Transcription
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)Mishry et al.,LYMPHOCYTES SUBSET AND CYTOKINS ESTIMATIONON IN PATIENTS WITH SCD ATHEREDITARY BLOOD DISEASE CENTRE IN BASRAHMahaKhalaf AL-Mishry*., Nadhim K. Mahdi and Sadeq K. Ali AlSalaitDepartment of Microbiology College of Medicine, University of Basrah ,IraqABSTRACTA case-control study has been carried on patients with Sickle cell disease registered at theHereditary Blood Disease Centre (HBDC) at Basrah Maternity and Children Hospital from thefirst of December 2016 till the end of March 2017. A total of 32 patients were included, theirages ranged from 16 to 55 years. Lymphocytes subset estimation including B.lymphocytes,T.lymphocytes, T.helper, T. cytotoxic,( CD4, CD8, and their ratio) NK natural killer, by using BDAccrui C6 flow cytometry (BD, Accuri C6)Accuricytomters. This study analyzed numericalvalues of selected serum cytokines Including IL1β, IL6, IL8, IL10, IL12 and TNFby usingcytometric beds arraykit(CBA) on patients in VOC, and it compared these values with thoseobtained from the same patients in steady-state and unaffected hemoglobin AAhomozygotes who served as normal healthy controls (NHC). This study show that SCD is astate of immune deregulation in which there is chronic inflammatory state with an acuteexacerbations during crises, also ILs in addition to being important inflammatory markers,they play a key role in the immunological basis of crises,from other side IL-6 can be utilized asa predictor of crisis in patients during steady state or imminent crisis.Keywords: Lymphocytes, serum cytokines ,Sickle cell disease,Basrah Maternity and ChildrenHospital.No: of Figures: 1No: of Tables: 4No: of References:312018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)INTRODUCTIONSickle cell disease (SCD) is a genetic blooddisease which is due to the presence of polymerization and denaturation results inoxidant damage to the red blood cellmembrane, with subsequently disturbedhomeostasis which in turn, can result indehydrated dense cells and irreversiblysickled cells (Berlin and Elliot, 1991). SCD isassociated with high morbidity andmortality among sickle cell suffers indeveloping countries (Ogamidi and Onwe,2000). Red cell abnormalities lead to eitherhemolysis or vasoo-cclusion (VOC). VOCresults from interaction between red cells,leukocytesandendothelialcellinflammation, endothelial injury, leukocytesadhesion and activation of coagulationpathwayscontributetothepathophysiology of VOC crisis (Mousa etal., 2010).Pro inflammatory cytokines are believed rintegrity,andpromote both erythrocyte and leukocyteadhesion in vascular beds. Multiple studieshave demonstrated patients with SCDhave chronically elevated levels of multipleinflammatory mediators (Black et al., 2014;Salas et al., 2014).Ischemic events produced by theocclusion of both large and small bloodvessels are stressful and involve intricateinteractions between red blood cells, theendothelium, and leukocytes (Duits et al.,1998). These interactions are known to beregulated by cytokines secreted by T cellsMishry et al.,as well as by adhesion molecules, andconsequently, the immune response isimplicatedintheinitiationanddevelopment of the sickle cell crisis.Indeed, studies show that immune subsetsare operative in sickle cell disease(Herna ndez et al., 1980; Graido-Gonzalezet al., 1998; Koffiet al., 2003; Pathare et al.,2004), and the susceptibility of sickle celldisease patients in crisis to infections thatspecifically require the help of T cells to becleared CD4 T cells, subdivided based ontheir associated cytokines, play a crucialrole in inflammatory responses and theelimination of infection.(Kumar et al., 2010).This study analyzed numerical values forCD3, CD4, and CD8 T cells and levels ofselected serum cytokines in patients inVOC, and it compared these values withthose obtained from steady-state sicklecell disease patients and unaffectedhemoglobin AA homozygotes who servedas normal healthy controls (NHC). This wasdone in an effort to understand if anyimbalance in the immune response isimportant in the pathogenesis of sickle celldisease.MATERIALS & METHODSA case-control study has been carried onpatients with Sickle cell disease registeredat the Hereditary Blood Disease Centre(HBDC) at Basrah Maternity and ChildrenHospital from the first of December 2016 tillthe end of March 2017. A total of 32patients were included, their ages rangedfrom 16 to 55 years. A specially designedquestionnaire was used which includes thedate of birth, sex , Residency, details of theacute painful episode and associated2018 July Edition www.jbino.com Innovative Association
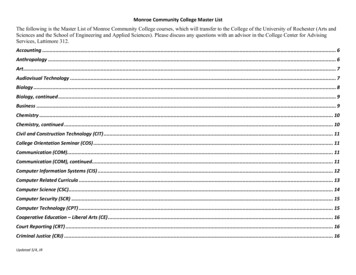
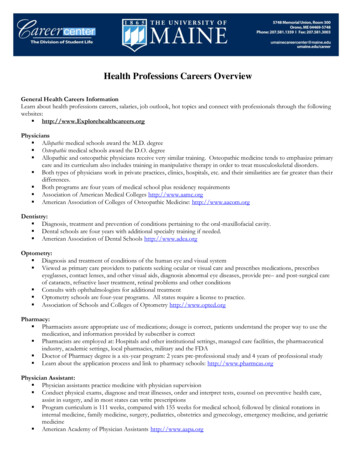
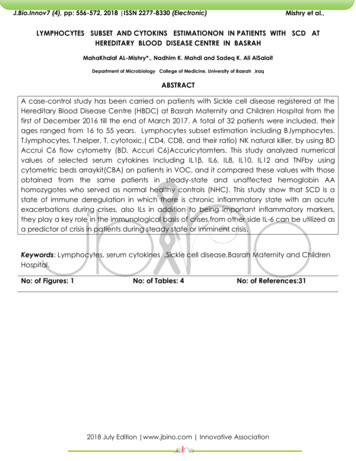
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)symptoms , site and frequency ofVasoocclutioncrisis per year, previoushistoryofstroke,Acutechestsyndrome,Hydroxy Urea intake, and historyof splenectomy, symptoms related toinfection .All patients had history ofadmission to Hereditary Blood DiseasesWard for the management of VOC, thesepatients were assessed initially (clinicallyand by selected laboratory data) duringVOC, and then during they were in steadystate (follow up).Patients recruited in study had beenevaluated for the type of SCD using HighPerformanceLiquidChromatography(HPLC), (VARIANT , β-ShortPrograms; BioRad Laboratories, Hercules, CA, USA).Thistest was also done for the control group toensure that they have normal Hb pattern.3ml of blood were withdrawn from eachpatient during painful episodes and alsoduring steady state for patients and controlgroups; the following investigations weredone for each patient with SCD and forcontrol group.Lymphocytes subset estimation includingB.lymphocytes, T.lymphocytes, T.helper, T.cytotoxic,( CD4, CD8, and their ratio) NKnatural killer, by using BD Accrui C6 flowcytometry (BD, Accuri C6, Accuricytomters,Inc. Ann Arbor 21, MI 48103, USA) and (BD,Accuri C6 software version 1.0.264.21) areused for cell acquisition and eventsanalysis. The machine is calibrated using 6peaks and 8 peaks calibration beads (BD,Accuri C6, Accuri cytometers, Inc. AnnArbor, MI48103 USA).Isotype negativeMishry et al.,control for FL1 and FL2 fluorescentdetectors (IgG1 FITC and IgG2 PErespectively, eBiosciences, Bendremedsystem GmbH, 1030 Vienna, Austria).Panelof monoclonal anti-human IgG fluorescentlabelled antibodies was used including:Flow Cytometry Reagents Anti-HumanCD3 APC 100 tests (Lot# 17-0037-42), FlowCytometry Reagents Anti-Human CD19PerCP-Cyanine5.5 100 tests (Lot# 45-019942), Flow Cytometry Reagents Anti-HumanCD4 FITC 100 tests (Lot# 11-0048-42), FlowCytometry Reagents Anti-Human CD8 PE100 tests (Lot# 12-0087-42) and FlowCytometry Reagents Anti-Human CD56(NCAM) PE 100 tests (Lot# 40 12-0567-42).All the items have been used by BD AccuriC6 flow cytometry (BD, Accuri C6,Accuricytomters, Inc. Ann Arbor 21, MI48103, USA) and (BD, Accuri C6 softwareversion 1.0.264.21) for cell acquisition andeventsanalysisaccordingtotheprocedure fixed in kits manuals, and sometime with some modifications dependingon optimal results. BD FACS Lysing Solutionsupplied fromBectonDickinsons andcompany, BD Bioscience, Ireland, REF349202).Lymphocyte gate was made on FSC/SSCscattergram as the distinct population ofevents with low FSC and SSC as shown in(Fig.1) T-helper cells was determined asCD3 /CD4 events, cytotoxic T cells asCD3 /CD8 events, B cells as CD3-, CD19 events and NK cells as CD3-/CD56 eventsas shown in (Fig.1).2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)Mishry et al.,ABCDFigure(1) Lymphocyte gate and subset determination.A- Lymphocyte subset population gate determination.B- CD4 B cell gate determination.C- CD8 B cell gate determination.D- NK cell gate ic Bead Array (CBA)byIncluding IL1β, IL6, IL8, IL10, IL12 and TNF.The BD CBA Human InflammatoryCytokines Kit can be used to quantitativelymeasure interleukin-8 (IL-8), interleukin-1β(IL-1β), interleukin-6 (IL-6), interleukin- 10 (IL-10), tumor necrosis factor (TNF), andinterleukin- 12 (IL-12) protein levels in asingle sample. The kit performance hasbeen optimized for analysis of specificproteins in tissue culture supernatants, EDTAtreated plasma, and serum samples usingone of two protocols depending on the2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)sample source. The kit provides sufficientreagents for 80 tests.Principle of CBA assays:BD CBA assays provide a method ofcapturing a soluble analyte or set ofanalytes with beads of known size andfluorescence, making it possible to detectanalytes using flow cytometry. Eachcapture bead in the kit has beenconjugated with a specific antibody.The detection reagent provided in the kitis a mixture of phycoerythrin (PE)–conjugated antibodies, which provides afluorescent signal in proportion to theamount of bound analyte. When thecapture beads and detector reagent areincubated with an unknown samplecontaining recognized analytes, sandwichcomplexes (capture bead analyte detection reagent) are formed. Thesecomplexes can be measured using flowcytometry to identify particles withfluorescence characteristics of both thebead and the detector. Six beadpopulations with distinct fluorescenceintensities have been coated with captureantibodies specific for IL-8, IL-1β, IL-6, IL-10,TNF, and IL-12 proteins. The six beadpopulations are mixed together to form thebead array that is resolved in a redchannel (FL3 or FL4) of a flow cytometer.Statistical analysisStatistical analysis was done using SPSSprogram version (18) software. Data wereexpressed by means Standard Deviation(SD).Comparisons of proportions wereperformed by cross tab using Chi-Squaretest. The Independent t- test was used forMishry et al.,quantitative comparison and between twomeans of different samples. Comparisonsbetween groups were made by using theone way analysis of variance (ANOVA)test. Correlations between variables wereevaluated by the Pearson or Spearmancoefficient. Mann-Whitney was used inorder to overcome the underlyingassumption of normality in parametric tests(the test does not assume that thedifference between 2 samples is normallydistributed). P value 0.05 was consideredas statistically significant.RESULTSThe results of the current study is an outputfrom 32 SCD patients (14 males and 18females), their ages range from 16 – 55years. Twenty two of them are SS, two aresplenoctomizedandonewithsplenomegaly. Ten of them are SF, two aresplenoctomizedandonewithsplenomegaly. The patients are recruitedduring crisis state then follow up27 of themin a steady state. There were 26 normalcontrol subjects, matched with the patientsin age and sexLymphocyte subset calculationWhole blood samples were analyzed todetermine whether there were anydifferencesamongthegroupsinLymphocyte subset (Table 1 and 2). Themean of Lymphocyte subset for threegroups are presented in Table (1).Total lymphocyte count value as shownbefore that was increased significantly incrisis and steady groups compared tocontrol the mean was (5.62 x10 9/L) ( 4.92x10 9/L) (2.62 x10 9/L) respectively ,this2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)difference is statically significant(P value 0.05).Mishry et al.,Although there was increased inCD4 T andCD8 T cellvalue in crisis and steadycompared to control group,but thisdifference is statically insignificant (P value 0.05). The CD4/CD8 ratio difference isstatically insignificant. There was little highvalue in steady than crisis but this highestinsignificant statically (P value 0.05).B cell and T cell were significantlyincreased in crisis and steady as comparedto control, B cell mean in crisis group (1.69x10 9/L) , while in steady group ( 1.19x10 9/L) and in control was (0.41 x10 9/L)with P value .006, T cell mean in crisis,steady and control was(3.41 x10 9/L),The value of NK cells was statically(3.15 x10 9/L), (1.84 x10 9/L) respectivelyinsignificant (P value 0.05).with P value 0.05Table (1) Descriptive Statistical results of Total lymphocyte count, B cell, T cell, CD4 , CD8 , NK celland CD4/CD8 ratio in all dy273.15Total852.83P value.005Total lymphocyte count.006B-lymphocytes.029T-Lymphocytes2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)Mishry et T-Lymphocytes/CD4 .056T-lymphocytes/CD8 NK cells.294.445cd4/cd82018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)Mishry et al.,Table (2) Multiple Comparisons of Statistical results of Total lymphocyte count, Bcell, T cell, CD4 , CD8 , NK cell and CD4/CD8 ratio in all groupsParameters cytesTLymphocytes/CD4 Tlymphocytes/CD8 MeanP 94.251Steady-.05981.672CrisisCrisisCrisisCrisisNK cellsCrisis2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)Steadycd4/cd8Mishry et n of Biological Markers (Specific cytokines)Serum samples were analyzed to determine whether there were anydifferences among the groups in specific cytokine (TNF, IL β, IL-6, IL8, IL10 and IL-12. Tables(3and4) .Although there was particular elevation inTNF, IL β and IL-10 values in patients groups especially in crisis ascompare to control but this difference is statically insignificant . There washighly difference of IL-6 value among groups, The total mean was (5.75pg/ml) and the mean in crisis group (12.96 pg/ml) , while in steady group (2.33 pg/ml) and in control was (1.02pg/ml) this difference is staticallysignificant(P value .003), with significant increase in crisis than othergroups.IL-8 shown significant increase in steady group ( 47.0741pg/ml) thancrisis group (22.71pg/ml) and all from control (7 ,85 pg/ml) ,this differenceis statically significant(P value .022).2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)Mishry et al.,Table (3) Descriptive Statistical results of specific cytokine (TNF, IL β, IL-6, IL8,IL-10 and IL-12) in all 47.07Total8825.76P value.255TNF.423IL-1β.003IL-6.002IL-82018 July Edition www.jbino.com Innovative AssociationControl271.04.242
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 Mishry et al.,.001IL-12The value of IL-12 was significantly high in crisis group (3.67 pg/ml) ascompare with other, in steady group ( 2.03 pg/ml) and in control was (2.03pg/ml),this difference is statically significant(P value .001).Table (4) Multiple Comparisons Statistical results of specific cytokine(TNF, IL β, IL-6, IL8, IL-10 and IL 12) ) in all groupsParametersMeanP ady2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)IL-6IL-8Mishry et 2Steady2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)DISCUSSIONIn this study absolute CD4 /CD8 T cell aresignificantly increased in crisis compare tocontrol but not to steady state patients.T-cell show significant increase in crisis andsteady compare with control group alsothere is significant increasing betweencrises and steady from side and steadywith control from other side.Also this studyshow that CD4\CD8 ratio shows increase insteady state with little difference betweencontrol and crisis but this increase didn’treach significant value. The mean NKabsolute cell count is slightly high in steadystate than in crisis and control group,however,these difference are notsignificant.The number of circulating T cells was foundto be highly variable between individualswith SCA at steady state (Koffiet al., 2003andMusaet al.,2010). However, moststudies have reported a reduction in theproportion of circulating CD4 and CD8 Tcells in SCA (Sanhadjiet al.,1988 ; Kaabaand Al-Harbi 1993 ) with normal orincreased absolute CD4 and CD8 T cellcount (Wang et al.,1988).Al-Najjar (2013)found that B lymphocytes and NK cellswere significantly increased in SCA patientswith acute VOC, And also found that thetotal T lymphocytes, CD4 T helperlymphocytes,CD8 ed in SCA patients with acute VOC,while in steady state there were allsignificantly increased.Al-Najjar (2013) found that (CD4 :CD8 )ratio showed also significant differenceMishry et al.,between steady state patients and control. Wong et al., (1995) reported that duringsickle cell crisis the (CD4 :CD8 ) ratio wasvariably affected.The cause for the observed alteration inlymphocyte phenotypes remains to beexplained. With advancing age andprogressivedeteriorationofsplenicfunction, hyposplenism has been shown tocontribute to lymphocyte abnormalities inSCA .It is possible that the observed increase inCD4 and CD8 T cells likely reflectimmune activity against recent or possiblyongoing vaso-occlusive events in SCA atrelative steady state (Sales et al., 2011;Keikhaeiet al., 2013).Little has been done to characterize T andB lymphocyte, function and contribution tochronic inflammatory diseases in SCA.Limited studies done indicate thatabnormalities in both T and B cells occur inSCA (Musaet al.,2010 and Vingertetal.,2014).In this study, we found thatcertaincytokines in sickle cell disease weresignificantly increased when comparedwith healthy subjects namely proinflammatory cytokines(TNF,IL-1b, IL-6, IL8,IL12) and anti-inflammatory cytokine(IL10) . TNF was increased in crisis groupcompared to steady state group as well asthe control group, but the difference wasnot significant ,IL-1b was increased insteady more than crisis patients , Howeverall these difference are not statisticallysignificant. IL-1β and TNF cytokines areable to promote the production and2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)release of other important mediators, suchas IL-8, a neutrophils-attractive chemokine.Together, these and other cytokines act intriggering the inflammatory cascade (Lealet al.,2013and Monaco et al.,2015 ).Lanaroet al., (2009) observed an increasein the circulating levels of TNF in SCApatients at steady state, which ischaracteristic of a pro-inflammatory state.Moreover, Pathareet al., (2004) observedanincreaseinthecirculatingconcentration of TNF during crisis events.Nnodimet al.,(2015) observed the level ofIL-1b is significantly elevated in steady stateCSD patients as compared with thecontrol.IL-6 was significantly increased in crisisgroup. In steady state it is also increasedcompared to control but the differencewas not significant. In another study thisincrement was not statically significant(Veigaet al.2013). The surprising result thatgive by (Qariet al.,2012) they observedthat IL-6 levels were significantly higherduring the steady state than during painfulcrises .Other studies showed similar finding ,Pathareetal., (2004) and Hibbertet al .,(2005) showed that serum concentration ofIL-6 was higher in SCA patients than innormal controls, and there was also asignificant increase in IL-6 levels in crisispatients when compared to steady-statepatients , as shown in this study.IL-8 in this study show significantly increasein serum level in steady group than controland even than crisis group, there issignificant difference between groups butthere is no significant difference betweencrisis and control groups, these cytokinesMishry et al.,induce increased adhesion of RBC andleukocytes to the vascular endothelium,and this adhesion can cause vasoocclusion and local hypoxia ( Pathareet al.2004). Several studies have shown thatpatients display higher levels of IL-8 duringVOC than during the stead y state(Pathareet al., 2004, Lanaroet al., 2009 andKeikhaeiet al., 2013). In contrast to thesefindings, other studies showed that thelevels of IL-8 were similar between patientsin crises and patients in steady-state(Michaels et al.,1998). IL-12 show there issignificant elevation in crisis group ascompared with other groups and nodifference in level between steady andcontrol groups.IL-12 are proinflammatorycytokines produced by macrophages anddendritic cells in response to microbialpathogens ( Hunter, 2005) .IL-12 regulatesboth innate and adaptive immunity. Thereare few reports in the literature pertainingto the role of IL-12 in SCA. Taylor et al.(1999) recommended to investigate IL-12levels in SCA patients during crises. Hassanet al. (2009) performed a similar study ofHbAS children who were infected withPlasmodiumfalciparum.Surprisingly,detectable levels of IL-12 were found inpatients with mild malaria, but not inasymptomatic individuals. This findingcould be related to the low levels of IL-10that are typically associated with thisinfection, as IL-10 is a potent inhibitor of IL12 (Hassan et al. 2009).This study demonstrated that no significantdifference in the level of IL-10 amonggroups despite of the minor elevation incrisis and steady but was not significantelevationarecent report has shown an2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)association between reduced IL-10 levelsand the frequency, type, severity, andduration of vaso-occlusive crises in childrenwith SCA. (Sarrayet al.,2015) suggesting apossible influence of IL-10 on thepathophysiologyofstroke.Musaet.al.,(2010) Observed notably low level ofIL-10 in crisis as compared with steady andcontrol. Recent work by Alsharif ( 20017)found number of, lymphocytes, CD3, CD4and CD8 count , TNF, IL-6 and IL-8, weresignificantly elevated in steady state SCApatients when compared with controlgroup, the results agree with this study.Conclusion and recommendationFrom this study we conclude that SCD is astate of immune deregulation in whichthere is chronic inflammatory state with anacute exacerbations during crises, also ILsinadditiontobeingimportantinflammatory markers, they play a key rolein the immunological basis of crises. fromother side IL-6 can be utilized as apredictor of crisis in patients during steadystate or imminent crisis.Further studyrecommend to highlight the details ofimmune deregulation and to study thepossibility of clinical utilizing IL6 and IL8 asapredictors of crisis .Also to study anypossible clinical value of the newgeneration of anti-inflammatory drugs (ILantagonists) in crisis management orprevention.ReferencesAl-Najjar, S.A. (2013). ImmunophenotypingMarkers and Cell Adhesion Molecules inSickle Cell Anaemia Patients in SaudiArabia.Ph. D. thesis, The ManchesterMishry et al.,Metropolitan University, Manchester, UnitedKingdom and King Abdulaziz University,Jeddah, Kingdom of Saudi Arabia, 174 pp.Alsharif, F.M. (2017). Immunology andSystemic Inflammation Biomarkers AmongSaudi Patients with Sickle Cell Anemia inAsymptomatic Steady State Condition.Curr. Res. Diabetes. Obes. J., 2(3): 1-4.Berlin, L. and Elliot, V. (1991).Sickle celldisease in Hematology Basic Principles andPractice.Edit by Ronald, H. Edward, J. Benz,Jr. Sanfford, J. and Shaffil, H.J.In Chen.Publishers: Churchil Livingstone, New York,Edinburgh, London, Melbourne, Tokyo.Black, L.V., Landry, R. and Templet, J.(2014).Evaluation of purified poloxamer(MST-188) in children with sickle cell diseasein crisis at OLOL Children’s Hospital,Children’s Hospital Scholarly Activity Day,Baton Rouge, Louisiana.Duits, A.J., Schnog, J.B., Lard, L.R., Saleh,A.W. and Rojer, R.A. (1998).Elevated IL-8levels during sickle cell crisis. Eur. J.Haematol., 61(5): 302-305.Graido-Gonzalez,E.,Doherty,J.C.,Bergreen, E.W., Organ, G., Telfer, M. andMcMillen, M.A. (1998).Plasma endothelin-1,cytokine, and prostaglandin E2 levels insickle cell disease and acute vasoocclusive sickle crisis.Blood, 92: 2551-2555Hassan, D.A., Marques, C., Santos-Gomes,G.M., do Rosario, V.E., Mohamed, 2009).Differentialexpression of cytokine genes among sicklecell-trait (HbAS) and normal (HbAA)childreninfectedwithPlasmodium2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)falciparum. Anna. OfandParasi, 103: 283-295.Trop.Medi.Herna ndez, P., Cruz, C., Santos, M.N. cklecellanaemia.Acta.Haematol., 63: 156-161.Hibbert, J.M., Hsu, L.L., Bhathena, S.J., Irune,I., Sarfo, B., Creary, M.S., Gee, B.E.,Mohamed,A.I.,Buchanan,I.D.,AlMahmoud, A. and Stiles, J.K. sm of children with sicklecelldisease.Experi.Biol.andMedi.(Maywood), 230: 68-74.Hunter, C.A. (2005). New IL-12-familymembers: IL-23 and IL-27, cytokines withdivergent functions. Nat. Rev. Immu, 5: 521531.Kaaba,S.A.andAl-Harbi,S.A.(1993).Reduced levels of CD2 cells and Tcell subsets in patients with sickle cellanaemia. Immunology Letters, 37: 77-81.Keikhaei, B., Mohseni, A.R., Norouzirad, R.,Alinejadi, M., Ghanbari, S., Shiravi, F. andSolgi, G. (2013).Altered levels of proinflammatory cytokines in sickle celldisease patients during vasoocclusivecrisesand the steady state condition.EuropeanCytokine Network, 24: 45-52.Koffi, K.G., Sawadogo, D., Meite, M.,Nanho, D.C., Tanoh, E.S., Altia, A.K.,Sanogo, I. and Sangare, A. (2003).Reducedlevels of T-cell subsets CD4 and CD8 inhomozygous sickle cell anaemia patientswith splenic defects.Hematol. J., 4: 363-365.Mishry et al.,Robbins ad Cotran Pathologic Basis ofDisease. 8th ed. Saunders Elsevier,Philadephia.,pp: 183-258.Lanaro,C.,Franco-Penteado,C.F.,Albuqueque, D.M., Saad, S.T., Conran, N.and Costa, F.F. (2009).Altered levels ofcytokines and inflammatory mediators inplasma and leukocytes of sickle cellanemiapatientsandeffectsofhydroxyurea therapy. J. Leukoc. Biol., 85:235-42.Leal, M.C., Casabona, J.C., Puntel, M. andPitossi, F.J. (2013). Interleukin-1β and tumornecrosis factor-α: reliable targets forprotective therapies in Parkinson's disease.Front Cell Neurosci., 7: 53-60.Michaels, L.A., Ohene-Frempog, K., Zhao,H. and Douglas, S.D. (1998). Serum levels ofsubstance P are elevated in patients withsickle cell disease and increase furtherduring vaso-occlusive crisis. Blood, 92: 31483151.Monaco, C., Nanchahal, J., Taylor, P. andFeldmann, M. (2015). Anti-TNF family: past,present and future. Int. Immunol., 27(1): 5562.Mousa, S.A., Momen, A.A., Sayegh, F.A.,Jaouni, S.A., Nasrullah, Z., Saeed, H.A.,Alabdullatif, A., Sayegh, M.A., Zahrani,H.A., Hegazi, M., Mohamadi, A.A.,Alsulaiman, A., Omer, A., Kindi, S.A.,Tarawa, A., Othman, F.A. and Qari, M.(2010). Review: management of painfulvaso-occlusive crisis of sickle-cell Anemia:consensus opinion. Clin.and Appl. Thromb.Hemost., 16(4): 365-376.Kumar, V., Abbas, A.K. and Fausto, N.(2010).Diseases of the immune system. In:2018 July Edition www.jbino.com Innovative Association
J.Bio.Innov7 (4), pp: 556-572, 2018 ISSN 2277-8330 (Electronic)Nnodim J. K., Meludu S., C., Dioka, C.E.,Martin I., Ukaibe N., and Ihim A (2015).Cytokine Expression in Homozygous SickleCell Anaemia. J. Krish. Insti.ofMedi. Sci.Univ., 4(1): 34-37.Ogamdi, S.O. and Onwe, F. (2000).A pilotstudy comparing the level of sickle cellknowledge in a University in SoutheasternTexas and a University in Enugu State,Nigeria,WestAfrica.Ethn-Dis.SpringSummer, 10: 232-236.Pathare, A., Al-Kindi, S., Alnaqdy, A., Daar,S., Knox-Macauly, H. and Dennison, D.(2004).Cytokine profile of sickle cell diseasein Oman.Am. J. Hematol., 77: 323-328Qari, M.H., Dier, U. and Mousa, S.A.(2012).Biomarkers of inflammation, growthfactor, and coagulation activation inpatients with sickle cell disease.Clin.andAppl. Thromb. Hemost., 18: 195-200.Salas, J., Deyo, J. and Black, L.V.(2014).Clinical Mimics of Lymphoma.Children’s Hospital Scholarly Activity Day,Baton Rouge, Louisiana.Sales, M.C., de Queiroz, E.O. and Paiva ,A.A. (2011). Association between anaemiaand subclinicalinfection in children inParaiba State, Brazil.RevistaBrasileira deHematologiaeHemoterapia, 33: 96-99.Sanhadji, K., Chout, R., Gessain, A., Sasco,A.J., Yoyo, M., Mezard, F., G. and Touraine,J.L. (19
natural killer, by using BD Accrui C6 flow cytometry (BD, Accuri C6, Accuricytomters, Inc. Ann Arbor 21, MI 48103, USA) and (BD, Accuri C6 software version 1.264.21) are . channel (FL3 or FL4) of a flow cytometer. Statistical analysis Statistical analysis was done using SPSS program version (18) software. Data were expressed by means .