Transcription
2020 Poster Presentations
A Mobile Hospice BedroomSandra S. Brown, BSN, RN, CHPN & Charisa J. Parker, BSN, RN, CHPNHouston Methodist Clear Lake HospitalINTRODUCTIONA new trend has emerged and home is now the most common place of death for persons inthe United States. In the acute care setting, we are not always able to transfer patients homefor hospice (Cross & Warraich, 2019). The Palliative Care Team at Houston Methodist ClearLake Hospital (HMCL) cared for 668 seriously ill and end-of-life patients in 2019. Of thosepatients, 170 (25%) were discharged to hospice; 75 (11%) remained at HMCL to receiveinpatient hospice services. The majority of these patients and families would prefer to gohome for hospice but their fragile clinical status kept them in our facility. Research has shownthat “the environment in which end-of-life care is delivered can support or detract from thephysical, psychological, social and spiritual needs of patients, their families, and theircaretakers” (Zadeh, et al., 2018, p. 1018). The initial thought of creating a ‘comfort cart’ forour inpatient hospice patients came through collaboration with our Chief NursingOfficer. After brainstorming, the concept grew from providing a few snacks and magazines tocreating a mobile bedroom with all the comforts of home to our inpatient hospice patients.PURPOSE/AIMSAt HMCL, we do not have a palliative care unit nor do we have a patient room that can beconverted permanently into a home-like palliative care or hospice room. Thinking outsidethe box, we decided to bring the comforts of home to our patients by creating a mobilebedroom for our inpatient hospice patients and families. Our aim was to support the familypresence, promote privacy, balance the patient’s need for privacy with caregiver’s need tomonitor condition, provide direct or indirect access to nature, feed the senses, foster a homelike environment, and control noise among other items.METHODSThe team shopped thoughtfully and responsibly to find “the perfect things” for the room RESULTSThe environmental factors implemented have been shown to improve quality of life and to minimize suffering in end-of-life settings. We have taken the conceptof a home-like environment in a free-standing hospice facility or at home and implemented it in the acute care setting with the advent of our innovative mobilebedroom. This takes our patient-centered care of seriously ill and end-of-life patients to new heights. By “bringing the comforts of home” to our hospicepatients, we compassionately care for our patients and help them die with respect and dignity in an environment that may reduce anxiety, pain and suffering.COSTWe purchased bedding, curtains, and environmentenhancement items to create two Mobile HospiceRooms for under 1,000. All items are cleaned perinfection control policy and bedding is launderedand stored for the next hospice patient experience.One daughter who experienced an inpatient hospice journey at HMCL told us:“My mom said she wanted to go home. I felt so guilty thatI couldn’t get her there.”CONCLUSIONPalliative Care and hospice are uncomfortable areas for many nurses. By providing hospice services inthe acute care setting, our staff on the Acute Care Units find themselves delivering care to patients andfamilies on inpatient hospice at times. The research by Zadeh, et al. found that home-like end-of-lifesettings can increase caregiver satisfaction, caregivers’ opinion of the patient, and caregivers’ ability toconnect to the patient as an individual. Our innovative mobile bedroom may also make the hospiceencounter more satisfying and fulfilling for our staff.By “bringing the comforts of home” to our hospice patients, the Palliative Care Team exudesCOMPASSION; we strive to fulfill the wish of many patients of going home for their final journey. Wecare for our patients and help them die with RESPECT and dignity by providing a home-likeenvironment that may reduce anxiety, pain, and suffering. We provide EXCELLENT care and implementinnovations such as our mobile bedroom in an effort to be a model for others in the Palliative Carecommunity to emulate.To support the family presence at the bedside, we purchased snacks and personal care supplies so family will not need to leave thehospital. Evidence has shown that having family present at end of life can reduce patient suffering, aid in closure, increase peace ofmind, and increase caregiver satisfaction (Zadeh et al., 2018).To provide indirect access to nature, we purchased a machine that delivers various nature sounds. Evidence has shown that direct orindirect exposure to nature can reduce patient stress, reduce perception of pain, and enhance a sense of peace (Zadeh et al., 2018).To feed the senses, we purchased soothing artwork, battery operated candles for soft lighting, and a diffuser to deliver aromatherapy. Evidence has shown that environmental interventions that provide access to artwork, music, and aromas can reduceanxiety, lessen perception of pain, and promote tranquility (Zadeh et al., 2018).To foster a home-like environment, we purchased a bedspread and throw blankets in soft colors and a frame with white curtains tohide the medical equipment above the headboard. Evidence has shown that home-like settings can reduce suffering, increasecomfort, and increase patient and family satisfaction (Zadeh et al., 2018).To provide privacy and to control noise, we will work with bed control and the Operations Administrator to move patients oninpatient hospice to a larger room at the end of the hall. We will place a sign on the door that will alert staff that the patient is onhospice. Evidence has shown that providing privacy helps to reduce stress, allows for dignity at end-of-life, and promotes healthygrieving for patients and families (Zadeh et al., 2018).REFERENCES/ACKNOWLEDGEMENTSCross, S. H. & Warraich, H. J. (2019). The New England Journal of Medicine, 381(24),2369-2370.Zadeh, R. S., Eshelman, P., Setla, J., Kennedy, L., Hon, E., & Basara, A. (2018). Journalof Pain Symptom Management, 55(3), 2017.09.011The Palliative Care Team would like to acknowledge nursing leadership at HMCL for theircontinued support and investment in our success.
EDUCATIONAL STRATEGY USING VIRTUAL SIMULATION TOHELP STUDENTS RECOMMEND PALLIATIVE/HOSPICE CAREDiane F. Smith, DNP, FNP, RNBON SECOURS MEMORIAL COLLEGE OF NURSING, RICHMOND, VIRGINIARESULTSINTRODUCTIONBackground Patients are being referred late or not at all to palliative or hospice care. The timing of patient consults occurs on the average of 37 days beforedeath; hospice care begins 20 days before death. Nursing students and seasoned nurses are not familiar with palliative orhospice care and/or feel uncomfortable about discussing end of life care. The nurses’ ability to work within the inter-professional palliative/ hospiceteams is needed to recommend appropriate, timelier referrals that result incompassionate care.CONCLUSIONS Virtual simulation was 100% student positive in its first offering. The students’ video responses demonstrated elements of the inter-professional team concept to advocate for future seriously ill patients. 100% of students identified patients that could be referred to palliative care/hospiceThe overall Learner satisfactionWas the simulation scenario realisticenough for me to engage, as if witha live patient?100%80% agree100%student satisfaction ofcourse100%of students identifiedpatients that could bereferred to palliativecare/hospiceDid the simulation scenario supporta realistic patient environment?87% agreeVideo 1: SBAR Report to StudentsREFERENCES/ACKNOWLEDGEMENTS1. Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. (1991). The Edmonton SymptomAssessment System (ESAS): a simple method for the assessment of palliative care patients.Journal of Palliative Care. 7:6-9.MATERIALS & METHODSDid the scenario demonstrateelements of the inter-professionalteam concept that will help advocatefor the seriously ill patients and theirfamilies for palliative care?Educational Innovation A virtual SBAR simulation was created for students to learn more aboutpalliative/hospice nursing care The simulation provides a safe online context Students practice their ability to appropriately refer patients topalliative/hospice careObjectives1. Apply SBAR to recognize symptoms in serious illness2. Create a mock phone call to practice advocating for palliative care.Methods 15 students volunteered to complete the course content over 15 weeks Each student participated in a virtual simulation consisting of: twovideos, discussion board debriefing, a post-reflection. Each student created a video to demonstrate their ability to advocate forpalliative care by a mock phone call to a virtual provider. This online virtual simulation could be used as a best practice model forother vulnerable populations and enhance nursing education and practice. Future educational research could be conducted to: determine knowledge gained apply the SBAR to practice situations improve clinical outcomes in the workplace.Video 2: Patient – Nurse InteractionDid the scenario advocate forthe need of palliative care forseriously ill patients and theirfamilies, from the time of diagnosis,as essential to quality care and anintegral component of nursing care?80% agree2 Cloud, J. (2000). A kinder, gentler death. Time: CNN Poll. Retrieved from:http://content.time.com/time/magazine/ article/0,9171,997968,00.html3 Gomes, B., Calanzani, N., Gysels, M., Hall, S, & Higginson, I. J. (2013). Heterogeneity andchanges in preferences for dying at home: A systematic review. BMC Palliative Care, 12(1),7-19. doi:10.1186/1472-684X-12-7.80% agree4 Herr, K., Titler, M., Fine, P., Sanders, S., Cavanaugh, J., Swegle, J., & Tang, X. (2010).Assessing and Treating Pain in Hospices: Current State of Evidence-Based Practices.Journal of Pain & Symptom Management, 39(5), 803-819.doi:10.1016/j.jpainsymman.2009.09.0255 Holdsworth, L., & King, A. (2011). Preferences for end of life: views of hospice patients,family careers, and community nurse specialists. International Journal of Palliative Nursing,17(5), 251-255.
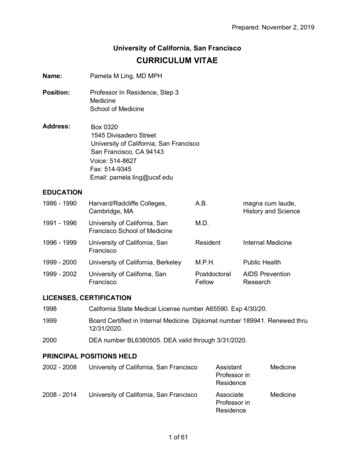
Gentle Yoga as an Integrative Modality for Chronic Pain in Adult Cancer Patients1Frier ,2Quinlin ,Kimberly ADNP, FNP-BC, APRN-CNP, ACHPN, LindaDNP, ANCS-BC, APRN-CNP, ACHPN,Brenda Buffington2, EdD, NBC-HWC, EP-C, Susan E. Thrane2, PhD, RN, CHPN1OhioState University Wexner Medical Center, 2Ohio State University College of NursingINTRODUCTIONChanges in opioid dispensing and prescribing have revised guidelinesfor managing chronic pain in adult cancer patients. Recommendations promotereduced opioids and use of integrative modalities for pain management. Gentleyoga (breathing, meditation and gentle stretching exercises) is associated withimproved emotional well-being, anxiety, sleep disturbances, fatigue andmusculoskeletal symptoms associated with aromatase inhibitors,chemotherapy and radiation. The American College of Sports Medicine(ACSM) guidelines conclude ample evidence for physical activity before,during and after cancer treatment.PURPOSEIn collaboration with clinicians from the outpatient Palliative MedicineClinic, this initiative developed and implemented a gentle yoga CPG topromote a formal evidence-based recommendation for gentle yoga andevaluated patient adherence with yoga class attendance in adult cancer patientsas part of a comprehensive pain and symptom management plan.METHODS EMR custom medication gentle yoga exercise prescription, signed byprescribing clinician. Patient education folder handout included class tracking cards, localcommunity yoga class handouts, a home practice handout and signedexercise prescription. Patient tracking and demographic data was collected and documented by adata broker via Excel spreadsheet. Cancer Data Analytics queried custom medication EMR data andaggregated clinician & patient data for graphic presentation.InclusionCriteriaAdults older than18 years of ageStable able,Number ofprogressiveclasses attendeddisease, acuteper participant.symptomatologyClinicianOutcomeNum. of custommed/exerciseprescriptions perprovider.28*Not currentlypracticing gentleyogaFollow-up inclinic duringand aftercompletionBaseline:CustommedicationEMR 10/1/19 –1/31/19Clinician OutcomeSpecial Orders Total by Type18N 18(75%)*2 patients left clinic and 2 prescriptionsgiven at the end of the project period.Patient outcomes reported on 24 patients.Average Number of Classes Per patient**Only patients who attended classesFemale9 classesMale10 classesGentleYoga28AllOthers51N 6(25%)1 Classes1 ClassGentle Yoga Orders PerProvider TypeAll Other Special OrdersBy Provider TypeNo classesNo ClassesPatient Count by RaceNPWhite79.2%(n 19)Black20.8%(n 5)MDNPMDNPMDPatient Reflections Participants reflected enjoyment, enhanced social interaction,reduced pain and new learning without long term plans tocontinue community classes. One participant expressed that the gentle yoga stretches havereally helped his neck and “makes me feel good about myself.”He also stated, “It’s something I need in my life right now.”Patient Count by SexFemale, 54.2% (n 13)Mean Age 56 yearsMale, 45.8% (n 11)Mean Age 50 years 26 Palliative Medicine Clinic outpatients (13 men/13 women) with chroniccancer pain were offered a formal recommendation for gentle yoga. Diagnoses included breast, ovarian, lung, head/neck, and rectal/anal cancers. Patients were white (70%) and 30-69 years of age. 6/24 patients actively participated in gentle yoga classes. 6 participants (5 male) completed a mean of 10 gentle yoga classes. Two patients were lost to follow-up. Most of the exercise prescriptions were prescribed by NPs (97%).CONCLUSIONS6Sex, Race, AgeCancerdiagnosisTracking cards: Clinician education Trial period:12 classes/12at monthly meeting October 1,weeks with2019-Januaryinstructor initial31, 2020& dateCreated smartphrases for EMRcustom medication.Educatedclinicians.Total # Patients Given GentleYoga PrescriptionsPatients Who Attended1 or more classesDemographicsChronicCurrentlymalignant or non- practicing gentlemalignant painyogaNot released forexercise by theironcologist orsurgeonPatient OutcomesRESULTS SUMMARYRESULTS Another participant felt that the chair yoga taught him stretchesto do at work that are helpful, that his balance has improved,that he likes the mindfulness, focus and stress relief, and thatmore men should try yoga. Women not participating reflected transportation issues, waitingon family or friend to participate, and ongoing illness.Adult cancer patients with chronic pain can benefit from gentle yoga.Encouraging cancer participation in gentle yoga with a written evidence-basedrecommendation using a custom medication was successful for six patients.Men may be willing to participate in gentle yoga if encouraged. Ongoingencouragement is necessary to overcome individual patient barriers such asfinances, transportation, and disease progression or morbidity. Diseaseprogression and morbidity requires re-evaluation of appropriateness forparticipation in exercise.Using the EMR custom medication as a written exercise prescription forgentle yoga participation is a viable process option. Developing a shared smartphrase for clinicians to upload into the free text section of the EMR custommedication is most advantageous for prescribing clinicians. Nurse practitionersare more likely to consider use of a custom medication.LIMITATIONSBARRIERSSmall sample sizePrescribing clinicians not remembering toPopulation disease trajectory of the Palliative offer gentle yoga.Medicine ClinicPromotional laminated 8X11 sign hung at eyelevel at vital sign area encouraged askingclinician about gentle yoga2 Majority holidays, winter limitedRN staff not remembering or knowing toengagement in classesprovide tracking card & patient educationCOVID-19 prevented 12 class completion of materials. Custom medication printed servedpatients engagedas a trigger for RN. Educational folder withtracking card at PCA desk.Bias with majority of recommendationsPatient not attending classes regularly.offered by long term OP prescribing clinician Monthly follow-up in clinic or by telephoneLoyalty may have contributed to maleand allowing completion of 8/12 classes aspredominant participationsuccessful helped for uncontrolled barriers.ACKNOWLEDGEMENTSAcknowledgements: Data Broker: Monique Brown, PCA; Data Analyst: Dania Ahmed, MPH;Preceptors: Dori Klemanski, DNP, APRN-CNP, Carol J. Colussi, MHA, RN, NEA-BC, SachinKale, MD and Palliative Medicine Clinic Colleagues
Through the E-Looking Glass:Telesimulation as the New Wonderland for Practicing Palliative ConversationsNicole Generales, BSN, RN, CHPN; Gina Petersen, MSN, RN, CHPN, CHSE; Jeffrey Collins BSN, RN,CCRNRESULTSINTRODUCTIONNurses are in ideal positions to provide quality palliative, including end of life(EOL), care to individuals, which requires advance care planning through aseries of conversations with loved ones and the healthcare team. Lack ofknowledge, discomfort, and system complexity has led to reduced qualityEOL care. While not a new phenomenon (Jeffers, 2020), nurses midpandemic are caring for dying patients at an alarming rate. Theinterdisciplinary Palliative Care Simulation Program (PCSP), developed in2016 to allow licensed nurses to practice discussing palliative care withpatients and families, improved nurses’ self-efficacy for palliative careprovision (Trovato & Generales, 2019). Suspended in-person meetingsbecame an opportunity to adapt the existing PCSP into a iteindividualstousetelecommunication to remotely participate in simulation, an approach tolearning that creates a safe environment to practice skills, such as crucialconversations (McCoy, Sayegh, Alrabah, & Yarris, 2017; Crider & SmithGlasgow, 2019).CONCLUSIONSSeven of nine participants (78%) completed the feedback form. Every participant (100%) agreed or strongly agreed that learning objectives were met, ratedthe course as “Very Good “ or “Excellent,” and agreed or strongly agreed they would use the skills they learned in their clinical practice.The Palliative Care Telesimulation Program is an innovative and effectiveexperience that was very well-received by a sample of nurse residents. Thisnovel transformation of an existing innovation is an exemplar of nursingeducation meeting the ongoing yet immediate needs of new graduate nursesin real-time during the COVID-19 pandemic.Limitations include a small convenience sample, lack of a valid and reliabletool for program evaluation, and technology issues. While access to atelecommunication platform was not a barrier in this pilot, it may be forindividuals in different circumstances.Considerations for the near future include inviting interdisciplinary colleaguesto join the discussion or participate in role play, adapting role play scenariosto meet needs of future participants, selecting a valid and reliable tool forevaluation, and considering this option when in-person education resumes.AIMACKNOWLEDGEMENTSBased on a needs assessment survey completed by nurse residents, thefollowing learning objectives were developed:o Recognize emotions in themselves and others, and navigateconversations using evidence-based communication techniqueso Understand palliative care and its relationship to hospice careo Explore goals of care with patients and families for advance careplanningo Discuss anticipated end of life symptoms, medications, and serviceswith patients and familiesWe would like to thank our colleagues in nursing and simulation education fortheir gracious and unending support:Barbara Flanagan, MSN, RN, CNL, Education Specialist, YNHH GreenwichHospitalCheryl Mayeran, MPH, Simulation Consultant, YNHHSREFERENCESMETHODSThe pilot Palliative Care Telesimulation Program was a 4-hour experienceusing a convenience sample of 9 nurse residents with 1-2 years of acute careexperience. Required prework included the Center to Advance Palliative Care(CAPC; n.d.) module, “An In-Depth Look at Pallaitive Care and its Services.”Nurses and facilitators connected via their organizations’ Zoom account. Theprogram began with a mindfulness moment and 1-2 word emotional check-in,followed by a series of Powerpoint slides, live polls, and role plays. Lecture,prebrief, and debrief occurred in the main Zoom room. Role play occurred infour breakout rooms with 2-3 participants each, moderated by facilitators whoshared adapted VitalTalk (2020) resources via the chat feature.The program was evaluated using the Yale New Haven Health System(YNHHS) SYN:APSE Simulation Feedback form.Historically used in medical and military education, telesimulation is anemerging approach to learning that is applicable and timely.Screenshot of Role Play #2. Image of hospitalized patient credited to Ganz (2005).“WHAT WERE THE MOST HELPFUL ASPECTS OF THE COURSE?”“Helpful tips to facilitate palliativecare conversations, real-lifesimulations to facilitate palliativecare conversations”“Simulation role play #2, getting to act as nurse(practice getting comfortable having difficultconversations with family members) and act assignificant other (understanding how they familymembers feels in that situationand understanding what they need)”“Learning tools to help patients andpeers understand their feelings andcope with difficult situations”“The tools to go back and reviewafterwards. Also the script for end of lifeconversation with family was priceless.Will help so much”CAPC. (n.d.). Tools and training for clinicians: Palliative care programs. Retrieved June 1,2020 from https://www.capc.org/Crider, M. C., & Smith Glasgow, M. E. (2019). Fostering professional developmentinsimulation. In L. Wilson & R. Wittman-Price (Eds.), Review manual for the CertifiedHealthcare Simulation Educator (CHSE ) exam (pp. 267-278). New York, NY:Springer.Ganz, S. (2005, July 1). Hold on. Let go. Retrieved August 10, 2020 23 (Originally photographed 2005, July 1)Jeffers, S. (2020, July 2). Death and dying in a pandemic: Preparing nursesfor end-of-lifecare [Web log post]. Retrieved July 10, 2020, from c-preparing-nurses- for-end-of-life-care/McCoy, C. E., Sayegh, J., Alrabah, R., & Yarris, L. M. (2017). Telesimulation:An innovativetool for health professions education. AEM Education and Training, 1(2), 132-136. doi:10.1002/aet2.10015Trovato, G., & Generales, N. (2019, October 10). Improving nurse resident palliativecareability through simulation. Podium presentation at ANCCNational Magnet Conferencein Orlando, Florida.VitalTalk. (2020) COVID collaborative resources. Retrieved June 1, 2020 rative-resources/
Increasing Patient and Family Satisfaction by ImplementingBedside Handoff Report in a Hospice In-patient UnitAn Evidence Based Practice ProjectLeah Guthrie BSN, RN, CHPNOhio’s HospiceRESULTSINTRODUCTIONCONCLUSIONSA need for increased, more in-depth communication between patients, families, and staffarose at a Southwest Ohio Hospice Inpatient Unit. It was founded that the end of shiftand beginning of shift were problematic areas of concern regarding communication.Based on the evidence Original process: The end-of-shift communication for nurses from the current shift and fromthe oncoming shift would collaborate in the “report” room to discuss patient status and anysignificant clinical and or psychosocial facts that should be shared. While this was taking placein the report room there seemed to be a void on the patient hallways causing confusion, lack ofcontinuity of care, and safety concerns for patients and families.It is recommended that a standardized bedside handoff process be trialed and implemented in allinpatient hospice facilities at Ohio’s Hospice for bedside handoff at shift change.PURPOSE/AIMSMission: Improve workflow and communication between nurses, patients, and families, atshift change. We would initially start by assessing the need in the inpatient unit, sending out asurvey to RN's regarding implementation, assessing patient/ family satisfaction with myrounding tool, trialing implementation prior to start, adjusting process based on previousassessment tools. Also, I would gather literature to help support the need to implement bedsiderounding at shift change.Vision: To improve patient and family satisfaction.Philosophy: Use Evidence Based Practice to provide superior service and care while alsoimproving quality and accountability during shift changes.Step 5 Evaluate The OutcomesEach Ohio’s Hospice facility/ Unit should apply bedside handoff in a way that fits the preferencesof its patients and clinicians while using the evidence to guide the process.Bedside Handoff In A Hospice Inpatient UnitStep 0 Clinical Inquiry:The evidenced based project started byassessing the need for increasedcommunication in the inpatient unit byanalyzing patient satisfaction surveyscores.Step 3 Critical Appraisal and EvidenceTable Keeper Studies established Evidence Table Originated Outcomes Synthesis TableStep 1 PICO:METHODSEvidence Based PracticeP: Terminally Ill PatientsI: Bedside HandoffC: No Bedside HandoffO: Perceived Quality of Nursing CareIn caregivers of terminally ill patients how does bedside handoff report as compared tono bedside handoff report affect perceived quality of nursing care?A PICO question was formed, andresearch was initiated to help guide thecommittee on how to move forward withthe change. Research was evaluated andanalyzed. Stakeholders were establishedand a mission was foundedStep 2 Search Strategies : Databases: Cinahl, PubMed Boolean terms: And, Or Keywords: Handover, Continuity ofcare, Standardized handoff, SBAR,Communication between nursingshifts, Bedside handoff, Bedsidereport, Evidence based practice,patient safety, bedside nursinghandoff, staff accountability, patientsatisfaction, Hospice, Inpatient Unit,NursingExpected Outcomes:Improved/ sustained caregiver satisfaction CAHPS survey scores in 2019 :Inpatient team included caregiver in the decisions (always)Kept informed about when team would arrive (Always)Kept informed about patients' condition (always)Hospice team listened carefully about problems with care (always)Hospice team listened carefully to caregiver (always)Received help as soon as wanted (Always)Patient got as much help with pain as needed (Yes, definitely)Increased patient awarenessReduced fall incidents (in some months)Reduced medication errors (goal).Sustainability planMaintaining positive culture about evidenced based bedside handoff Discuss making Bedside handoff a clinical practice guideline for all OHI inpatient units. Staff Meetings Reinforcing Bedside handoff into staff orientation Educating PreceptorsCreating a clinical practice guideline templateStep 4 Evidenced BasedReccomendationsImplementation Plan Asked staff to trial bedside handoff Staff surveys (pre and postimplementation) Patient survey results during team leaderrounding DEYTA scores Directly asking patients and families ifthey would like to participate in bedsidehandoff. F Followed up with direct question: howdid they like it?REFERENCES/ACKNOWLEDGEMENTS1. Baker, S.J., McGowan, N., (2010). Bedside shift report improves patient safety and nurseaccountability. Journal of Emergency Medicine. 36(4). 355-358.2. Dorvil, B. (2018). The secrets to successful nurse bedside shift report implementation andsustainability. Nursing Management, 49(6), 20-25.3. Ernst, K. M. (2017). Nurse-to-nurse shift handoffs on medical-surgical units: A process within theflow of nursing care. Journal of Clinical Nursing, 27(5-6), e1189-e1201.4. Groves, P.S., Manges, K.A., & Scott-Cawiezell J. (2016). Handing Off Safety at the Bedside.Clinical Nursing Research, 25(5), 473-493. Retrieved from 547738166305355. Maxson, P. M., Derby, K. M., Wrobleski, D. M., & Foss, D. M. (2012). Bedside nurse-to-nursehandoff promotes patient safety. Medsurg Nursing, 21(3), 140‐4; quiz 145.6. Wildner, J. (05). Patient participation in change-of-shift procedures the implementation of thebedside handover for the improvement of nursing quality in an Italian hospice. Journal of Hospiceand Palliative Nursing, 14(3), 216-224.
MEDICATION REDUCTION IN HOSPICE PATIENTS IN LONG-TERM CARETERRI ISAACS, DNP, NP-C, ACHPN & LEE ANN LONG, DNP, RN, CHPNHOSPICE CLEVELAND COUNTYINTERVENTIONSINTRODUCTIONPURPOSE/AIMS Educate long-term care (LTC) facilityproviders/pharmacists regarding evidence ondeprescribing for hospice patients. Conduct regular medication reviews with LTCpharmacist, hospice provider and hospice RN. Make recommendations to providers formedication deprescribing for hospice patientsresiding in LTC. Meet Healthy People 2020 goal of 10%reduction of inappropriate medications fordisabled older adults (U.S. Department of Healthand Human Services [HHS], 2019). Improve quality of life for hospice patientsresiding in LTC. Education of hospice and LTC staff with pre/ post surveys to determine staff perception of comfort inrecognizing polypharmacy, recommending deprescribing and willingness to deprescribe. Weekly use of the MedStopper online tool to provide patient specific deprescribing guidance.www.medstopper.com Weekly rounding with nursing staff to provide support and guidance. Bi-weekly conference with the LTC pharmacist to review medications for deprescribing recommendations. Periodic collaboration with LTC physician and nurse practitioner to assess for barriers to deprescribing.FINDINGSNumber of Medications Medications that do not have current indications orare known to be ineffective, unnecessary, orconsidered duplicate therapy are alsopolypharmacy and problematic in the elderly(Endsley, 2018). Polypha
1Ohio State University Wexner Medical Center, 2Ohio State University College of Nursing ACKNOWLEDGEMENTS Acknowledgements: Data Broker: Monique Brown, PCA; Data Analyst: Dania Ahmed, MPH; Preceptors: Dori Klemanski, DNP, APRN-CNP, Carol J. Colussi, MHA, RN, NEA-BC, Sachin Kale, MD and Palliative Medicine Clinic Colleagues RESULTS SUMMARY