Transcription
ARTICLEEvaluation of Stereo Acuityin Professional Baseball andLPGA Athletes Compared toNon-AthletesTitmus Stereo Test/Wirt Circles. Additionally,to examine the new test for reliability andvalidity.Methods: Participants included professionalbaseball players (PBP; n 265) and professionalwomen golfers (LPGA; n 52), and nonathletes (n 107). All participants were testedon the RightEye Fine Depth Perception (FDP)test and a subset (n 20) was retested todetermine reliability and internal consistency.A different subset (n 81) was tested forvalidity comparing the Titmus Stereo Test/WirtCircles to the RightEye FDP test. Cronbach’sAlpha, intraclass correlation coefficients (ICC)were examined for reliability and ANOVA wasconducted to determine convergent validityas well as differences in stereo acuity betweengroups.Melissa Hunfalvay, PhDRhonda Orr, PhDNicholas P Murray, PhDClaire-Marie Roberts, PhDStatement of Conflict of Interest: 2nd,3rd and 4th authors are independent of thecompany (RightEye, LLC) with no conflicts ofinterest. All analysis and results are conductedby the 2nd, 3rd and 4th authors. All datacollection was conducted independently ofRightEye by experienced vision specialists.The first author works for RightEye as ascientist, is blind to the analysis and follows allethical considerations during the scientific andexperimental process.Results: Results: The test was revealed to havehigh reliability and validity, therefore being agood measure of stereo acuity. Furthermore,significant differences (p .001) betweenathletes and non-athletes were found. Both PBPand LPGA athletes were significantly differentfrom non-athletes (p .05). No differences werefound between athlete groups.ABSTRACTPurpose: To investigate stereo acuity ofprofessional athletes in an open (baseball) andclosed (golf) skilled sport compared to nonathletes using a new digitized version of theCorrespondence regarding this article should beemailed to Melissa Hunfalvay, PhD, at melissa@righteye.com. All state ments are the author’s personalopinion and may not reflect the opinions of theCollege of Optometrists in Vision Development, VisionDevelopment & Rehabili tation or any institu tion ororganization to which the authors may be affiliated.Permission to use reprints of this article must beobtained from the editor. Copyright 2017 College ofOptometrists in Vision Development. VDR is indexed inthe Directory of Open Access Journals. Online access isavailable at www.covd.org.Conclusions: The RightEye FDP test is bothreliable and valid and can therefore be usedconfidently as a measure of static stereoacuity. Elite athletes in open and closed skillsshow significantly better stereo acuity thannon-athletes.Stereopsis is the perception of depth frombinocular retinal disparity.1,2 Stereo acuity,is one important component of stereopsis.Stereo acuity is the smallest detectable depthdifference that can be seen in binocular visionand is critical to human performance as itassists us to see in three dimensions. Stereoacuity is one of the fastest visual depth cues3and plays a major role in anticipation timingskills such as catching a ball.4 Stereo acuityHunfalvay M, Orr R, Murray N, Roberts CM. Evaluationof stereo acuity in professional baseball and LPGAathletes compared to non-athletes. Vision Dev &Rehab 2017;3(1):33-41.Keywords: athletes; fine depth perception;visual performance; LPGA; MLB;Stereo acuity; Titmus 49 Stereo Test;Wirt Stereo TestVision Development & Rehabilitation34Volume 3, Issue 1 April 2017
has also been shown to enhance performanceof fine motor skills such as placing beads ona needle.5 It is critical in both viewing staticobjects (such as a golf ball placed on a tee) aswell as dynamic movement (such as hitting abaseball).6,7As stereo acuity is critical to humanperformance across many different tasks, it begsthe question, is there evidence that athletes,at the highest level of their professions, havebetter stereo acuity than non-athletes? Ifresearch can prove this point, this knowledgemay be transferred to help others achieve thesame high level of stereo acuity through visiontraining. Furthermore, it may be used as onepossible predictor in the development of thenext generations of athletes.To date, research on stereo acuity levels ofathletes compared to non-athletes exists andprovides mixed conclusions. Junior baseball/softball players demonstrated significantlybetter static near stereo acuity using theRandot Stereotest than non–ball players, withcomparable results to professional baseballers.7Distance stereo acuity in major league baseballplayers exceeded that of minor leagueplayers.8 Dynamic stereo acuity measurementswould be more relevant in sports with movingtargets. For example, professional baseballersdemonstrated better dynamic stereo acuitythan inexperienced control participants.9 Ingolf, where static stereo acuity is important,professional golfers showed superior stereoacuity response times, compared with amateurand senior counterparts.10However, evidence to the contrary alsoexits. College baseball players showed nocorrelation between near and distance stereoacuity and batting performance.11 Static stereoacuity assessed between professional andamateur soccer players as well as those withouta soccer background showed no differences.12Similarly, no significant differences wereidentified between youth elite and sub-elitesoccer players in static and dynamic visualacuity or stereoscopic depth sensitivity.13Vision Development & RehabilitationThere may be several reasons why thecurrent body of research seems contradictory.One reason may be the skill levels of athletesfor comparison.11,13 Another may be the ageof the participants which ranges from childrento adults.5 Small sample sizes,12 variationin measurement tools throughout manyexperiments (e.g. Poltavski & Biberdorf,14used Nike SPARQ; Paulus et al.,12 used a 3DTV) and differences between sports (Poltavski& Biberdorf,14 examined ice hockey athletes;Paulus et al.,12 examined soccer players, Labyet al.8 examined baseball players) likely alsocontribute to the differential findings.Sports have many different requirementsthat determine success. One way to differ entiatemotor skills is determining if they are openor closed skills. Open motor skills are thosethat involve a nonstable and unpredictableenvironment where an object or environmentalcontext is in motion and where the performerdetermines when to begin action.15 Closed motorskills are performed in a stable and predictableenvironment where the performer determineswhen to begin the action.15 These motor skillconcepts are on a continuum, meaning it is rareto find a skill that is 100% closed or 100% open.However, fielding in baseball is an open skill.Batting in baseball is also open but less openthan fielding as the pitcher controls the initiationof the pitch requiring the batter to respond.Golf is a more closed skill than baseball as thegolfer can take their time hitting the ball and theball is not in motion. Stereo acuity is importantin both these sports. For baseball, viewing thedistance of position players. For golf, preciselyknowing the depth the ball is from the athleteis important to the biomechanics of the swingpath. It is unclear in the current state of researchif athletes at the highest levels, across varyingdifferent motor skills, all have better stereoacuity compared to non-athletes. Past researchhas limitations in terms of great variation in ageswithin and between groups. Such variation canaffect statistical outcomes.16 Development ofstereopsis and in-turn stereo acuity is thought35Volume 3, Issue 1 April 2017
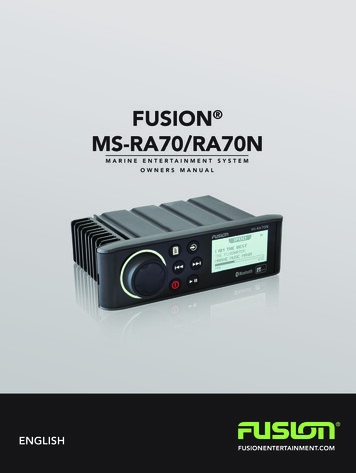
to begin from age 3-5 months,17 mature around7-9 years of age18 and deteriorate from age 40years.19Variation in tools used to measure stereoacuity could be another contributing factorof equivocal results. The variety of testsand limited information on test validity andreliability bring into question the stimuli usedto evaluate stereopsis and therefore the resultsof the studies.To date, in the field of optometry theTitmus Stereo Test/Wirt Stereo Test is the mostwidely used, studied and accepted method ofexamining stereo acuity, specifically near staticstereo acuity.20 This test has been determinedto be unbiased culturally with high testability forall ages.20 The test is based on horizontal retinaldisparity of two images and the identificationof a shape that is apparently closer. The Titmustest is a two-page design with various stimuliat different angles of disparity. The Wirt circlesplaced at each corner of a diamond pattern(repeated nine times) are situated on the upperleft page (see Figure 1).The purpose of this study is to examinedifferences in static stereo acuity using adigitized version of the most widely used staticstereo test in optometry, the Titmus Stereo Test/Wirt circles. Furthermore, this study examinedthe reliability and validity of a new digitizedstatic stereo acuity test: the RightEye Fine DepthPerception test. This study includes adults onlywhose development of stereo acuity should beat its peak. Additionally, this study comparestwo groups of professional athletes and nonathletes, and athletes in an open skilled sport(baseball) are compared to athletes in a closedskill sport (golf) for differences in stereo acuity.Figure 1: Titmus Stereo Test/Wirt Stereo Test bookletthe RightEye database. LPGA participantswere between the ages of 18-31 years (M 24.8, SD 3.5), professional baseball playerswere between the ages of 26-31 years (M 28.1, SD 3.2) and NA participants werebetween the ages of 19-35 years (M 27.1, SD 5.1), 53% were male (n 57) and 47% werefemales (n 50).To test reliability of the digital translationof the Wirt dots, a small subgroup of twentyparticipants was re-tested a second time onthe RightEye Fine Depth Perception (FDP) test.The subgroup included participants of the NAgroup between the ages of 22-33 years (M 26.0, SD 3.8), 50% were male (n 10) and50% were females (n 10).To test validity the Stereo Fly Test (SFT)specifically the nine Stereotest Circles (SC; seeFigure 1) was used on a subgroup of 81 partici pants. The subgroup included participants ofthe NA group (n 40) between the ages of20-34 years (M 26.6, SD 4.8), 45% weremale (n 20) and 55% were females (n 20).The subgroup also included participants ofthe PBP group (n 41). All were minor leagueathletes between the ages of 26-30 years (M 28.2, SD 2.8), all were male.METHODSParticipants52 Ladies Professional Golf Association(LPGA) and 265 professional baseball players(PBP), approximately 40% playing in the MajorLeague (ML) and 107 non-athletes (NA) wereretrospectively obtained for this study throughVision Development & Rehabilitation36Volume 3, Issue 1 April 2017
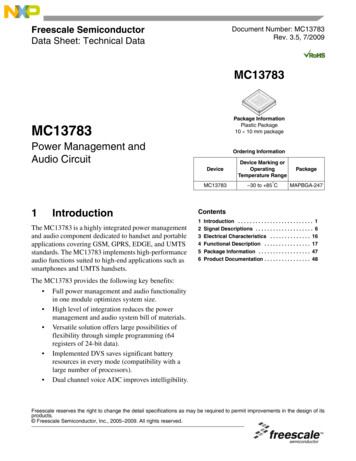
LPGA participants were recruited as part of“The A-Team”, headed by Dr. Don Teig, andincluded a group of sports trained eye careprofessionals. PBP participants are RightEyeclients and testing was conducted by the sportvision doctor for these teams. NA participantswere recruited through advertisements placedon the internet, social media, bulletin boards,and via word of mouth. Testing for the NAgroup was conducted by sport vision specialistsin Maryland. All testers were experiencedsport vision specialists (e.g. optometrists,ophthalmologists) and had received and passedthe RightEye training, education, and protocolprocedures prior to testing.Participants were excluded from partici pation in the study if they met any of thefollowing pre-screening conditions: neuro logicaldisorders (such as concussion, traumatic braininjury, Parkinson’s Disease, Huntington’s Disease,cerebral palsy); vision related issues that preventedsuccessful21,22 calibration of all 9-points (suchas extreme tropias,23 phorias,23,24 static visualacuity of greater than 20/40,21 nystagmus,21,25cataracts26 or eye lash impediments26); smallvessel strokes; consumption of drugs or alcoholwithin 24 hours of testing. All subjects providedinformed consent to participate in this study inaccordance with IRB procedure (IRB: UMCIRB13-002660).then asked to complete the informed consentand demographic information (age, gender,skill level and years playing at a professionallevel) in the RightEye application. Participantswere then seated at 60cm distance from thecomputer system before testing. They wereinstructed to don the 3D glasses. Then thefine depth perception test commenced. Theparticipant read the following instructions:You will see 4 circles, press the arrow keyon the keyboard that matches the circle thatlooks like it sticks out. A visual demonstrationand two practice trials were given to modelappropriate behavior.To test reliability of the digital translationof the Wirt dots, participants was re-testeda second time on the RightEye Fine DepthPerception (FDP) test. To test validity the StereoFly Test (SFT) specifically the nine StereotestCircles (SC; see Figure 1) was employed. TheRightEye Fine Depth Perception (FDP) andthe SFT test was conducted immediately afterone another. Half the group was randomlyselected to be tested on the RightEye FDPtest first and the other half on the SFT testfirst. Instructions outlined in the instructionbooklet were followed by each tester. Thisincluded holding the booklet straight beforethe participant to maintain the proper axis ofpolarization as well as providing good light, butavoiding reflections on the shiny surface. Thebooklet was held at sixteen inches, measuredby each instructor using an extended ruler.The polarized viewers (glasses) were donnedfor each test.RightEye Fine Depth Perception Test.The RightEye FDP test is similar in stimulipresentation to the Stereo Fly Test (SFT)specifically the nine Stereotest Circles (SC; seeFigure 1). The RightEye FDP test differs fromthe SC test as the 3D is computer generatedand is presented on monitor not in a physicalbook (see Figure 2).The RightEye FDP and the SC test use stimuliwhere one of the four dots are presented withcrossed binocular disparity, creating the illusionMaterials and EquipmentThe participants were seated in a stationary(non-wheeled) chair that could not be adjustedin height at a desk within a quiet, privatetesting room. The participants were asked tolook at a NVIDIA 24-inch 3D Vision monitorand Alienware gaming system that could beadjusted in height. Participants wore NVIDIA3D Vision Glasses, and a Logitech (modelY-R0017) wireless keyboard and mouse wereused. Participants heads were unconstrained.Testing ProcedureIf participants passed pre-screening require ments and all 9-points of calibration they wereVision Development & Rehabilitation37Volume 3, Issue 1 April 2017
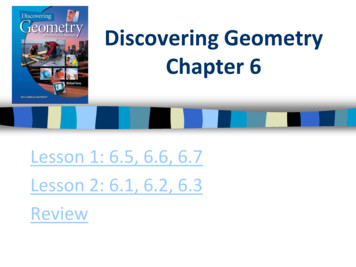
disparity to respond. If they respond correctly,then the next smaller level of disparity is shownuntil participants respond incorrectly. Oncethey respond incorrectly the testing phasebegins at that level. For example, if a personresponds correctly in the screening phaseat 800 arc seconds, the next trial shows 400seconds. If participants respond incorrectlyin the screening phase at 400 arc seconds,participants begin the testing phase at 400arc seconds. The purpose of the screeningphase is to reduce testing time by gettingthe participant in the general area of his/herindividual disparity threshold before requiringmultiple correct responses at the testing phase.Once screening is complete testing begins. Intesting, if the subject correctly responds to 3of 3 or 3 of 4 stimuli then the disparity levelgets smaller. The participant sees no morethan 4 stimuli at any one level of disparity. Ifthey get 2 incorrect responses the stimuli showa larger disparity. When the participant fails atesting level, that is, the participant gets morethan one trial wrong within a level of disparityduring the testing phase, the next stimulus isshown at the next highest disparity level, ifpassed the test ends and the score reportedis the last passed level. Output is reported inarc seconds (800-20), levels (1-10) and distanceof disparity (2.21-0.06cm).Figure 2: Sample of the RightEye FDP stimuli. One of thefour dots will appear to float when shown in 3D.that it protrudes (floats) toward the viewer.Target disparities range from 800 to 20 secondsof arc, and decrease as the test progresses.There are 10 levels of disparity in the RightEyeFDP 217 test (see Table 1).Table 1: RightEye FDP levels, arc seconds and centimeters(cm) of disparityLevel #12345678910Angle of Disparity (arc seconds)8004002001401008060504020One dot at each level is presented incrossed disparity and the location of thedisparate dot is randomly selected to reducelearning or memorization effects. Stimuli areshown for 60-seconds or less depending onwhen the user responds on the keypad. If theuser responds in 10 seconds, then the testproceeds to the next stimuli. If a participantfails to respond within 60-seconds that trial isconsidered a failure.The administration of the test is conductedin three consecutive phases, each phase hasindependent logic: phase one is practice,phase two is screening and phase three istesting. In the practice phase a total of twopractice trials are given before the screeningphase starts. Practice trails are set at 800 and400 arc seconds. During the screening phasethe participant have one attempt per level ofVision Development & RehabilitationValidity by DesignValidity by design also considered “facevalidity” or “priori validity” is concerned withwhether the test seems to measure what isbeing claimed. The RightEye FDP test hasseveral validity by design elements built intothe test. These fall into two categories: 1. teststimuli, 2. test logic and flow.Test stimuli are modeled after a standardclinical measure, the Titmus Stereo Test/Wirtcircles. This clinical test is one of the mostused tests for static stereo acuity.27 Relativedistances between dots and size of overallstimuli were mathematically calculated to berepresentative at the 60cm distance required38Volume 3, Issue 1 April 2017
for digitized testing. Color, contrast, andarc seconds (distance of disparity) were allmathematically calculated using standardconversion to a 60cm visual angle. Therefore,the RightEye FDP test stimuli were consistentwith a known, gold standard, the Titmus StereoTest/Wirt circles making the translation frombooklet to 3D screen comparable and providevalidity by design of the stimuli. Test logic andflow: after careful consideration of the TitmusStereo Test/Wirt circles test and other testlogic such as the Amblyopia Treatment Study(ATS) – HOTV Visual Acuity Test Protocol28 aswell as discussions with leaders in the field ofoptometry and ophthalmology, it was decidedthat the most effective testing protocol wouldbe the three-phase approach discussedabove (see RightEye FDP test). Specificallyconsidering accuracy of results the three-phaselogic provided the most likely consideration of:a) limited testing time to reduce the possibilityof fatigue; b) reducing the ability to guess dueto presenting only one stimuli (25% chance ofguessing correctly) at each level of disparityas is the case for the Titmus Stereo Test/Wirtcircles test; c) reducing the ability to malingerby controlling time, allowing the participantto have enough time (60-seconds) but not toomuch time to respond. The randomizationof the disparity was also added to reduce alearning or memorization effect which is morelikely in the Titmus Stereo Test/Wirt circles test.When a level is incorrectly answered in theTitmus Stereo Test/Wirt circles test the patientis asked to go back to the previous level, whichwas often answered only a few seconds earlier,and the circle of disparity has not changed.Therefore, unless the patient has a short-termmemory loss it is often easily remember as theprevious level of disparity is tested within onlya few seconds. Error handling, such as knownlocation of the participant’s eyes on the screenfurther enhances the confidence that theparticipant was not guessing because the eyescan be confirmed as “on the stimuli” targetwhen the response was made. Furthermore,Vision Development & Rehabilitationmovement of the participant, left or right, ratherthan staying still, looking directly at the stimulus,is also measured through error proofing.Should the participant move to one side or theother or move too close to the stimulus thisis recorded and will require the participant toretake the test. Furthermore, the Titmus StereoTest/Wirt circles test booklet may be tipped ormoved when held by patients during testingto gain an advantage. All such test logic andflow decisions enhance the RightEye FDP test’svalidity by design, providing further confidencein the accuracy of the results.Data AnalysisReliability was evaluated using intraclasscorrelation coefficients (ICC) between trials. Inaddition, trial-to-trial reliability was evaluatedwith Cronbach’s Alpha (CA) and the IntraclassCorrelation of Coefficients Standard Errorof Measurement for each ICC. Alpha levelwas set at p 0.05 for all statistical test. TheICC indicate the relative reliability and areinterpreted using the following criteria ICC 0.75 specifies excellent reliability and 0.40 ICC .74 represents fair to good reliability.29Convergent validity was investigated bycalculating the bivariate correlation coefficientof the Righteye FDP stereo acuity (sec arc) andSC arc seconds. Validity was also examinedusing the convergent findings within theAnalysis of Variance (ANOVA) test.To test the difference between groups(LPGA, PBP and NA), a one-way ANOVA wasused with alpha set at p .05 as the critical levelof significance. Tukey’s HSD post hoc test wasused when necessary to evaluate significanteffects. Also, when necessary, violations ofthe sphericity assumption were correctedusing Greenhouse-Geisser adjustments of thedegrees of freedom.RESULTSTable 2 shows the means and standarddevia tions of arc seconds for the three groups.CA, ICC’s, and associated SEM for trial reliability39Volume 3, Issue 1 April 2017
DiscussionThe purpose of this experiment was toexamine differences in stereo acuity using adigitized version of the Titmus Stereo Test/Wirtcircles. To provide a confidence level in theresults the Titmus Stereo Test/Wirt circles wereused as they are the most widely used andaccepted measure of static stereo acuity. As thetest was translated to a digitized version usingthe ATS-HOTV Visual Acuity Testing Protocol itwas important to test the reliability and internalconsistency of the digitized version as well asvalidity. The translation of this standardized testto the 3D digitized version (RightEye FDP test)showed strong reliability. Furthermore, internaltest consistency was examined and provided aclear indication that the test measured stereoacuity. Furthermore, validity results betweenthe Titmus Stereo Test/Wirt circles and theRightEye FDP test was high, indicating that theresults of the new digitized version can be usedand compared accurately to the Titmus StereoTest/Wirt circles results. These results indicatethat both the translation of the visual stimuli andthe testing logic (ATS-HOTV) provides similarresults to the Titmus Stereo Test/Wirt circlesand therefore subsequent analysis betweengroups can be considered with confidence.Results between groups revealed thatathletes (LPGA and PBP) were significantlybetter at static stereo acuity measured by theRightEye FDP. However, differences betweenLPGA and PBP athletes were not significant.These results are consistent with past researchby Soloman et al.9 where professional baseballathletes showed better stereo acuity thaninexperienced controls. It is also consistentwith past research that shows athletes whoplay a sport but differ significantly in skilllevel of that sport also show differences intheir stereopsis (Laby et al.,8 baseball; Coffeyet al.,10 348 golf). These results indicate thatit does not matter if the sport requires moreopen skills (baseball) or closed skills (e.g. golf).Superior stereo acuity seems to be importantfor different sports at the highest level.(Trial 1 & Trial 2) are reported (see Table 2).The CA demonstrated reliability within anacceptable level. Calculated SEMs suggest themeasures are capable of accurate assessmentof stereo acuity represented in arc seconds. AllICC were statistically significant at the p 0.05level. The test-retest reliability and internalconsistency provides a clear indication theseare in fact measuring stereo acuity.Table 2: Means followed by standard deviations ofgroups LPGA, PBP and NAArc SecondsLPGA49.42 (25.27)PBP53.35 (18.43)NA94.48 (54.84)Table 3: Cronbach’s Alpha (CA) and Intraclass CorrelationCoefficients (ICC)CAArc Seconds.625ICC.456**p .5Convergent validity via a correlationses revealed high positive significantanaly correlations between the Righteye FDPtest degree of stereo acuity and the SCtest (r .979, n 82, p .001). To providefurther evidence of validity, the ANOVA forthe SC test (F(2, 79) 6.01, p .001; ω .12) produced equivalent group differenceswith the Righteye FDP test. In addition,validity was also established by design (seeMethods section; Validity by Design). A oneway ANOVA was conducted to analyze thedifferences in stereo acuity between groups.Significant effect of stereo acuity on groupswas identified, F(2, 421) 13.822, p .001,ω .45. Tukey’s HSD tests showed thatboth LPGA golfers and PBP players scoredstatistically significantly lower (p .05) thanthe NA group. However, stereo acuity did notdiffer between the LPGA and PBP athletes.In addition, the one-way ANOVA for disparityindicated significant effect for groups, F(2,421) 10.483, p .001; 324 ω .21.Vision Development & Rehabilitation40Volume 3, Issue 1 April 2017
Results also reveal less variability in staticstereo acuity ability at the highest levels ofboth golf and baseball. In other words, not onlywere the athletes significantly better than nonathletes, but the athletes were also more like oneanother. This further supports that static stereoacuity is significantly better for elite athletesirrespective of gender as the LPGA golfers wereall female and the PBP were all male.Results of this study differ from pastresearch in soccer by Ward & Williams13 whereno differences were found between staticstereo acuity of youth elite and sub-elite soccerplayers. This may be explained through humandevelopment of stereopsis. The participantgroup in the current experiment was selectedbased on mature stereopsis and stereo acuity18and before developmental deterioration (afterage 40, Lee & Koo19). Ward and Williams14participants included a group of children nineyears and younger. Leat et al.18 state thatstereopsis does not mature in some childrenuntil nine years old and that development isnot linear in nature. Therefore, if changes indevelopment are still occurring at differentrates it could be a confounding variable thataccounted for the non-significant differencesin the results found by Ward and Williams.13It is also possible that the nonsignificantresults found by Ward and Williams13 mayoccur due to different sport demands betweensoccer, baseball, and golf. Soccer requires asignificantly larger ball than both baseball andgolf. Furthermore, the target in soccer (goalarea) is many times larger than both the hittingrange or catching range in baseball and thecup size in golf. It is therefore possible thatsoccer has “different enough” demands toboth golf and baseball that it could explainwhy nonsignificant finding were found insoccer, compared to the significant findingsfound in this study for both golf and baseballcompared to non-athletes.Limitations of this study are considered interms of broader scope. It would be incorrectto assume a child, who is still developingVision Development & Rehabilitationthis ability should be measured against afully developed person. Also, as children aredeveloping stereo acuity abilities they shouldbe measured against one another withinthose developmental levels. As developmentis not linear, that is, some children developstereo acuity faster than others, longer termpredictions about a final level of stereoacuity should be considered with great care.Furthermore, it would incorrect to predict achild’s ability at a sport based on stereo acuityas a potential predictor, before full maturityof stereo acuity is realized. Further researchat various developmental levels of stereoacuity need to be examined. Additionally,any prediction of stereo acuity for those whohave mature stereo acuity abilities should beconsidered as only one of many potentialfactors that may contribute to success in sport.Examination of dynamic stereo acuity as wellas distance stereo acuity and stereopsis wouldprovide a more complete picture of the visualabilities of these groups.CONCLUSIONSOverall conclusions show that the RightEyeFDP test is reliable, internally consistent, andvalid and can therefore be used confidently asa measure of static stereo acuity. Elite athletesin open and closed skills show significantlybetter stereo acuity than non-athletes.REFERENCES411.Wheatstone C. Contributions to the psychology ofvision – part the first. On some remarkable, and hithertounobserved phenomena of binocular vision. Phil TransRoyal Society London. 1838; 128: 371-394.2.Bishop PO. Binocular vision. In: RA Moses and WM Hart,eds. Alder’s Physiology of the Eye, Clinical Application. 8thed. St. Louis, MO: Mosby. 1987: 619-689.3.Cutting J, Vishton, PM. Perceiving layout and knowledgedistances: The integration, relative potency, and contextualuse of different information about depth. In: Epstein W,ed. Perception of Space in Motion. San Diego, CA: RogersS; 1995: 71-118.4.Mazyn LIN, Lenior M, Montagne G, Delaey C, SavelsberghGJP. Stereo vision enhances the learning of a catchingskill. Experimental Brain Research. 2007; 179: 723-726.Volume 3, Issue 1 April 2017
5.O’Connor AR, Birch EE, Anderson S, Draper H. Relationshipbetween binocular vision, visual acuity, and fine motorskills. Optometry Vision
Titmus Stereo Test/Wirt Stereo Test is the most widely used, studied and accepted method of examining stereo acuity, specifically near static stereo acuity.20 This test has been determined to be unbiased culturally with high testability for all ages.20 The test is based on horizontal retinal disparity of two images and the identification