Transcription
11/2/2018The Advanced Practice Providerin ObservationBy Carla Chipalkatty, MS, PA-C,Assistant Medical Director of ObservationBrigham and Women’s HospitalEmergency DepartmentNovember 1, 20181
11/2/2018Disclosure I have no actual or potential conflict of interestin relation to this presentation.The Successful APP-Run UnitStaffingAPP LeadershipQualityAssessmentBeyond TypicalED ManagementCustomerService2
11/2/2018Observation at BWHProtocols at BWH Abdominal PainAllergic ReactionAsthma/COPDAtrial Fibrillation and FlutterBack PainCellulitisChest painCHFDVTDehydration/hyperemesisFebrile NeutropeniaFlank Pain(Pyelonephritis/Urolithiasis) General ComplaintHeadacheMetabolic DerangementMild Traumatic Brain InjuryPneumoniaPsychiatric EmergencyPESocial InterventionsSyncopeTransfusionTIA/StrokeGI BleedHyperglycemia/Hypoglycemia3
11/2/2018Protocols at BWHFrequency of use (2017)Generic Protocol26%LEFT BLANK5%Psychiatric Illness12%Abdominal Pain7%Neuro Eval (Stroke/TIA)10%Chest Pain11%Protocols at BWHFrequency of use (2017)Generic Protocol26%LEFT BLANK5%Psychiatric Illness12%Abdominal Pain7%Neuro Eval (Stroke/TIA)10%Chest Pain11%4
11/2/2018Protocols at BWHUsed for:SBOSeizureFeverPICC line issueNon-operative hip fxGoutCrohn’s flareAnd many moreStaffingBetter call thebackline for aSTAT read so Ican dischargethis one ASAPSure, I’d be happyto call yourbrother, sister andcousin (who is adoctor) to updatethem too My patient inroom 2 islooking septicLet’s checkvitals andstart fluids5
tientmedicineStaffingAdvanced Practice igh patientsatisfactionratesGrowingprofessionAAPA: PA Salary ReportUS Department of LaborCapstack, et al.Paradise, et al.6
11/2/2018Staffing 12 hour APP shifts Rotate– ED– Urgent care– Observation Experiencedprovider in OUStaffing: New Hire TrainingExperienced APP 4 weeks ED training shifts 4 OU training shifts Solo OU shift after 6 monthsNew Graduate APP 6 weeks ED training shifts6 OU training shiftsSolo OU shift after 12 monthsNeeds supportAll new hire APP’s: APP peer mentor program Training checklist Topic review7
11/2/2018StaffingHow can weprevent this?StaffingDedicatedOU staffRotatingED staff Familiarity Perspective8
11/2/2018Staffing: Rounding ModelsDownstairs ED OU:12th Floor OU:12 hour APP coverage24 hour APP coverage10 Beds10 BedsLocated in EDLocated on 12th floorShared case managerDedicated case managerLOS 14 hoursLOS 20 hours13 patients/day8 patients/dayPsychNo behavioral healthStaffing : Rounding ModelsDownstairs ED OU:12th Floor OU:12 hour APP coverage24 hour APP coverage11AM-11PM APP6:30AM-6:30PM APP-Resident/Attendingrounds 6:30AM-APP/Attendingrounds 6:30AMED ResidentCoverage OvernightImprovingcommunication: Verbal handoff Writtenhandoff6:30PM-6:30AM APP Attendingcheck in9
11/2/2018Beyond Typical ED ManagementLonger LOS extra time for value added careLonger LOS inpatient-like issues ariseBeyond Typical ED Management10
11/2/2018Beyond Typical ED ntVTEProphylaxisBeyond Typical ED ManagementMedicationReconciliationActive medication management Who does it? Pharmacies can help Special considerations Metformin and beta blockers inchest pain AKILindenauer, et al.11
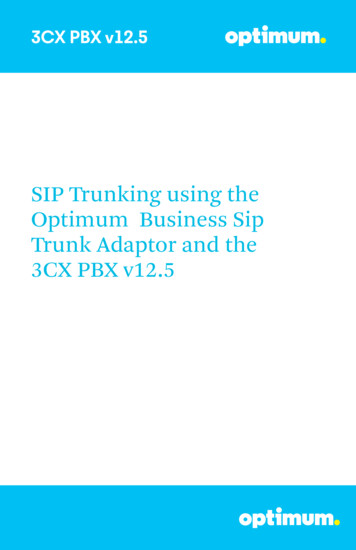
11/2/2018Beyond Typical ED ManagementMake a referenceguideDiabetesManagement Order short acting insulinfor diabetics Check glucose Beware: steroid inducedhyperglycemia New onset diabetes anddischargeBeyond Typical ED ManagementCommon Insulin Conversions Levemir (insulin detemir) Lantus (insulin glargine) 1:1 NPH Lantus (insulin glargine) 2:1 Humalog (Insulin lispro) Novolog (insulin aspart) 1:1 Humulin/Novolin (Regular human insulin) Novolog (insulin aspart) 1:1 Novolin Mix 70/30 calculate units as 70% NPH and 30% insulin aspartLong acting insulin duration NPH 12hrs typically dosed BID Lantus (Insulin glargine) 24hrs typically dosed QDShort acting insulin duration Aspart 3-5 hours (good if patient eating) typically dosed qAC and qHS Regular insulin 5-8 hours (good if pt NPO) typically dosed q6hrBrandGenericNovologInsulin AspartHumalogInsulin lisproHumulin/NovolinRegular human insulin (aka Regular insulin)LantusInsulin glargineLevemirInsulin detemir12
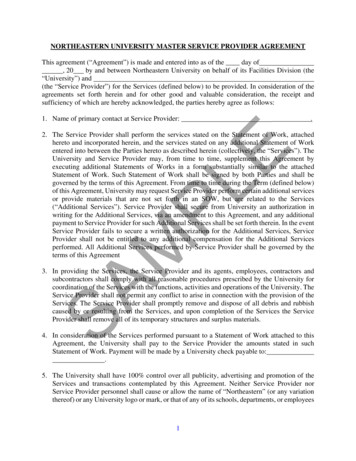
11/2/2018Beyond Typical ED ManagementDiabetes DischargeInsurancePreferred MeterBCBS of MAOne TouchCaremark (CVS)One TouchCommonwealth of MA (Unicare SateIndemnity Plans)One TouchExpress Scripts National PreferredFormularyOne TouchFallon Community Health PlanOne TouchHarvard Pilgrim Health PlanFreeStyleMA Medicaid (MassHealth)FreeStyleMedicare (Part B)FreeStyleTufts Health PlanOne TouchGLUCOMETER SELECTION: **Please discuss with case management before orderingOrder Test Strips and Lancets associated with meter (freestyle or one touch)QID testing (120/month supply)ORDERING LANTUS:Lantus PEN – **Please check with case management, not covered by all insurancesLantus VIAL – ** Alternative if pens not coveredGive instructions for endocrine follow up: 617-732-5666Insulin glargine (Lantus Solostar Pen 100unit/mL)# units SC freqDisp: 5 pensRefills: 3Insulin needles (disposable) 32 x 5/32”Disp: 100 needlesRefills: 3Insulin glargine (Lantus 100unit/mL)# units SC freqDisp: 3 vialsRefills: 3Insulin syringe-needle U-100 1mL 31x15/64”Disp: 100 syringesRefills: 3Beyond Typical ED ManagementPadua Prediction Score for Risk of VTEBaseline featuresScoreActive cancer*Previous VTE (with the exclusion of superficial veinthrombosis)†Reduced mobility‡Already known thrombophilic condition33Recent ( 1 month) trauma and/or surgery2Elderly age ( 70 years)Heart and/or respiratory failureAcute myocardial infarction or ischemic stroke111Acute infection and/or rheumatologic disorder1Obesity (BMI 30)Ongoing hormonal treatment1133Score 4 is high risk:AnticoagulateVTEProphylaxisScore 4 or staying 24 hours: mechanicalprophylaxis*Patients with local or distant metastases and/or in whom chemotherapy or†radiotherapy had been performed in the previous 6 months. Bedrest withbathroom privileges (either due to patient’s limitations or on physicians order)‡for at least 3 days. Carriage of defects of antithrombin, protein C or S, factor VLeiden, G20210A prothrombin mutation, antiphospholipid syndrome.Barbar, et al.13
11/2/2018Customer ServiceNavigating the intersection of patient expectationswith specialty service expectationsTiming of testingand resultsBacklines forreading roomsWeekend andholiday scheduleConsultantavailabilityCustomer ServiceDisposition planning Case management Physical therapy Social work Patient relations(complaints department)Can you come backtomorrow? Maybethen I’ll be ready togo home 14
11/2/2018Quality Assessment Peer submitted case review Review the data Steering committeeQuality AssessmentUse caution with diagnosis with no specific, easyto identify endpoint15
11/2/2018APP LeaderJob description:Front lineCreates relationshipsFacilitates trainingManages complaintsAPP Leadership Structure DirectorChiefPA-IPA-II– 5% salary increase– APP education and professional development– Annual renewal PA-III––––4% salary increaseAdministrative time (typically 4-8hrs/week)Administrative callObservation, urgent care, IT, new hire training 5000 spot bonus for CAQ Annual bonus16
11/2/2018Summary Recruit experienced APP’sIdeal staff rotatesHave anchor APP staffAnticipate inpatient-like issuesSupport your current staff with educationCreate “cheat sheets”Manage patient expectationsCase managers and social workers remove barriers todischarge Encourage staff feedback Chose a diagnosis with an endpoint Create APP leadership opportunity with obsQuestions?ThisEmail me: cchipalkatty@bwh.harvard.eduThis Photo by Unknown Author is licensed under CC BY-NC17
11/2/2018References Ross MA, Hockenberry JM, Mutter R, Barrett M, Wheatley M, Pitts SR. Protocol-driven emergency departmentobservation units offer savings, shorter stays, and reduced admissions. Health affairs. 2013 Dec 1;32(12):2149-56.Conley J, Bohan JS, Baugh CW. The Establishment and Management of an Observation Unit. Emergency Medicine Clinicsof North America. 2017 Aug 31;35(3):519-33.2016 AAPA Salary Report. American Academy of Physician Assistants.United States Department of Labor: Bureau of Labor Statistics: ants.htm#tab-6. Accessed October 29,2018United States Department of Labor: Bureau of Labor Statistics: ts-nurse-midwives-and-nurse-practitioners.htm. Accessed October 29, 2018Capstack TM, Segujja C, Vollono LM, Moser JD, Meisenberg BR, Michtalik HJ. A comparison of conventional andexpanded physician assistant hospitalist staffing models at a community hospital. Journal of Clinical OutcomesManagement. 2016 Oct 1;23(10):455-61.Paradise J, Dark C, Bitler N. Improving access to adult primary care in Medicaid: Exploring the potential role of nursepractitioners and physician assistants. Henry J. Kaiser Family Foundation; 2011.Nurse Journal: ractitioner-salary-statistics/. Accessed Sept 1, 2017Blue Cross Blue Shield of Massachusetts: connect/67462dc45fab-4988-a66e-348020c69353/PA PA-PCP Billing Guidelines.pdf?MOD AJPERES. Accessed Sept 1, 2017.Lindenauer PK, Shieh MS, Pekow PS, Stefan MS. Use and outcomes associated with long-acting bronchodilators amongpatients hospitalized for chronic obstructive pulmonary disease. Annals of the American Thoracic Society. 2014Oct;11(8):1186-94Barbar S, Noventa F, Rossetto V, Ferrari A, Brandolin B, Perlati M, De Bon E, Tormene D, Pagnan A, Prandoni P. A riskassessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: thePadua Prediction Score. Journal of Thrombosis and Haemostasis. 2010 Nov 1;8(11):2450-7.Department of Health and Human Services: Office of Inspector General: . Accessed August 10, 201718
ORDERING LANTUS: Lantus PEN -**Please check with case management, not covered by all insurances Lantus VIAL -** Alternative if pens not covered Give instructions for endocrine follow up: 617-732-5666 Diabetes Discharge Beyond Typical ED Management VTE Prophylaxis Padua Prediction Score for Risk of VTE Baseline features Score Active cancer* 3