Transcription
COLLABORATIVE QUALITY IMPROVEMENT OFMATERNAL, NEWBORN, AND CHILD HEALTHSERVICES IN TAJIKISTANSalwa Bitar, Faridun Khudonazarov, Roman Yorick, IntraHealth InternationalGulnora Razykova, Tahmina Jaborova, Halima Boboeva, Surayo Pulatova, Abt AssociatesJuly 2020
BackgroundThe Feed the Future Tajikistan Health and NutritionActivity (THNA) is a five-year (2015-2020) project fundedby USAID and led by IntraHealth International. Withpartner Abt Associates, IntraHealth is working with theMinistry of Health and Social Protection of the Populationto improve the health and nutrition of women andchildren living in 12 of 24 districts of the Khatlon region.Facing many social and economic challenges at the timeof the break-up of the Soviet Union, Tajikistan additionallysuffered as a result of the 1992-1997 civil war that tookplace mainly in Khatlon. The conflict damaged health careinfrastructure and services, with more than 60 primaryand secondary care health facilities destroyed. It alsoresulted in “brain drain,” as over 260,000 people, includingmedical professionals, left the country.2. Increase availability and consumption of diversenutrient-rich foods throughout the year3. Drive behavior change related to MNCH, water,sanitation, and hygiene (WASH), and nutrition forchildren and women4. Conduct advocacy to support and institutionalizethese interventions.This technical brief covers clinical QI interventions inhospitals and PHCs while a second technical briefdocuments community-based approaches. The majorclinical focus areas for QI include ANC, emergencyobstetric and newborn care (EmONC), effective perinatalcare (EPC), integrated management of childhood illness(IMCI), anemia, and nutrition.Figure 1. Health care facilities in the 12 Feed theFuture districtsThe Ministry of Health and Social Protection of thePopulation is committed to improving the quality ofmaternal, newborn, and child health (MNCH) andnutrition services in hospitals and primary health centers(PHCs), as well as in communities. A government call toaction to eliminate maternal deaths resulted in majorreductions in the maternal mortality rate, from 68/100,000live births in 2000 to 32/100,000 in 2015.To continue thisprogress, multiple quality improvement (QI) initiatives arebeing considered and introduced. However, despite highemphasis on QI at the central level, the ministry’s capacityto roll it out to facilities remains limited and donordependent, and health indicators are poor, especially inrural areas such as Khatlon.In the 12 districts where THNA works, the 2017Demographic and Health Survey showed only 44% ofpregnant women had made four antenatal care(ANC) visits and, while facility delivery was high at 90%,postpartum care was almost nonexistent. Infant deathand under-5 mortality rates remained high (33 and 40 per1,000 live births, respectively), along with the prevalenceof anemia, malnutrition, and child illnesses such asdiarrhea and acute respiratory infections. These problemsare compounded by a high fertility rate (4.1) and lowcontraceptive prevalence (21%).ApproachesTo address these challenges, THNA implements fourintegrated, cross-sectoral approaches:1. Improve quality, accessibility, and utilization of MNCHservices at the community, PHC and hospital levelsClinical-level ActivitiesTHNA and the ministry are implementing a collaborativeimprovement approach to strengthen the quality of thetargeted clinical services at 12 hospitals and 12 PHCsserving the Feed the Future districts, using World HealthOrganization (WHO) scorecards for EPC and IMCI asquantitative measures for QI. The scorecards are toolsto conduct rapid health facility assessments for quality ofcare, in which each item is evaluated through informationgathered by different sources to reach an overall score.
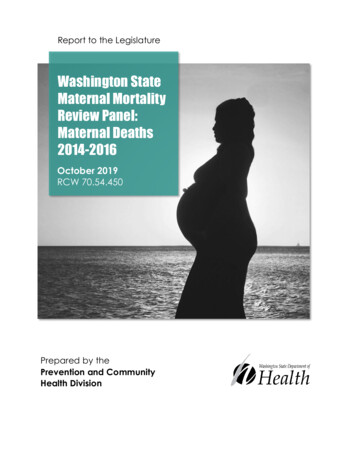
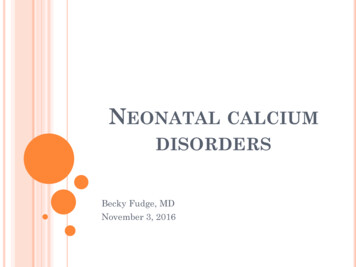
Essential features of THNA QI collaborative Shared objectives and clinical standardsQualified, functional QI teamsShared monitoring system using WHO scorecardsTraining and coaching supportLearning sessions and site visits to share experiences,innovative ideas, and solutionsSample QI team members Facility head (honorary team lead)Responsible person for QI (collaborative improvementteam lead)Responsible person for infection control and clinicalsafetyResponsible person for continuing educationResponsible person for internal protocolsQI collaborative: Originally developed by the Institutefor Healthcare Improvement and further adapted byUniversity Research Co., collaborative improvement isa structured QI approach that organizes health facilitiesto work together for 18 to 24 months to achievesignificant gains in specific areas of care. The intentionis to accelerate both the pace and geographic spread ofthe improvements, even in the context of weak healthsystems, by focusing on the collaborative efforts of QIteams that learn together.Supervision and monitoring: THNA provided initialcoaching and monitoring while simultaneously trainingstaff from the QI teams to undertake this role. Teamleads develop QI action plans with their team, agree onresponsibilities, and monitor and follow up on the team’sachievements and challenges. The approach encouragessupportive supervision instead of the previous punitiveapproach—for example, the QI collaborative transformednear-miss maternal death audits from a punitive to apositive QI approach, in which teams analyze the rootcauses of each case and introduce safeguards to preventthem in the future.“The QI approach encouraged supportive supervision.THNA explained expectations and worked closely with us.Before our system relied on orders. Now we explain, andthe team willingly accepts and implements the changes. Westopped punishments.”—Nurse, Shahritus HospitalShared learning: During learning sessions or exchangevisits between facilities, teams complete scorecards oneach other and provide useful feedback, accelerating theadoption of positive changes through an environment ofpositive competition.Building clinical competence: THNA uses mixedapproaches to strengthen clinical competencies, includingon-the-job training and simulation using anatomicalmodels as well as classroom training, on-the-jobmentoring, and supportive supervision. For hospitals,THNA trained 12 EPC, 10 IMCI, and 18 Kangaroo MotherCare master trainers. For PHCs, THNA built the capacityof 19 master trainers in nutrition in pregnancy, infant andyoung child feeding, management of anemia, and infectioncontrol. Master trainers are based at nutrition resourcetraining centers equipped by THNA at the 24 hospitalsand PHCs.“We almost lost a young mother to postpartumhemorrhage during a heavy shift with eight simultaneousdeliveries and Cesarean sections. A young woman wasbleeding from a perineal tear, sutured hastily, and wasalmost going into shock when we discovered her. Sincethen, we improved our compliance with the postpartumcare standard that requires us to check vital signs andvaginal bleeding every 15 minutes, for every delivery,including uncomplicated normal deliveries.”—Midwife, Dusti District HospitalLinking QI with the community: QI teams counselcommunities and work with health volunteers and peersupport groups (e.g., for mothers-in-law, young mothers,and men) to emphasize the value of ANC for the motherand baby. THNA also connects health workers at ruralfacilities with health volunteers who identify and referpregnant women not registered for ANC, those withdanger signs in pregnancy, and children with malnutritionand diarrhea.ResultsTable 1 presents data on QI collaborative interventions.Figure 2 shows progressive improvements at eighthospitals that regularly reported on four essentialindicators for EPC and EmONC. Figure 3 illustratesprogress reflected in EPC scorecards in 12 hospitals.Despite continuous improvements, no hospital reachedthe optimal score of 3, mainly due to low scores oninfrastructure indicators related to water supply andsewage systems. Figure 4 shows progress between thefirst baseline visit and second monitoring visit at the
screening. Appropriate anemia therapy is also notimproving quickly due to stock outs of iron supplementsat PHCs. Infection control improved in all locations wherecollaborative improvement strengthened mentoring andmonitoring systems; Figure 6 shows progress in hospitals.12 hospitals using the WHO IMCI scorecard. Figure 5documents marked improvements in ANC indicators atthe 12 PHCs. Screening for eclampsia showed slowerimprovement as some PHCs have no kits to testalbuminuria, one of the three measures for eclampsiaTable 1. Data on THNA clinical interventions, Year 4InterventionResultFacility health workers trained in nutrition counseling1,584Total number of health workers in FTF districts: 3,017590Total number of PHC providers in FTF districts: 2,394PHC providers trained in prevention and management ofanemiaChildren under five reached with clinical nutritioninterventionsDenominator50,000Total number of children under five in FTF districts:102,251Total number of pregnant women in FTF districts:52,162466Total number of maternity department workers: 51024Total number of central district hospitals and PHCs: 2432n/a13n/a27,000Pregnant women reached with clinical nutritioninterventionsTrainers and health workers trained in Kangaroo MotherCareNutrition resource training centers established at hospitalsand PHCsTopics/standards developed for on-the-job trainingPHCsHospitals19n/a1,497Total number of health workers in FTF districts: 3,017Doctors280Total number of doctors: 474Midwives161Total number of midwives: 268Nurses950Total number of nurses: 2,099Neonatal nurses51Total number of neonatal nurses: 86Pediatric nurses54Health workers receiving clinical on-the-job trainingObstetrics/gynecology and neonatology specialists trainedas trainers in supportive supervision for EPCPHC providers trained as trainers in supportive supervisionfor ANC and infant and young child feeding21Total number of pediatric nurses: 90Total number of hospital-level resource and trainingcenters: 12Total number of PHC-level resource and trainingcenters: 12Hospitals receiving equipment for IMCI and EPC12Total number of central district hospitals: 12Health fairs conducted to connect specialists to remoterural communities60Total number of THNA target communities: 50012Figure 2. Progress in EPC and EmONC at 12 hospitals, Jan. 2018-June 1%52%45%85%200Jan.2018June2018June2019% of correctlyfilled % of health workers observingthe rules of handwashingJan.2018June2018June2019June2020% of midwives correctlyperforming periodicauscultation of the fetusJan.2018June2018June2019June2020% staff readiness for EmONC(modeling)
Figure 3. Progress in EPC scores at 12 hospitals, May 2016-Feb. 20203.02.33May 2016May20172.01.341.0Sep. 2018Aug. 2019Feb. 2020Cohort ICohort II (1)(Q1-2, Y2)Cohort II (2)(Q3-4, 6Average2020Cohort III(Y3)Figure 4. Progress in IMCI scores at 12 hospitals between first (Oct. 2016-Nov. 2017), second (Feb. 2017- Aug.2018) and third (Jan-Feb. 2020) supportive supervision visits1st supportivesupervision visit542nd supportivesupervision visit3.42.9323rd supportivesupervision visitCohort ICohort II (1)(Q1-2, Y2)Cohort II (2)(Q3-4, Y2)Average,1st rd visitCohort III(Y3)Figure 5. Progress in ANC at 12 PHCs, Quarter 2, Year 2-Quarter 3, Year 5100806040200Q2Y2Q3Y4Q3Y5% of pregnant womenwho were registeredin the first trimesterQ2Y2Q3Y4Q3Y5% of pregnant womenwho were screenedfor eclampsiaQ2Y2Q3Y4Q3Y5Q2Y2% of pregnant womenwho received nutritioncounselingQ3Y4Q3Y5Q2Y2% of pregnant women whoreceived folic acid in thefirst trimesterQ3Y4Q3Y5% of pregnant womenwho received appropriateanemia treatmentFigure 6: Progress in infection control and clinical safety at 12 hospitals, Aug. 2017-Feb. 2020Aug. 201780%70%60%50%40%June 201848%May 2019Feb. 202030%20%Average,Aug. 2017Cohort ICohort II (1)(Q1-2, Y2)Cohort II (2)(Q3-4, Y2)Cohort verage,Feb. 2020
ChallengesRecommendations Although the Ministry of Health and Social Protectionof the Population has been introducing multiple QIinterventions at facilities, its overall strategy andapproach for QI is not firm yet. Multiple standardsand tools are being considered and used by differentdonors, which complicates roll out.While the ministry is interested in expanding QI forEmONC and IMCI in Khatlon region and nationally,budget limitations may inhibit sustainability and scaleup. Using evidence from its work, THNA is advocatingwith the Khatlon Department of Health and donorsto scale up the interventions.The training and capacity building provided throughTHNA has not been counted in terms of providers’continuing medical education (CME) achievements andrequirements. Multiple donors and partners face thesame issue and are advocating with the ministry toaccredit such trainings to motivate health workers toparticipate.Some hospitals and PHCs still lack running waterand sewage systems, presenting a major barrier toinfection control and quality of care.Postpartum care, although offered at the facilityafter delivery, remains almost absent once themother and newborn go home. This is mainly due toshortages of health workers in communities and longdistances from many communities to PHCs. Missedopportunities to provide family planning counselingand services also continue.Health facilities face shortages of essential medicinesand supplies, such as iron supplements and lab kits.Some essential ANC services, such as basic lab tests,are offered for a fee, which creates a barrier to accessfor most women. Scale up the clinical QI interventions: Theseapproaches resulted in remarkable qualityimprovements at minimal additional cost or effort tothe Ministry of Health and Social Protection of thePopulation, which makes the interventions ready forscale up. The QI collaborative is an excellent modelfor scaling up best practices, as it improves the inputs,the process, and the system of care. We recommendinitial scale up to additional hospitals and PHCs inKhatlon, since their situations and challenges are verysimilar. However, the ministry and donors need toagree on one approach to QI to accelerate progress.Involve the Department of Health in supportivesupervision and monitoring: This is essential forsustainability and scale up, as the QI teams needadditional stakeholder support to respond to some ofthe infrastructure needs and policy changes.Update the government CME system: The motivationof health providers to take part in clinical and QItraining activities would improve significantly if suchtraining brought a required CME credit.Ensure all hospitals and PHCs have runningwater and sewage systems: The government, localcommunities, private sector entities and donors needto prioritize this basic need.Strengthen postpartum care: Greater impact willbe achieved if postpartum care includes a mix ofhome visits by PHC midwives and health volunteersto check on mothers and newborns and providecounseling and referrals to facilities as needed.Integrate family planning services and counselingthroughout the continuum of care.Improve funding and supply chain for ANC: Ensureall basic ANC medicines and supplies, such as ironsupplements and urine albumin dipsticks are availableat the lowest level PHC facilities free of charge.Photo by Claudia Muir for IntraHealth InternationalThis technical brief is made possible by the generous support of the American people through the United States Agency for International Development (USAID)under the Feed the Future Initiative.The contents are the sole responsibility of IntraHealth International and do not necessarily reflect the views of USAID or theUnited States Government.CONTACTRoman YorickChief of Party,Tajikistan Health & Nutrition Activityryorick@intrahealth.org
Population is committed to improving the quality of maternal, newborn, and child health (MNCH) and nutrition services in hospitals and primary health centers (PHCs), as well as in communities. A government call to action to eliminate maternal deaths resulted in major progress, multiple quality improvement (QI) initiatives are