Transcription
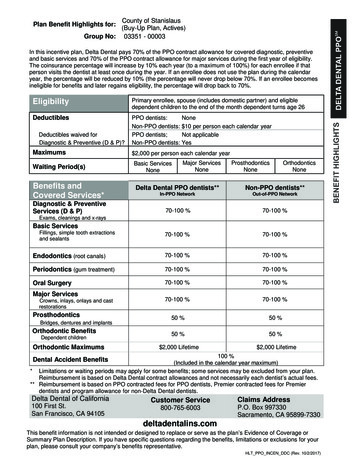
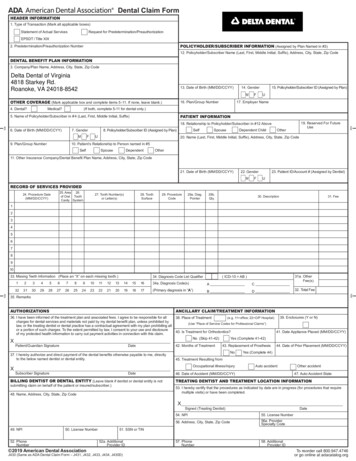
Dental Claim FormHEADER INFORMATION1. Type of Transaction (Mark all applicable boxes)Statement of Actual ServicesRequest for Predetermination/PreauthorizationEPSDT / Title XIXPOLICYHOLDER/SUBSCRIBER INFORMATION (Assigned by Plan Named in #3)2. Predetermination/Preauthorization Number12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip CodeDENTAL BENEFIT PLAN INFORMATION3. Company/Plan Name, Address, City, State, Zip CodeDelta Dental of Virginia4818 Starkey Rd.Roanoke, VA 24018-854213. Date of Birth (MM/DD/CCYY)MOTHER COVERAGE (Mark applicable box and complete items 5 -11. If none, leave blank.)Medical?4. Dental?16. Plan/Group Number15. Policyholder/Subscriber ID (Assigned by Plan)14. GenderFU17. Employer Name(If both, complete 5-11 for dental only.)PATIENT INFORMATION5. Name of Policyholder/Subscriber in # 4 (Last, First, Middle Initial, Suffix)fold7. Gender9. Plan/Group Number10. Patient’s Relationship to Person named in #5MSelfUFSelfSpouseDependent ChildOtherfold19. Reserved For FutureUse18. Relationship to Policyholder/Subscriber in #12 Above8. Policyholder/Subscriber ID (Assigned by Plan)6. Date of Birth (MM/DD/CCYY)20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip CodeSpouseDependentOther11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code21. Date of Birth (MM/DD/CCYY)22. GenderMF23. Patient ID/Account # (Assigned by Dentist)URECORD OF SERVICES PROVIDED25. Area 26.of Oral ToothCavity System24. Procedure Date(MM/DD/CCYY)27. Tooth Number(s)or Letter(s)28. ToothSurface29. ProcedureCode29a. Diag.Pointer29b.Qty.30. Description31. Fee1234567891034. Diagnosis Code List Qualifier( ICD-10 AB )1234567891011121314151634a. Diagnosis Code(s)AC32313029282726252423222120191817(Primary diagnosis in “A”)BD31a. OtherFee(s)32. Total Feefoldfold33. Missing Teeth Information (Place an “X” on each missing tooth.)35. RemarksAUTHORIZATIONSANCILLARY CLAIM/TREATMENT INFORMATION36. I have been informed of the treatment plan and associated fees. I agree to be responsible for allcharges for dental services and materials not paid by my dental benefit plan, unless prohibited bylaw, or the treating dentist or dental practice has a contractual agreement with my plan prohibiting allor a portion of such charges. To the extent permitted by law, I consent to your use and disclosureof my protected health information to carry out payment activities in connection with this claim.38. Place of TreatmentXPatient/Guardian SignatureDate37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directlyto the below named dentist or dental entity.XSubscriber SignatureDateBILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is notsubmitting claim on behalf of the patient or insured/subscriber.)n39. Enclosures (Y or N)(e.g. 11 office; 22 O/P Hospital)(Use “Place of Service Codes for Professional Claims”)40. Is Treatment for Orthodontics?No (Skip 41-42)42. Months of Treatment41. Date Appliance Placed (MM/DD/CCYY)Yes (Complete 41-42)43. Replacement of ProsthesisNo44. Date of Prior Placement (MM/DD/CCYY)Yes (Complete 44)45. Treatment Resulting fromOccupational illness/injuryAuto accident46. Date of Accident (MM/DD/CCYY)Other accident47. Auto Accident StateTREATING DENTIST AND TREATMENT LOCATION INFORMATION53. I hereby certify that the procedures as indicated by date are in progress (for procedures that requiremultiple visits) or have been completed.48. Name, Address, City, State, Zip CodeXSigned (Treating Dentist)49. NPI50. License Number52. PhoneNumber 2019 American Dental AssociationDate54. NPI55. License Number56. Address, City, State, Zip Code56a. ProviderSpecialty Code57. PhoneNumber58. AdditionalProvider ID51. SSN or TIN52a. AdditionalProvider IDJ430 (Same as ADA Dental Claim Form – J431, J432, J433, J434, J430D)To reorder call 800.947.4746or go online at adacatalog.org
The following information highlights certain form completion instructions. Comprehensive ADA Dental Claim Form completion instructionsare posted on the ADA’s web site l-claim-form).GENERAL INSTRUCTIONSA. The form is designed so that the name and address (Item 3) of the third-party payer receiving the claim (insurance company/dentalbenefit plan) is visible in a standard #9 window envelope (window to the left). Please fold the form using the ‘tick-marks’ printedin the margin.B. Complete all items unless noted otherwise on the form or in the instructions posted on the ADA's web site (ADA.org).C. Enter the full name of an individual or a full business name, address and zip code when a name and address field is required.D. All dates must include the four-digit year.E. If the number of procedures reported exceeds the number of lines available on one claim form, list the remaining procedures ona separate, fully completed claim form.F. GENDER Codes (Items 7, 14 and 22) – M Male; F Female; U UnknownCOORDINATION OF BENEFITS (COB)When a claim is being submitted to the secondary payer, complete the entire form and attach the primary payer’s Explanation of Benefits(EOB) showing the amount paid by the primary payer. You may also note the primary carrier paid amount in the “Remarks” field (Item 35).DIAGNOSIS CODINGThe form supports reporting up to four diagnosis codes per dental procedure. This information is required when the diagnosis may affectclaim adjudication when specific dental procedures may minimize the risks associated with the connection between the patient’s oraland systemic health conditions. Diagnosis codes are linked to procedures using the following fields:Item 29a – Diagnosis Code Pointer (“A” through “D” as applicable from Item 34a)Item 34 – Diagnosis Code List Qualifier (AB for ICD-10-CM)Item 34a – Diagnosis Code(s) / A, B, C, D (up to four, with the primary adjacent to the letter “A”)PLACE OF TREATMENTEnter the 2-digit Place of Service Code for Professional Claims, a HIPAA standard maintained by the Centers for Medicare and MedicaidServices. Frequently used codes are:11 Office; 12 Home; 21 Inpatient Hospital; 22 Outpatient Hospital; 31 Skilled Nursing Facility; 32 Nursing FacilityThe full list is available online -POS-database.pdfPROVIDER SPECIALTYThis code is entered in Item 56a and indicates the type of dental professional who delivered the treatment. The general code listed as“Dentist” may be used instead of any of the other codes.Category / Description CodeDentist A dentist is a person qualified by a doctorate in dental surgery (D.D.S.)or dental medicine (D.M.D.) licensed by the state to practice dentistry,and practicing within the scope of that license.General PracticeDental Specialty (see following list)Code122300000X1223G0001XVariousDental Public 223X0400XPediatric ntics1223P0700XOral & Maxillofacial Pathology1223P0106XOral & Maxillofacial Radiology1223D0008XOral & Maxillofacial Surgery1223S0112XProvider taxonomy codes listed above are a subset of the full code set that is posted thcare/health-care-provider-taxonomy-code-set/
Notice of Nondiscrimination and Accessibility PolicyDelta Dental of Virginia complies with applicable Federal civil rights laws and does not discriminate on the basis ofrace, color, national origin, age, disability, or sex. Delta Dental of Virginia does not exclude people or treat themdifferently because of race, color, national origin, age, disability, or sex.Delta Dental of Virginia: Provides free aids and services to people with disabilities to communicate effectively with us, such as: Qualified sign language interpreters Written information in other formats (large print, audio, accessible electronic formats, other formats) Provides free language services to people whose primary language is not English, such as: Qualified interpreters Information written in other languagesIf you need these services, contact Civil Rights Coordinator.If you believe that Delta Dental of Virginia has failed to provide these services or discriminated in another way onthe basis of race, color, national origin, age, disability, or sex, you can file a grievance with:Civil Rights CoordinatorATTN: Compliance Dept.4818 Starkey RoadRoanoke, VA 24018-8542Phone: 1-800-237-6060TTYnumber : 1-877-287-9039, 540-491-9714Email: Compliance@corvesta.comYou can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, Civil Rights Coordinatoris available to help you.You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rightselectronically through the Office for Civil Rights Complaint Portal, available r by mail or phone at:U. S. Department of Health and Human Services200 Independence Avenue, SWRoom 509F, HHH BuildingWashington, D. C. 20201Phone: 1-800-368-1019Hearing Impaired: 1-800-537-7697 (TDD)Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llameal 1-800-237-6060 (TTY: 1-877-287-9039).ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги перевода.Звоните 1-800-237-6060 (телетайп: 1-877-287-9039).CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn. Gọi số 1-800237-6060 (TTY: 致電 1-800-237-6060(TTY:1877-287-9039)。 (رقم 800-237-6060-1 اتصل برقم . فإن خدمات المساعدة اللغوية تتوافر لك بالمجان ، إذا كنت تتحدث اذكر اللغة : ملحوظة .)9039-287-877-1 : هاتف الصم والبكم PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng mga serbisyo ng tulong sa wikanang walang bayad. Tumawag sa 1-800-237-6060 (TTY: 1-877-287-9039). تسهیالت زبانی بصورت رایگان برای شما ، اگر به زبان فارسی گفتگو می کنید : توجه . تماس بگیرید 1-800-237-6060 (TTY: 1-877-287-9039) با . فراهم می باشد ማስታወሻ: የሚናገሩት ቋንቋ ኣማርኛ ከሆነ የትርጉም እርዳታ ድርጅቶች፣ በነጻ ሊያግዝዎት ተዘጋጀተዋል፡ ወደ ሚከተለውቁጥር ይደውሉ 1-800-237-6060 (መስማት ለተሳናቸው: 1-877-287-9039). تو آپ کو زبان کی مدد کی خدمات مفت میں دستیاب ہیں ۔ کال ، اگر آپ اردو بولتے ہیں : خبردار 1-800-237-6060 (TTY: 1-877-287-9039). کريں
ATTENTION : Si vous parlez français, des services d'aide linguistique vous sont proposés gratuitement.Appelez le 1-800-237-6060 (ATS : 1-877-287-9039).ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги перевода.Звоните 1-800-237-6060 (телетайп: 1-877-287-9039).ध्यान दें: यदद आप ह िं दी बोलते हैं तो आपके ललए मुफ्त में भाषा सहायता सेवाएं उपलब्ध हैं। 1-800-237-6060 (TTY:1-877-287-9039) पर कॉल करें ।ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachliche Hilfsdienstleistungen zurVerfügung. Rufnummer: 1-800-237-6060 (TTY: 1-877-287-9039).লক্ষ্য করুনঃ যদি আপনি বাংলা, কথা বলতে পারেন, তাহলে নিঃখরচায় ভাষা সহায়তা পরিষেবাউপলব্ধ আছে। ফোন করুন ১-800-237-6060 (TTY: ১-877-287-9039)।Ige nti: O buru na asu Ibo asusu, enyemaka diri gi site na call 1-800-237-6060 (TTY: 1-877287-9039).AKIYESI: Ti o ba nso ede Yoruba ofe ni iranlowo lori ede wa fun yin o. E pe ero ibanisoro yi 1800-237-6060 (TTY: 1-877-287-9039).
A dentist is a person qualified by a doctorate in dental surgery (D.D.S.) or dental medicine (D.M.D.) licensed by the state to practice dentistry, and practicing within the scope of that license. 122300000X General Practice 1223G0001X Dental Specialty (see following list) Various Dental Public Health 1223D0001X Endodontics 1223E0200X