Transcription
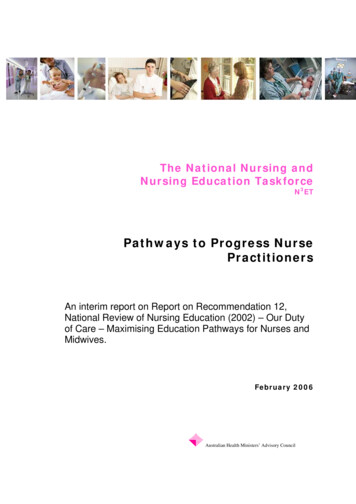
Presentation Overview:In words and a pictureThe Nursing Workforce in North Carolina:Academic Progression and New Rolesin a Transformed SystemWe will use North Carolina toframe data and informationregarding:Erin Fraher, PhD MPP, Erica Richman, PhD MSW and Katie Gaul, MA Current nursing workforceProgram on Health Workforce Research & PolicyCecil G. Sheps Center for Health Services Research, UNC‐CH “Education mobility”nurses — those whoentered workforce withADN and have gone onto BSN or higherStatewide AHEC ConferenceGreensboro, North CarolinaSeptember 11 , 2015 Future nursing workforcein a transformed systemThis work is supported in part with funding from the North Carolina AHEC Program, the Robert Wood Johnson Foundation and HRSA.Select StatsNorth Carolina, 2012North CarolinaTotal PopulationNon‐Federal PhysiciansMetropolitanNonmetropolitanRural Counties (n 54)Urban Counties (n 46)9,765,2292,208,796 (22%)7,556,433 (78%)21,7883,01518,773Per 10,000 pop22.313.624.8Primary Care Physicians7,4021,3006,102Per 10,000 pop7.65.98.1Nurse Practitioners4,2446973,547Physician Assistants4,0446713,373Dentists4,4016693,732Dental Hygienists5,4901,0304,460Registered Nurses97,22216,438 (17%)“Recommendation 4:Increase the proportion ofnurses with a baccalaureatedegree to 80 percent by 2020”80,784 (83%)Pharmacists9,8221,760Physical Therapists5,3407588,0624,582Occupational Therapists2,7733502,423Data include active, in-state health professionals licensed in North Carolina as of October 31, 2012. Physicians are non-federal,non-resident-in-training. Primary care includes family practice, general practice, internal medicine, pediatrics, and OB/GYN.At first, recommendation made us nervousSource: Institute of Medicine. Future of Nursing: Leading Change, Advancing Health. 2011Number of nurses with ADN as entry degreeand baccalaureate as highest degree hasincreased dramaticallyNumber of North Carolina Nurses Entering with ADN as EntryDegree Who Have Baccalaureate or Higher Degree, 1982‐2012Why?A 2008 Sheps Center study of Associate Degree Nursingprograms in NC showed that ADNs were more likelythan their BSN counterparts to8,0007,1027,0006,0005,0001. practice in rural/underserved areas2. practice in higher‐need settings, likehome care/ hospice and long‐term care3. Practice in higher‐need specialties, like geriatrics4,7634,000Bacc nursing3,7623,00023442,3302,000Bacc otherMasters nursingMasters 20071522012Note: Missing data ranged from 0.5% in 1982 to 11.5% in 2007Source: Fraher E, Belsky D, Carpenter J, Gaul K. A Study of Associate Degree Nursing Program Success: Evidence from the 2002 Cohort. NC Health ProfessionsData System, Cecil G. Sheps Center for Health Services Research. October 2008. CS ADN Report.pdfNote: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.1
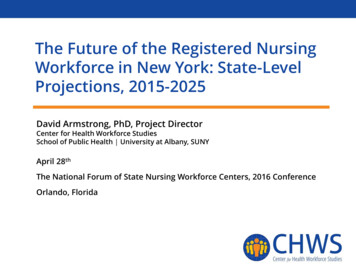
So we did another studyOur sampleOur analysis of the 2012 NC RN licensure file compares:Our research question:“Do nurses who entered the workforce withan ADN and have a baccalaureate or higherdegree in nursing behave more like ADNsor baccalaureate nurses?”N 74,763 (76.9% of total RNs)In 2012, 14,300 nurses had ADN for entry degree and baccalaureate or higher as highest degree. Our sample Includes 9,516 nurses entered with ADN and have baccalaureate or higher in nursing as highest degree—the “education mobility” nurses Exlcudes 4,784 nurses entered with ADN and have baccalaureate or higher outside nursing—the “career mobility” nursesNote: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.Mobility nurses less likely to practice in homecare/hospice and long‐term care than ADNnurses without additional educationMobility nurses less likely to practice in geriatrics thanADN nurses without additional education. Nurses withBSN at entry more likely to practice in pediatricsNorth Carolina Nursing Workforce byEmployment Setting and Degree, 2012North Carolina Nursing Workforce byPractice Area and Degree, 2012Hospital In‐Patient (n 37,577)Other (n 11,806)Hospital Out‐Patient (6,754)Rehab (n 1,142)Mental Health Facility (n 1,334)Critical/Emergency Care (n 10,105)Public Clinic/Health Dept (n 2,263)5%Home Care/Hospice (n 5,250)3%Long Term Care (n 4,093)6%4%9%Peds/Neonatal (n 5,142)BSN EntryMobility: ADN Entry and BSN as HighestADN Entry and ADN HighestSolo/Group Med Practice (n 4,691)Sch of Nursing/Medicine (n 1,463)Ob/Gyn (n 4,454)Other (n 2,932)Geriatrics (n 4,071)10%20%30%40%50%10% 6%Med‐Surgical (n 22,547)HMO/Insurance Company (n 774)0%BSN EntryMobility: ADN Entry and BSN as HighestADN Entry and ADN HighestPsych Mental Health (n 2,640)10%60%Note: Employment setting was missing for 3,420 RNs.3%0%4%5%8%10%15%20%25%30%35%Note: Specialty was missing for 3,428 RNs.Note: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.Note: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.Mobility nurses less likely to practiceas staff/general duty nursesMobility nurses 3 times more likely to practice inNC’s most distressed countiescompared to BSN entry nursesNC Nursing Workforce by Position Type and Degree, 2012NC Nursing Workforce by Economic Tier of Practice Location and Degree, 2012Other (n 6,192)5%Research (n 621)Tier 1 (Most Distress) (n 8,897)CRNA (n 1,522)15%BSN EntryMobility: ADN Entry and BSN as HighestADN Entry and ADN Highest17%Clinical Specialist (n 735)Nurse Midwife (n 167)22%Nurse Practitioner (n 3,046)26%Tier 2 (Moderate Distress) (n 19,717)Staff/General Duty (n 45,639)31%HeadNurse or Assistant (n 2,550)Instructor (n 2,550)BSN EntryMobility: ADN Entry and BSN as HighestADN Entry and ADN HighestSupervisor or Assistant (n 5,359)Consultant (n 923)73%Tier 3 (Least Distress) (n 46,149)59%52%Admin or Assistant (n 1,590)0%10%20%30%40%50%Note: Position type was missing for 3,417 RNs.Note: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, ic tier designations are from the North Carolina Department of Commerce: te: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.2
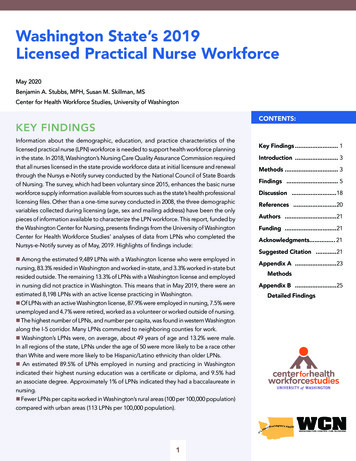
Mobility nurses twice as likely as BSN nursesto practice in rural countiesNorth Carolina Nursing Workforce by Rural/Urban Setting and Degree, 2012After seeking additional education, mobility nurses behave:More like BSN nurses in terms of specialty and setting10%Rural (n 12,974)BSN EntryMobility: ADN Entry and BSN as HighestADN Entry and ADN Highest20% Less likely to practice in home care, hospice, long‐term care and geriatricsMore like ADN nurses in terms of geographic dispersion.Compared to BSN entry nurses:24% Twice as likely to practice in rural90%Urban (n 61,789) Three times more likely to practice in NC’s Tier 1 counties80%Like neither group in terms of job title76%0%10%So do mobility nurses behave more likeADNs or baccalaureate nurses? It depends20%30%40%50%60%70%80%90%100% Less likely to be in staff/general duty positionsRural source: US Census Bureau and Office of Management and Budget, March 2013. ”Core Based Statistical Area” (CBSA) is the OMB’s collective term for Metropolitan andMicropolitan Statistical areas. Here, nonmetropolitan counties include micropolitan and counties outside of CBSAs.Note: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.Implications for education Need more rotations outside of hospital—in homehealth, long‐term care, hospice, public health and othercommunity‐based settings Continue to diffuse BSN education out to ADNs in ruraland underserved areasThe future nursing workforce:New roles in a transformedhealth system There are over 8,000 ADNs practicing in rural countieswho have not pursued additional education in nursing But it’s not just a numbers game .we need to thinkabout new roles for nursesLet 1,000 flowers bloom: ongoing experimentsin health system transformation Growing number of patientcentered medical homes,accountable care organizationsand integrated delivery systems CMS actively fundingdemonstration projects Secretary Burwell recentlyannounced 50% of Medicarepayments tied to value by 2018New models of care:key characteristicsGoal: provide patients with more comprehensive, accessible,coordinated and high quality care at lower costs Payment based on value, not volume (accountability) Emphasis on primary, preventive and “upstream” care Care is coordinated between:– medical sub‐specialties, home health agencies and nursing homes– health care system and community‐based social services (socialdeterminants of health) EHRs used to monitor patient & population health—increased useof data for risk‐stratification and hot spotting Interventions focused on both patient‐ and population‐level3
Nursing in a Transformed Health CareSystem: New Roles, New Rules“What will it take to optimizethe contributions of nurses inthese changing systems? Redesign the nursing curriculum toimpart new competencies; Retrain existing nurses to impartnew skills and knowledge; Revamp licensing examination andrequirements to reflect the newcurriculum; and Restructure the state regulatorysystem to allow flexible deploymentof the nurse workforce.”‐Quoted from Janet Weiner, MPH. Penn LDI Voices Blog. “Re: Nurses”.June 25, 2015. How do nurses fit innew models of care? PCMHs and ACOs emphasize care coordination, populationhealth management, patient education, health coaching, dataanalytics, patient engagement, quality improvement, etc. Moving more toward ambulatory settings and community care New job titles and roles emerging “Boundary Spanners” Requires application of skills in new ways anddevelopment of new skillshttp://ldi.upenn.edu/uploads/media tation: Fraher E, Spetz J, Naylor M. Nursing in a Transformed Health Care System: New Roles, New Rules.LDI/INQRI Research Brief. June 2015. http://ldi.upenn.edu/uploads/media ew and evolving role areas Population health Complex older adults andfamily caregivers Care coordination andtransitional care Use of data, evidence andother performanceimprovement skills Interprofessional collaborationSource: Fraher E, Spetz J, Naylor M. Nursing in a Transformed Health Care System: New Roles, New Rules. LDI/INQRI Research Brief. June2015.But how do we redesign structuresto support these roles?RegulationTo create a more dynamic regulatory system, we need: To develop evidence to support regulatory changes, especially fornew roles Better evaluation of pilot workforce interventions to understandif interventions improve health, lower costs and enhancesatisfaction To establish a national clearinghouse to provide up‐to‐date andreliable information about scope of practice changes in otherstates Remove regulatory barriers to let nurses utilize skills to maxbenefit of patientsSource: Dower C, Moore J, Langelier M. It is time to restructure health professions scope‐of‐practice regulations to remove barriers to care. Health Aff (Millwood).2013 Nov;32(11); Fraher E, Spetz J, Naylor M. Nursing in a Transformed Health Care System: New Roles, New Rules. LDI/INQRI Research Brief. June 2015.Sources: Bodenheimer T, Berry‐Millett R. Care management of patients with complex health care needs. Princeton, NJ: Robert Wood JohnsonFoundation; 2009.But how do we redesign structuresto support these roles?Education Must redesign education system so nurses can flexibly gainnew skills and competencies Retrain and upgrade skills of the 2.9 million nurses already inthe system – they are the ones who will transform care Training must be convenient – timing, location, &financial incentives Need to prepare faculty to teach new roles and functions Clinical rotations need to include “purposeful exposure” tohigh‐performing teams and ambulatory settingsSource: Fraher E, Spetz J, Naylor M. Nursing in a Transformed Health Care System: New Roles, New Rules. LDI/INQRI Research Brief. June 2015; Ladden et al. The Emerging PrimaryCare Workforce. Preliminary Observations from the Primary Care Team: Learning from Effective Ambulatory Practices Project”. Academic Medicine; 1013, 88(12): 1830‐1835.But how do we redesign structuresto support these roles?Policy Insurance reimbursement rulesCurrent system creates inefficiencies and hinders nurses from delivering optimal services;Shift toward value‐based care will likely support efforts to maximize nursing contributions to care Regulation of entry‐level nursing educationModify state licensure board rules governing pre‐licensure programs to ensure grads have new skills andcompetencies needed; adjust clinical training requirements to include more ambulatory experiences NCLEXCurricula designed to ensure graduates can pass NCLEX;If NCLEX changes to reflect new roles, curricula will change to keep up Federal and state funding agenciesFunding can drive innovation and encourage transformationSource: Fraher E, Spetz J, Naylor M. Nursing in a Transformed Health Care System: New Roles, New Rules. LDI/INQRI Research Brief. June2015.4
Who is going to pay for all thisretooling we need to do? Adequate and sustainable payment models to retooland redeploy the workforce are lacking Many workforce innovations are supported by one‐timefunds. If payment models don’t change rapidly enough,will these interventions be sustainable? 1,000 flowers are blooming but are adequate dollarsavailable to conduct research and evaluations necessaryto develop evidence base needed to support workforceredesign?Why the nursing workforce is criticalto health system transformation With nearly 3 million nurses in active practice, nursing isby far largest licensed health profession (about fourtimes as many nurses as physicians) Nursing care linked to quality and satisfaction measuresthat will increasingly be tied to value‐based payments Nurses provide whole‐person care across health andcommunity‐based settings Nurses are the ultimate “flexible” workforce taking onnew roles in transformed health systemContact infoErin FraherErica RichmanKatie Gaulerin fraher@unc.edu(919) 966‐5012elr@email.unc.edu(919) 966‐7737k gaul@unc.edu(919) 966‐6529Extra SlidesProgram on Health Workforce Research and Policyhttp://www.healthworkforce.unc.eduEducation Highest Degree of North CarolinaNursing Workforce: 2012Highest Degree HeldNumberPercentUnknownDiplomaAssociate DegreeBaccalaureate in NursingBaccalaureate in OtherMasters in NursingMasters in OtherDoctorate in NursingDoctorate in .0%There were 8,897 RNs missing highest degree.Note: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.Asians, African Americans, males are morelikely to have baccalaureate or higher The average age of ADN and BSN or highernurses is the same at 44 years of age. 62% of male RNs vs57% of female RNshave BSN or higher* 86% of Asian RNs and65% of African American RNshave BSN or higher***Out of 6,216 male RNs and 75,357 female RNs.**Out of 2,143 Asian RNs and 9,046 African American RNs. Race was missing for 150 RNs.Note: Data include RNs who were actively practicing in North Carolina as of October 31, 2012. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.5
Highest Degree of North CarolinaNursing Workforce: 1982‐2012Boundary spanningroles growing quicklyNorth Carolina Nursing Workforce by Highest Degree, 1982‐201250% Increasing number of staff focused on roles that shiftfocus from visit‐based to population‐based strategies47%45%40%40% Two %3%0%DiplomaAssociate1982Baccalaureate rsing2007Masters Other20120%1%DoctoratePanel ManagersHealth CoachesAssume responsibility forpatients between visits. UseEHRs and patient registries toidentify and contact patientswith unmet care needs. Oftenmedical assistants but can benurses or other staffImprove patient knowledgeabout disease or medication andpromote healthy behaviors. Maybe medical assistants, nurses,health educators, social workers,community health workers,pharmacists or other staffNote:8,897 RNs missinghighest degree data in 2012.Note: Data include RNs who were actively practicing in North Carolina as of October 31 of the respective year. Source: North Carolina Health Professions Data System, with dataderived from the NC Board of Nursing, 2012. Produced by: Program on Health Workforce Research and Policy, Cecil G. Sheps Center for Health Services Research, UNC‐CH.6
Program on Health Workforce Research & Policy Cecil G. ShepsCenter for Health Services Research, UNC‐CH Statewide AHEC Conference Greensboro, North Carolina September 11 , 2015 This work is supported in part with funding from the North Carolina AHEC Program, the Robert Wood Johnson Foundation and HRSA. Presentation Overview: