright 2017 Health Catalyst6
Understanding the Financial Impact of LOS ImprovementsIt was important for Allina to quantify benefits and estimate thefinancial opportunity as best as it could, and Allina knew the mostexpensive parts of hospital stays were the admission and dischargeprocesses, regardless of the LOS. To attempt to quantify the overallcost of saving a day of hospitalization, Allina started with hospitalstays in its medical or surgical units with four-day lengths of stayand focused on estimating expenses from day three of the four-dayhospital stays because these expenses were most representativeof the savings expected from reducing LOS. Allina developeda complex formula that estimated the bottom line impact to theincome statement. Using conservative -calculations that includedonly direct supplies and partial labor, cost savings were estimatedat a conservative rate of 500 per day, and once Allina knew theestimated cost savings per day, it was able to quantify opportunitiesand impact.Improving LOS PerformanceAllina accelerated and dramatically improved LOS performancebecause of the clinically relevant and actionable data available innear real-time. It engaged the hospitalists through frequent reportingof LOS performance data, by provider, in a way that was transparentand non-accusatory. As LOS initiatives progressed, this data led toclinical transformation and less practice pattern variation, therebyreducing overall LOS.Hospitalists partnered with multidisciplinary team members todevelop a consistent discharge planning process and establishedcommunication expectations with all team members involved inthe care of their patients. By developing a standardized process,team members were consistently informed of the anticipateddischarge date and when discharge orders were complete. Themultidisciplinary team identified the highest volume SNFs patientswere admitted to, and partnered with leadership at these SNFsto develop transfer agreements and availability standards forweekends. The highest volume SNFs agreed to accept morepatients on the weekends and Allina care teams agreed tostandardize the patient information and discharge instructions sentwith each patient to the SNF.Meeting the Demand for DataData available through Allina’s EDW and inpatient data mart createdan insatiable demand for detailed performance data across theorganization. Allina needed a new way to provide information to allCopyright 2017 Health Catalyst7
constituents that was scalable and did not require adding additionalresources. Given these constraints, Allina created the inpatientdashboard, a business intelligence solution that provided the following:An intuitive computer system that did not require significanttechnical skills to useThe ability for end users to directly access data and createdetailed reports in near real-timeThe ability to segment the population by numerous variables,including method of arrival, discharge destination, clinicalservice line, discharge unit, ICU utilization, etc.Tables and graphs that could be exported for distribution toother team membersCritical Success FactorsAllina had two critical success factors in optimizing its LOS. First,providers across the organization supported the data and believedin its accuracy due to the specificity, acuity adjustment, andbenchmarking available. Providers had strong buy-in to the data andanalytic capabilities and championed efforts with multidisciplinaryteam members to dramatically improve performance. Second,the inpatient dashboard eliminated bottlenecks in getting clinicallyrelevant and actionable data into the hands of providers in afinancially viable way. Allina’s scalable capabilities provided theorganization with transparent data that did not require hiringadditional resources.120%115%110%105%100%95%90%Year 1Year 2Year 3Year 4Figure 5: Allina Health Trending Performance to National Average LOS (GMLOS)Copyright 2017 Health Catalyst8
RESULTS OF LOS OPTIMIZATIONAllina has seen dramatic improvements in LOS in its initial yearsand has maintained performance nationally as other health systemssimultaneously work to optimize LOS performance (see Figure 5).Based on the LOS improvements made, Allina achieved significantresults in its first two years:26,000 inpatient days saved 13.4 million saved (direct impact estimated at conservativerate of 500 per day)Hospital capacity (bed availability) created for 5,000 admissions – equivalent to adding 90 new bedsAvoided adverse patient events and reduced the total costof care:Averted 90 patient falls, including 20 with harm12 patients did not get a multi-drug resistant organism, reducingtotal cost of care by 198,999 (estimated at 16,500 per)25 patients did not get a C. Diff infection (hospital-acquiredinfection), resulting in improved outcomes and reduced totalcost of careAllina’s EDW and analytics platform enabled data availability andimpacted all aspects of care delivery from the administrative officesto the patient’s bedside. The results achieved and money savedensure Allina will continue to serve people within its communitieseach and every day.WHAT’S NEXT?Length-of-stay management has become intertwined within generalorganizational performance at Allina. With the access to data and thedeveloped infrastructure, LOS optimization has moved into ongoingsupport stages. Data continues to be used to identify opportunities,monitor current performance, and prioritize efforts. Additionally,the values used to calculate performance to GMLOS are updatedannually based off of the updated CMS values released in the fourthquarter of the year. Annually updating these values helps Allina tounderstand and put national performance changes into context.REFERENCES1.Copyright 2017 Health CatalystAgency for Healthcare Research and Quality. (2014, October). Overview ofHospital Stays in the United States, 2012. Retrieved from 80-Hospitalizations-United-States-2012.pdf9
ABOUT HEALTH CATALYST Health Catalyst is a mission-driven data warehousing, analytics,and outcomes improvement company that helps healthcareorganizations of all sizes perform the clinical, financial, andoperational reporting and analysis needed for population healthand accountable care. Our proven enterprise data warehouse(EDW) and analytics platform helps improve quality, add efficiencyand lower costs in support of more than 50 million patients fororganizations ranging from the largest US health system toforward-thinking physician practices.For more information, visit www.healthcatalyst.com, and follow uson Twitter, LinkedIn, and Facebook.Copyright 2017 Health Catalyst
Late-Binding Data Warehouse Health Catalyst Analytics Platform. SERVICES. Installation Services Professional Services. EXECUTIVE SUMMARY. Like most large healthcare systems throughout the country, Allina Health's financial health improves dramatically by optimizing . inpatient care for the patients it serves.