Transcription
District of Columbia Department of HealthFive-Year Maternal and ChildHealth Needs Assessment Summary2021-2025September 2020DC Health Community Health Administration
AcknowledgementsGovernment of the District of ColumbiaMuriel Bowser, MayorOffice of the DirectorLaQuandra S. Nesbitt, MD, MPH, DirectorCommunity Health AdministrationAnjali Talwalkar, MD, MPH, Senior Deputy DirectorAnkoor Shah, MD, MBA, MPH, Deputy Director for Policy and ProgramsPrepared by:Jasmine Bihm, DrPH, MPH, Program Manager for Title V Maternal andChild Health Services Block GrantContributing Members:Nadia Khan, Public Health AnalystMoriam Animashaun, Data AnalystMarcella Hernandez Wild, Data Analyst
IntroductionAs part of the federal Title V Maternal and Child Health Services Block Grant Program, statesare legislatively required to report on the MCH populations by conducting a comprehensive andstatewide Five-Year Needs Assessment and presenting findings through a Needs AssessmentSummary.Five-Year Needs Assessment ProcessFrom February 2019 to March 2020, the DC Health Title V team utilized quantitative andqualitative methods to gather information to assess strengths and needs of the MCH populationof the District of Columbia in each of the five population health domains - women, infants,children and youth, including children with special health care needs, and adolescents. Theteam engaged the MCH Advisory Council at the beginning to serve as an advisory board andprovide input on unmet needs and positive factors affecting the district’s MCH populations. Theteam conducted a literature review of existing, recently published health reports, an analysis ofhealth outcome data provided by the Center for Policy, Planning and Evaluation (CPPE) at DCHealth, and nationally available datasets. In keeping with needs assessment best practices fromother states, we conducted a community Discovery Survey for input on important MCH topicsfrom a public perspective. The team conducted key informant interviews with stakeholders whoserve as experts in the administration, delivery of services and care for MCH populations, aswell as a focus group with the Youth Advisory Council. In addition, we incorporated focus groupand listening session data gathered as part of the District of Columbia’s Office of the StateSuperintendent (OSSE)’s Preschool Development Grant: Birth to Five Needs Assessment.MethodologyThe methods used for gathering data included a literature review, the administration ofelectronic surveys (English & Spanish) to the MCH Advisory Council and the District community,key informant interviews, family listening sessions and focus groups. The Community HealthAdministration vetted questions for surveys, interviews and focus groups prior to distribution.The Title V team held discussions with department of health staff from other states andreviewed needs assessment best practices. Best efforts were made to use the most recent dataavailable for reporting on health indicators. A list of topics was compiled from a review of thedata collected. Topics were then prioritized based on frequency of mention and ranking by TitleV staff and senior leadership. The final list of topics was selected based on needs assessmentfindings and agency funding priorities.MCH Population Health StatusKey findings of the needs assessment suggest the following priority areas: well-woman visits,breastfeeding, reducing perinatal disparities, mental health including grief and trauma-informedcare, implicit bias/discrimination, positive youth development, early childhood developmentalscreening, medical home identification/place-based care, and community safety including safeand affordable housing. The findings point to persistent health disparities by race/ethnicity andimmigrant, and socio-economic status. In addition, they emphasize the need to address socialdeterminants of health such as housing, education, violence and discrimination/implicit bias asthese were among the top factors community members identified as the biggest unmet needs ofDistrict women, children and families, as well as things needed to live their fullest lives. Factors1
identified through the Discovery Survey as positively influencing families to thrive within theDistrict community were community support activities, access to public spaces, a safeenvironment, food access, social support, community-based services, public transportation andquality education. The full report on the District of Columbia’s MCH Needs Assessmentdescribes the findings, strengths and needs of each population domain and will be shared onthe DC Health website, Title V page: https://dchealth.dc.gov/page/title-v.The Covid-19 Pandemic and Impact on the District of Columbia MCH PopulationThe 5-year Needs Assessment presents data collected before the start of the COVID-19pandemic. District residents and families, like many across the nation have been impacted bythis public health emergency. The District of Columbia Mayor implemented an early and swiftresponse to Covid-19 with an executive order issued on February 28th directing District agenciesto prepare for potential impacts of the Coronavirus. This included directing the Department ofHealth and Department of Homeland Security and Emergency Management to coordinate theDistrict’s response, and the activation of the Emergency Operations Center on March 2nd. DCDepartment of Health confirmed the District’s first coronavirus case on March 7th and the Mayordeclared a public health emergency on March 11th which initiated a series of city-wide publichealth safety measures over the next few days to help prevent spread of the virus includinglimiting mass gatherings to 250 or less on March 13th, shifting Spring Break for DCPS studentsto March 16th (and ultimately suspending in-person learning for the rest of the school year),shifting District Government operations to an agency-specific telework schedule as of March16th, and prohibiting mass gathering of 50 or more on the same day. On March 24th, the Mayorannounced the closure of non-essential businesses and prohibition of gatherings of 10 or morethrough April 24th, however this was ultimately extended through late June. Guidance on maskwearing and social distancing was also issued early on in the pandemic in April, when the publichealth emergency was extended. Free Covid-19 testing sites for residents experiencingsymptoms were set up across the District. The Mayor established a Contact Trace Force to hirehundreds of additional tracers at DC Health on April 23rd. DC Department of Health, in its role asone of the primary public health responders, has developed and continued to implement timelyguidance and provide resources to help mitigate the Covid-19 crisis.As of early September 2020, the District had approximately 14,362 known cases ofCoronavirus, a test positivity rate of 2.8%, and 611 lives lost. Approximately 51% of cases areamong Black/African Americans and 22% among Whites with 19-30 and 31-40 as the agegroups with the greatest percent of cases (22 and 20%, respectively). While the incidence ofany new cases or deaths are undesirable outcomes, the District’s rates of Covid-19 have beenrelatively stable as compared to other states. Much of this stability can be attributed to thedecisive safety measures described above. Nevertheless, the Covid-19 pandemic is still presentin District residents’ lives, as the jurisdiction is presently in Phase 2 of re-opening, and thusschools, many businesses, etc. have not yet returned to full, pre-pandemic operational status.The pandemic has paralleled and exacerbated existing socio-economic disparities. Thepreliminary rate of unemployment for May 2020 was 9% (triple the 3% rate of May 2019). Lackof, or reduction in employment can have domino effects on health outcomes. Connected tofinancial stability, food insecurity is relevant to all MCH populations. On average, over 20162018, D.C. had a 10.6% prevalence of household food insecurity, this represents a 1.8%decrease from the 2006-2008 rate of 12.4%. Despite this improvement, approximately 11% ofareas in the District are food deserts, with more than three-quarters located in Ward 7 and Ward8, areas with the lowest median incomes and highest needs. To help combat these issue duringthe pandemic, WIC has been deemed an essential service and grocery distribution sites havebeen set up in high-need areas, among other efforts to help vulnerable during the pandemic.2
Several of the already pressing needs identified by the 5-year MCH Needs Assessment havethe potential to be greatly exacerbated. In terms of women’s health, between 2009 and 2016,the percent of infants born to mothers receiving prenatal care beginning in the first trimesterdecreased from 74.7% to 65.7%. Neighborhoods across Wards 7 and 8 experience lower ratesof first trimester prenatal care initiation, ranging from 44.16% to 64.19%. Violence againstwomen was echoed in key informant interviews as an important issue for Districtresidents. Unfortunately, with Covid-19 and stay-at-home orders to help mitigate virus risk, thereis also an unintended higher risk of interpersonal and domestic violence. An FQHC and Title Vgrantee, La Clínica del Pueblo, which serves a predominantly immigrant, low-incomepopulation, has continued working with the DC Coalition Against Domestic Violence (DCADV)on the planning activities associated with staff training on gender-based violenceprevention. La Clínica’s Gender and Health team is revising and updating the DCADV content torespond to the challenges that gender-based violence victims are facing as a directconsequence of the COVID-19 pandemic context.As far as perinatal health is concerned, breastfeeding efforts including lactation on-siteassessments at Howard University Hospital had to be cancelled or rescheduled. BecauseChildren’s National Medical Center (CNMC) reduced their in-person pediatric visits, there hasbeen a decrease in breastfeeding consults. Efforts to maintain consultations are ongoingthrough telephonic consultation. La Clinica del Pueblo has been under a modified operatingstatus since March 16th. Under this status, well-women, well-child, prenatal and maternal carevisits are ongoing either via telehealth or through a limited number of on-site visits. These MCHvisits, in addition to immunization and family planning services continue to be prioritized at theclinic, with the focus for well-child visits on infant care, due to existing perinatal health disparitiesamong this population.In reference to children and children with special health care needs, the immunization coverageaverage rate for MMR, Varicella, and DTaP was around 86% as of Fall 2019 – these rates havedecreased as health and medical facilities have modified operations, and families navigatepriorities during the pandemic. In June, DC Health identified about a 70% decrease in vaccineadministrations from March through May 2020. This is similar to trends identified in Marylandand nationwide per the CDC. This decline in number of vaccines administered over the courseof those three months has resulted in a 3-4% decrease in total immunization coverage amongschool children. DC Health took the following immediate actions to increase childhoodimmunization access and coverage including: a public messaging campaign to highlight theimportance of childhood vaccinations and overall preventative care; public messaging campaignto reinforce that it is safe to see your doctor or visit a hospital; coordinating and strategizing withpediatric health centers across the District to improve access to care via opening weekend,evening, and walk-in hours, mailing out over 25,000 letters to families notifying them of whichvaccines are overdue and points of access, and more. In July, the District saw a four-foldincrease in vaccine ordering when compared to April (11,690 doses ordered in July compared to2,807 in April). Vaccine ordering is an early indicator that typically corresponds to an increase inoverall vaccine coverage later. Although the vaccine administrations are still overall lower whencompared to 2018 and 2019, DC Health is encouraged the District is moving in the rightdirection and will continue efforts to increase these rates.The initial closure of schools had a major impact on the work of Title V MCH grantees asseveral operate in conjunction with the School Based Health Centers (SBHC). The AmericanAcademy of Pediatrics (AAP) recommends limiting the amount of time that babies and toddlersspend in front of a screen which was impractical for some families to do even pre-pandemic.3
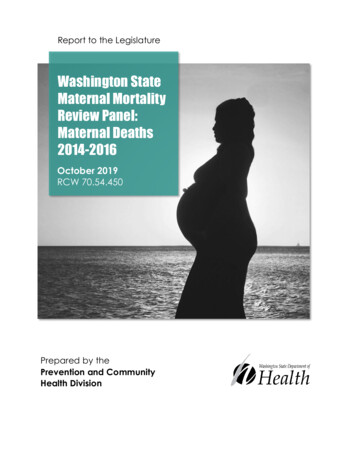
Keeping babies and toddlers away from TVs, tablets, computers, smartphones, andgaming systems is particularly impractical now during the pandemic, when many families havebeen required to engage in virtual learning, or need tools to help keep children occupied whileparents engage is work duties. As an example, the school year has started, but will be executedthrough virtual learning at least through November. Parent Navigators who assist other parentsof children with special health care needs have struggled to take care of their own children whilestill providing care for those most vulnerable. Thus, in accordance with hospital guidance,navigators of the CNMC Parent Navigator program were allowed to telework.Adolescent health issues are also impacted. Adolescent mental health and mental disorderswere among the health indicators that got worse over the last few years. The provision of theWendt Center’s Resilient Scholar program, group and individual trauma-informed therapysessions were drastically altered – either delayed or moved to telephone or online platforms,which presented with its own challenges for families with limited internet, electronic resources orthose experiencing trauma related to family dynamic issues who were now required to stay athome. Efforts to pilot test projects focused on health care transition within several SBHC’s werehalted.As described previously, DC Health, other local government agencies and community-basedorganizations have all had to modify operations to adapt to a “new normal” to continue to serveDistrict residents, in particular those most vulnerable. As the Covid-19 pandemic continues, DCDepartment of Health will remain at the forefront of helping to stem the health impact of thiscrisis. Title V funds and programming remain vital to keeping mothers, children, including, and inparticular, those with special health care needs, adolescents and families, safe and healthy.Women’s/Maternal HealthFigure 1. Women with Incomes below the Federal Poverty LineWomen comprise the majority of the of the District’spopulation (52.4%) with more than a quarter ofreproductive age (15 – 44 years of age). By race, 47%of women in the District are African American, 40%are White and 11% are Hispanic. Heart disease andcancer are the two leading causes of death amongwomen (and men) accounting for half of deaths in theDistrict in the last five years. Although insurance rates(96.7%) for the maternal health population exceed thenational average (92.1%), disparities in health fordifferent age and racial/ethnic groups continue to exist.According to Figure 1, nearly 20% of women living inthe District had incomes below the federal povertylevel in 2016, with the highest concentration living inneighborhoods in Wards 7 (Twining, Stadium Armory)and Ward 8 (Douglass and St. Elizabeth’s), followed by some neighborhoods in Wards 2, 5, andWard 6. The District’s priorities for Women’s/Maternal Health include: well-woman visits,prenatal care, mental health, safe and affordable housing, implicit bias/discrimination.Access & Quality of HealthcareThe District is home to seven hospitals and hospital systems, of which five are birthing facilities.Providence Hospital, in Ward 5, closed as part of a revised strategic plan and United MedicalCenter (Ward 8) permanently closed the labor and delivery unit after temporary closure by the4
Department of Health due to quality of care concerns. Hospitals, are concentrated in theNorthwest and Northeast quadrants of the District, thus particularly those who live in the eastend of the city, and are predominantly Black and low-income have difficulty accessing birthingservices.Maternal MortalityFrom 2005-2014 there was an average of 39 deaths among women per 100,000 live births fromcauses related to pregnancies - one of the highest rates in the U.S. This is more than twice thenational average of 17, and far higher than non-Hispanic white mothers at 13 deaths per100,000. Differences also exist between racial and ethnic groups and coverage type. Only 36%of women in the District on Medicaid and CHIP received at least 81% of the expected number ofprenatal visits and only 49% had a postpartum care visit between 21 and 56 days after givingbirth. The District of Columbia Maternal Mortality Review Committee, established in 2019, isworking towards collecting data to identify key causes of maternal mortality in the District.Testimony by the District’s chief medical examiner at a December 2018 hearing revealed that75% of the maternal deaths recorded in DC between 2014 and 2016 were black women. Equityissues are present alongside high infant mortality creating what some perceive as a maternalcare crisis in DC.Well-Woman Visits and Preventive Care UtilizationIn 2018, the Behavioral Risk Factor Surveillance System (BRFSS) reported that 82.4% ofwomen in the District had a routine check-up by a doctor within the past year. Nevertheless,there continues to be a disparity in preventive care use by income levels. Those with a lowerincome (64%) are less likely to visit the doctor regularly than those with middle income (74%) orhigh income (89%).Prenatal CareAlthough District women are engaging in some preventive care services, rates of womenaccessing prenatal care are significantly lower. Between 2009 and 2016, the percent of womenwho initiated prenatal care in the third trimester or had no entry to prenatal care increased from5.8% to 6.3%. Women in neighborhoods across Wards 7 and 8 have lower rates of firsttrimester prenatal care initiation, ranging from 44.16% to 64.19%. Approximately 2.39% ofwomen in the District who had a live birth did not receive any prenatal care. The percentage ofwomen who did not receive prenatal care was higher in most Ward 7 and 8 neighborhoods(2.54% to 9.52%). Mothers who did not initiate prenatal care were more likely to have apregnancy that resulted in a preterm birth (26.9%) as compared to those who initiatedpregnancy during their first trimester (10.2%). Characteristics such as previous preterm birth,smoking prior to pregnancy, mother being overweight or obese, history of diabetes, history ofhypertension have all been associated with a higher risk of preterm birth and aredisproportionately experienced by non-Hispanic black mothers. Several key informants alsohighlighted late entry to prenatal care as a contributing factor toward maternal and infant healthdisparities.Maternal Mental HealthThe mental health of women emerged as an important finding as women often prioritize theneeds of their family before their own. According to 2018 BRFSS data, 13% of women in theDistrict reported experiencing 14 days or more of their mental health not being good comparedto 12.1% of men.5
Programmatic/District Strengths Targeted Messaging to Improve Health Literacy: DC Health hasembarked on a health literacy “Well Women” campaign (part of DCits overarching Perinatal Health Initiative) to bolster awareness ofthe importance of routine well care. Improved Data: DC Health has prioritized gathering additionaldata to better understand barriers for reproductive age women,particularly among women not traditionally engaged in care,including a Title V supported literature review as part of a study on understanding the effectsof racism on maternal health outcomes. Title V provides financial support to enhance DCPRAMS, leveraging findings to develop programming. Integration of Population Health and Social Determinants of Health (SDOH) tools andGender-based Violence Support: Title V funds have supported La Clinica del Pueblo whoserves primarily immigrant and low-income Latinas, in integrating population health andSDOH tools into their electronic medical records systems. The program also expanded itsapproach to gender-based violence by including strategies that engage men and boys asallies, and address harmful social norms.Needs and Areas of Opportunity for New Activities Mental Health Services: In order to ensure women in the District have an equitableopportunity to access mental health resources, DC Health must be mindful of fundingservices that diversify the workforce as well as placement of services. Address Barriers to Prenatal Care, Especially for Mothers on Medicaid: As DC Healthconsiders the definition of a “well woman,” it will be important to continue to considerprograms that offer opportunities for healthy eating, living and early access to prenatal care. Promoting Safe and Fair Public Spaces: Generational stress, racial discrimination, andother forms of discrimination were identified as impacting women in the District. Black andHispanic/Latinx District residents are more likely to interact with police officers, making themfeel unwelcomed in public spaces. Expanding Access to Healthcare: Healthcare systems data and key informant interviewsemphasized issues women face associated with the closure of hospitals in the District,limiting patient choices for care and increasing travel distance to the nearest hospital. Improving Postpartum Care: Strengthening linkages to care through existing programs(Healthy Start; DC Maternal, Infant, and Early Childhood Home Visiting (MIECHV); SchoolBased Health Centers) will allow women to receive timely services during the postpartumperiod. Diversifying the Workforce/Mitigating Differences in Healthcare Delivery: Several keyinformants stated that diversifying the workforce and providing implicit bias trainings willallow healthcare agencies and clinics to provide culturally and linguistically appropriate careand mitigate differences in healthcare delivery based on race/ethnicity, sex, gender,nationality, etc.Infant/Perinatal HealthInfant health indicators often serve as a gauge for the overall health of a community. In theprevious five years the District of Columbia has prioritized reducing infant mortality andimproving other perinatal outcomes, such as pre-term births, low and very low birth weight birthsand early maternal entry to prenatal care. In 2018, DC Health published a comprehensive reporton Perinatal Health and Infant Mortality. Key findings regarding demographics of Districtmothers include that from 2010-2012 to 2013-2016, DC experienced an increase in births to6
non-Hispanic white women, women with more than a high school education, women aged 30-39years, and women who are married. In addition, births to mothers aged less than 20 yearscontinued to decline as compared to 2010-2012. Births to mothers aged 15-19 years decreasedsignificantly by 50% from 2006-2016. The District’s priorities for Infant/Perinatal Healthinclude: reducing perinatal disparities including infant mortality, preterm birth, low birthweight, and breastfeeding.Infant MortalityInfant mortality rates (IMR) in the District have been on a downward trend from 2007 through2016 from 13.1 infant deaths per 1,000 live births and 7.1 per 1,000 live births, respectively.This rate is still higher than the Healthy People 2020 target rate of 6.0 per 1,000 livebirths. Although the overall IMR declined by 45.8%, significant disparities between racial andethnic groups persist with the rate for African American mothers three times higher than forWhites.Health Characteristics of Women Prior to PregnancyHealth characteristics of women who had live births during 2015 – 2016 demonstrate starkdifferences when stratified by race/ethnicity. Non-Hispanic Black women had higher proportionsof experiencing a previous preterm birth (4.92%), smoked prior to pregnancy (7.05%), beingoverweight or obese (55.44%), had diabetes prior to becoming pregnant (1.26%), and hadhypertension prior to becoming pregnant (3.52%) than their White counterparts (1.04%, 0.94%,21.31%, 0.25%, and 1.12%, respectively). Similarly, Hispanic women had a higher proportion ofexperiencing a preterm birth prior to the current pregnancy (2.55%), were overweight or obese(46.48%), had diabetes prior to their current pregnancy (1.42%) compared to their Whitecounterparts.Health Characteristics of Women during PregnancyWomen’s health experiences during pregnancy also differ significantly. For example, nonHispanic White women initiated prenatal care during their first trimester at a higher rate (86%),with Hispanic women falling second (64%) and non-Hispanic Black women experiencing thelowest rate (52%). Non-Hispanic Black women also experienced higher percentages of havingsmoked during their pregnancy (4.6%) compared to Hispanic (0.56%) and non-Hispanic Whitewomen (0.43%).Birth Outcomes: Preterm Births (PB) and Low Birth WeightPremature births (births to infants less than 37 weeks old) can lead to significant morbidity andmortality. The total number of PB suggested little change from 2011 at 11.0% to 10.6% in 2017.During 2015 – 2016, the number of women who experienced a preterm live birth and haddiabetes prior to becoming pregnant was about 2.6 times higher than women who did not havediabetes prior to pregnancy. The proportion who experienced a preterm live birth and wereeither overweight or obese was 33% higher than women who were normal or underweight. Theproportion of PB for non-Hispanic Black women was significantly higher (12.8%) compared tonon-Hispanic White women (7.77%). This rate exceeds the 6.5% target for 2020. In 2018,6.71% of births were between 34-37 weeks of gestation in the District. The PB rates were higherin neighborhoods located in Wards 5, 7, and 8. Most neighborhoods in Wards 4, 6, 7, and all ofWard 8 had a higher percentage of women who delivered between 34-37 weeks compared tothe District average. According to 2015-2016 birth data, 74% of low birth weight babies werefrom Ward 5, 7, and 8.7
BreastfeedingThe 2020 Breastfeeding Report Card states that 88.0% of infants in the District of Columbiahave ever breastfed, this is almost 4% higher than the national rate. Breastfeeding generallydecreases as the age of the infant increases, with rates in the District at 64.7% by 6 months and39.3% by 12 months. The latest rates demonstrate an increase over the last few years with therate at 82.8% for ever breastfeeding, 57.4% and 33.1% for 6 and12 months, respectively,according to the 2016 Report Card. While the overall ever breastfed rate is high, breastfeedinginitiation rates can vary widely by race and socio-economic status – the DC WIC breastfeedinginitiation rate in 2018 was 62% (up 5% from 2017, largely due to peer counselors and 24/7access to an IBCLC from Pacify), but can be as low as 30.9% at DC WIC clinics inpredominantly African American areas of the city.Culturally & Linguistically-appropriate Breastfeeding Support and Education: Several keyinformants highlighted that women first turn to their family and friends and then their medicalprovider, if applicable, for breastfeeding support. One informant stated that women of colortypically get their breastfeeding advice from women who have children and are from theirimmediate family, and another stated that women typically ask their mothers or grandmothersfor guidance, but the physician is usually last. Because of this, it is possible that women may ormay not always be delivered the proper breastfeeding education that fully supports a woman’sdecision to breastfeed.Programmatic/ District Strengths Strong Community-Based Breastfeeding Support: Title V funds the DC BreastfeedingCoalition (DCBFC), to provide maternity facilities with financial support and technicalassistance to achieve and maintain Baby-Friendly designation, provide LactationCertification Preparatory Programs with a focus on historically underserved populations,breastfeeding peer educators, linkages and referrals to WIC for prenatal and postpartumwomen. Also, the District established a Lactation Commission. Safe Sleep Program (SSP): Title V supports the Safe Sleep Program that aims to reducethe risk of SIDS/Sudden Unexpected Infant Death through empowering parents. Comprehensive Perinatal System: DC Health has developed a comprehensive approachthat encompasses seven priorities that collectively work to improve perinatal outcomes. TitleV supports staff that oversee many of DC Health’s federally funded maternal and childhealth programs, including Healthy Start, the Maternal, Infant and Early Childhood HomeVisiting (MIECHV) Program and the Supplemental Nutrition for Women, Infants and Children(WIC) Program. Targeted Messaging to Improve Health Literacy: DC Health’s Perinatal Health Initiativeincludes campaigns and messaging to address perinatal health disparities and improvematernal and child health in the District.Needs and Areas of Opportunity for New Activities Pregnancy Risk Assessment Monitoring System (PRAMS): The District’s PRAMScollects state-specific, population-based information from women to assess theirexperiences and attitudes before, during, and after pregnancy. DC Health plans to includequestions that will provide additional insight on women’s postpartum care and postpartumdepression.8
Immunizations: Efforts will focus on the enhancement of data collection, tracking, sharingof data from hospitals, and partner organizations complying with immunization requirementsand case management.Strengthen Data Systems, Newborn Hearing and Metabolic Screenings: DC Health’sUniversal Newborn Hearing Screening Program and the Newborn Metabolic ScreeningProgram are both supported by Title V. Although newborn screenings hav
visits are ongoing either via telehealth or through a limited number of on-site visits. These MCH visits, in addition to immunization and family planning services continue to be prioritized at the clinic, with the focus for well-child visits on infant care, due to existing perinatal health disparities among this population.